
From the 1Department of Physical Therapy, Mejiro University; present address: Department of Physical Therapy, Kobe International University, Kobe, 2Saitama Rehabilitation Center, 3Department of Occupational Therapy, Mejiro University, and 4Department of Physical Therapy, Ibaraki Prefectural University of Health Sciences, Ibaraki, Japan
Objective: To determine the usefulness of an un-stable board balance test in identifying a fall history among high-functioning community-dwelling elderly individuals.
Design: Case-control study.
Subjects: Sixty-one community-dwelling elderly aged ≥ 65 years and having the capacity to walk independently without an assistive device.
Methods: Subjects completed 3 balance performance tests: the Unstable Board Balance Test, Functional Reach Test, and Timed Up and Go. For analysis, subjects were classified as fallers or non-fallers based on the history of falls over the previous year, and performance outcomes were compared between the 2 groups. Subjects classified as fallers were then matched 1:1 with non-fallers (for sex, age, body weight and height), and the optimal cut-off score and area under the receiver operating characteristic curve (AUC) for each test were calculated.
Results: Functional reach test and Timed Up and Go did not reliably discriminate between fallers and non-fallers. In contrast, the score on the unstable board balance test was significantly different between the 2 groups (p = 0.040). Among all 3 tests, AUC was largest for the unstable board balance test (0.78), with superior sensitivity (0.67) and specificity (0.87).
Conclusion: For high-functioning elderly subjects, the unstable board balance test was useful in discriminating between fallers and non-fallers.
Key words: dynamic balance; assessment of falls; history of falls; elderly people.
Accepted Oct 8, 2018; Epub ahead of print Nov 8, 2018
J Rehabil Med 2019: 51: 00–00
Correspondence address: Kazunori Akizuki, Department of Physical Therapy, Kobe International University, 9-1-6 Koyouchou, Higasinada-ku, Kobe-shi, Hyogo 658-0032, Japan. E-mail: akizuki@kobe-kiu.ac.jp
The aim of this study was to determine the ability of an Unstable Board Balance Test to discriminate fall history in high-functioning community-dwelling elderly people. Subjects underwent an Unstable Board Balance Test, a Functional Reach Test (FRT), Timed Up and Go (TUG) measurement, and body height and body weight measurement. The age of subjects was determined and they were asked whether they had fallen within the past year. FRT and TUG did not differ significantly between fallers and non-fallers, but the Unstable Board Balance Test did show a significant difference between groups. We found that, in high-functioning elderly subjects, the Unstable Board Balance Test was able to detect elderly people with a fall history more accurately than either FRT or TUG.
It is estimated that one out of every 3 elderly individuals over the age of 65 years will experience one or more falls per year (1), resulting in health impairment of varying degrees of severity (2). In Japan, fall-related injuries are the fourth leading cause for elderly individuals requiring nursing care (3). As we consider the ageing of the general population globally (4), prevention of falls and fall-related injuries among the elderly population has become increasingly important.
Early identification of individuals at high risk of falls has been shown to be an effective strategy to reduce the occurrence of falls (5). Various clinical tools have been developed to identify individuals at high risk of falling (6). Of these, the Berg Balance Scale (BBS), the Timed Up and Go (TUG) and the Functional Reach Test (FRT) are widely used for their convenience and availability of cut-off values to identify those at risk of falling (7–10). The cut-off values (to differentiate fallers from non-fallers) for these tests, however, vary depending on individuals’ characteristics and the length of follow-up (11, 12). Moreover, the use of these tests in healthy, active, elderly individuals is limited due to a ceiling effect. In fact, both the BBS and TUG lack the specificity to identify a decrease in balance capacity predictive of a risk of falls among healthy, high-functioning, elderly individuals (13, 14). Therefore, there is a need for an assessment tool to detect changes in balance capacity that are predictive of falls in healthy, active elderly individuals.
Previous studies have shown that dynamic balance tests could be more appropriate than the BBS and TUG to differentiate the risk of falls among healthy, active, elderly individuals (15, 16). Thus, we developed the Unstable Board Balance Test for this purpose, anticipating that it would not be limited by the same ceiling effect of BBS or TUG in this population. The Unstable Board Balance Test was also designed to be portable and not restricted by the measurement environment, as well as providing objective, quantitative measures promptly. Therefore, the purpose of the current study was to determine the sensitivity and specificity of the Unstable Board Balance Test in differentiating individuals with a positive history for falls among a group of healthy, active, elderly individuals, and to compare the results with those from the TUG and FRT. If the Unstable Board Balance Test is valid in detecting slight reductions in the balance capacity of individuals with a fall history, then the test could be useful for early identification of those at risk of falls in the community, allowing for the opportunity to provide a falls prevention intervention.
In this study, we recruited elderly people living near the Iwatsuki Campus of Mejiro University, who attended the Saitama City Silver Resource Center between 28 February 2017, and 4 August 2017. The inclusion criteria were as follows: (i) age ≥ 65 years; (ii) living independently in the community; (iii) ability to walk independently, without an assistive device; and (iv) ability to visit the university facility where the study was conducted, without assistance. Individuals with a history of orthopaedic surgery that could affect balance or neurological diseases, as well as those with pain when performing the unstable board balance test and those with a Mini-Mental State Examination (MMSE) score < 24 were excluded.
In order to calculate the sample size required for the study, a preliminary survey of 29 subjects was performed. The effect size of the Medial-lateral Stability Index (MLSI), the primary outcome of the Unstable Board Balance Test, was 1.33, with a ratio of 5:24 between individuals with a history of fall (fallers) and those without a history of falls (non-fallers). Using G*power 3.1.9.2 software (17), the required sample size was calculated for an alpha value of 0.05 and power (1 – β) of 0.80. A sample size of 36 individuals (6 fallers and 30 non-fallers) was required. In order to control for confounding variables during the matching between fallers and non-fallers, we made the decision to recruit 58 individuals, to have at least 10 fallers and appropriate non-faller matched controls.
A preliminary explanation of the details of the study was given to all subjects, and written consent was obtained. The study protocol was approved by the institutional review board of Mejiro University (approval number 17-004).
This was a case-control study, with the following measures obtained for analysis: demographic and personal information (age, body height, body weight, history of falls over the past year) and balance performance outcomes (Unstable Board Balance Test score, the FRT and the TUG). The BBS was not included due to its previously reported ceiling effect for healthy, active, elderly individuals (13, 15). The measurement method for each balance performance test is described below.
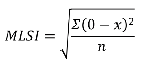
Unstable Board Balance Test. All tests were performed using the DYJOC unstable board (SAKAI Medical Co. Ltd, Tokyo, Japan). The DYJOC board has a dimension, of 300 × 500 × 30 mm with 2 semi-circular bosses (φ160 × 60 mm) attached to the rear of the platform. For this study, the 2 bosses were attached to restrict the tilt movement to the medial-lateral (ML) direction (Fig. 1), as allowing unrestricted movement in all directions makes the task too difficult to complete for elderly individuals. In addition, blocks were inserted on either side of the board to allow a maximum tilt angle of 12° (Fig. 2). The board was fitted with a small 3-axial accelerometer and a 3-axial gyroscope (multi sensor θ, SAKAI Medical Co. Ltd) to measure the tilt degree and the acceleration. The data were transmitted to a personal computer via a dedicated data logger (Data Logger, SAKAI Medical Co. Ltd). The MLSI was calculated using analysis software (MS DYJOC, SAKAI Medical Co. Ltd), as follows:
where x is the degree of tilt of the board in the ML plane and n the number of samples (sampling frequency, 100 Hz). Because the given stability index reflects the change in the inclination of the unstable board per unit time, a larger value indicates a greater degree of fluctuation in ML balance control.
Subjects were instructed to stand on the board, with feet at shoulder width and arms along the side of the body, and to maintain the position of the unstable board as parallel to the floor as possible. Subjects were asked to fix their gaze on a focal point placed 1 m in front of them, which was adjusted to eye level for each subject. All measurements were obtained without shoes. Each subject completed 3 20-s trials.
Fig. 1. The unstable board used in this study. (a) Top surface, (b) bottom surface.
Fig. 2. Tilt angle adjustment method. The maximum tilt angle was limited to 12° by placing a 2.5-cm plate on both sides of the board.
Functional reach test (FRT). The subject was instructed to stand sideways along a wall, to which a measuring tape was affixed, with the arm closest to the wall at 90° of shoulder flexion. In this standardized standing position, the location of the tip of the third finger along the tape measure was recorded. Subjects were then instructed to reach as far forward as possible, without taking a step, and the location of the tip of the third finger was recorded at the furthest distance reached to. The distance between the 2 marks was recorded as the functional reach distance (cm). Each subject completed 2 trials, with the maximum FRT distance obtained using in the analysis. The criterion validity, predictive validity, test-retest reliability, and inter-rater reliability for the FRT, for younger and older adults, has been described previously (18, 19).
Timed Up and Go (TUG). The following instructions were provided to subjects: “When I say ‘go’, stand up from the chair using the armrest, walk 3 m, straight ahead, at a comfortable speed, up to the cone, turn and return to the chair, and sit down. I will record the time taken for you to complete the task, from the time you stand up from the chair to when you return to a sitting position.” Subjects completed 1 practice trial, with feedback provided as needed, and subsequently performed the actual TUG for recording. The time to complete the TUG was measured using a stopwatch, and one examiner performed all assessments. High inter- and intra-examiner reliability were previously reported for the TUG in elderly individuals (20). In addition, the TUG has concurrent validity with gait speed, the BBS, and the Barthel Index (20).
Recent fall history. For the purpose of this study, a “fall” was defined as “an unexpected event in which the subject came to rest on the ground, floor or a lower level” (21). Subjects were asked to report the number of falls they had experienced over the previous year. We excluded falls resulting from extraordinary environmental factors.
For analysis, subjects were divided in a “faller” and “non-faller” group, according to their self-reported falls history. Demographic, personal and performance scores were compared between the 2 groups, using a χ2 test for the categorical variable (sex) and an independent sample t-test for continuous variables. Subsequently, subjects in the faller group were matched 1:1 to subjects in the non-faller group for sex, age (± 5 years), height (± 5.9 cm for men and ± 5.1 cm for women) years, and body weight (± 7.5 kg for men and ± 6.8 kg for women), to control for the effects of these variables on test scores. The allowed ranges were defined based on known standard deviations for men and women, 70–74 years of age, published by The Ministry of Education, Science, Sports and Culture of Japan (22).
For each performance test, a receiver operating characteristic (ROC) curve was calculated and the area under the curve (AUC) used to determine the accuracy of the test in differentiating fallers from non-fallers, with the AUC interpreted as follows: AUC ≥ 0.9, high accuracy; AUC between 0.7 and 0.9, moderate accuracy; and AUC between 0.5 and 0.7, low accuracy (23). The optimal cut-off value to differentiate between the 2 groups was calculated for each performance test using Youden’s index. The sensitivity, specificity, positive likelihood ratio (PLR), and negative likelihood ratio (NLR) for identified cut-off values were calculated to determine the discrimination precision for each performance test with regard to fall history, with a PLR > 5 and NLR < 0.2 indicating that the test would be clinically useful, having a high probability of correctly identifying subjects with and without history of falls (24).
All analyses were performed using IBM SPSS Statistics software (version 24), with significance level p < 0.05.
Of the 66 subjects who satisfied the inclusion criteria, 2 were subsequently excluded because of a diagnosis of knee osteoarthritis, 2 because of an acute onset back pain, and 1 who had undergone total knee replacement with the previous year. The demographic and personal attributes of the 61 subjects included in the analysis, as well as their performance scores are summarized in Table I, with between-group differences on measured variables reported in Table II. The faller and non-faller groups were comparable with regard to the distribution of age and body weight, but with a greater proportion of women in the faller than non-faller group (p = 0.007); and, with a greater proportion of men, subjects in the non-faller group were taller than those in the faller group (p = 0.045). The MLSI was significantly larger for the faller than non-faller group (p = 0.040, Cohen’s d = 1.363), but with no between-group difference for the FRT (p = 0.168, Cohen’s d = 0.512) or TUG (p = 0.492, Cohen’s d = 0.254).
Table I. Subjects’ characteristics
Table II. Comparison of variables between the faller and non-faller group (n = 61)
Between-group differences on the balance performance tests, after matching between the faller and non-faller groups, are reported in Table III. During the matching process, 1 subject was excluded from the faller group because a matched control in the non-faller group could not be identified; data for 8 subjects in the faller group and 8 in the non-faller group were included in the analysis. Even after matching, a significant between-group difference was identified only for the Unstable Board Balance Test (p = 0.016, Cohen’s d = 1.468), with no difference for the FRT (p = 0.478, Cohen’s d = 0.390) or TUG (p = 0.268, Cohen’s d = 0.617).
Table III. Comparison between the “faller” and “’non-faller” groups after matching (n = 16)
Fig. 3 shows the ROC curve for each balance performance score, with the optimal cut-off value, AUC sensitivity, specificity, PLR, and NLR for each reported in Table IV. The AUC was greater for the Unstable Board Balance Test (0.78), compared with the FRT (0.64) and TUG (0.54). In addition, the cut-off values calculated from the ROC curve were 8.6° for the Unstable Board Balance Test (sensitivity 0.67; specificity 0.87; PLR 4.95; NLR 0.39), 30.7 cm for the FRT (sensitivity 0.78; specificity 0.50; PLR 1.56; NLR 0.44) and 7.3 s for the TUG (sensitivity 0.33; specificity 0.94; PLR 5.78; NLR 0.71).
Fig. 3. Receiver operating characteristic (ROC) curves for identifying a recent fall.
Table IV. Characteristics of each test
This study examined the comparative usefulness of the Unstable Board Balance Test, FRT and TUG to differentiate fallers from non-fallers among a group of health and high-functioning, community-dwelling, elderly individuals. The TUG and FRT are commonly used in clinical practice (and research) for the assessment of balance control, both of which can be assessed rapidly. The BBS was not used due to its ceiling effect, with healthy, active, individuals achieving the maximum score (13, 15). As our group of interest was healthy community-dwelling elderly individuals, we set our inclusion criteria to persons who could walk independently, without an assistive device, and could visit the facility for assessment by themselves. These criteria allowed us to recruit a group of high-functioning individuals for whom existing fall assessment tests (TUG and FRT) could not discriminate the fall risk. Among study group, 14.8% of subjects had experienced a fall over the previous year, an incidence rate which was lower than previously reported (25). We do need to consider that individuals might have selected to not report a fall, due to pride or embarrassment (26), resulting in some fallers being included in the non-faller group. Regardless of this potential error, the TUG and FRT could not reliably discriminate between fallers and non-fallers. In a previous study, standard values (calculated from a meta-analysis) of 8.1 s have been reported for individuals 60–69 years of age, and 9.2 s for those 70–79 years of age (27), with values for subjects in our study being comparable to these standard values. However, the FRT value for our study group was greater than the standard value previously reported for elderly individuals of 29.4 cm (28). The high function of our study group probably explains the inability of the FRT and TUG to differentiate between fallers and non-fallers. However, despite being high functioning, 14.8% of the people had experienced a fall within the past year, a finding which is consistent with the rate of fall previously reported in healthy and high-functioning elderly individuals (16, 29). Of note, the Unstable Board Balance Test reliability discriminated between fallers and non-fallers, and this in the absence of any self-reported difficult with walking.
The current study demonstrates that the MLSI can discriminate between fallers and non-fallers, which was not possible using the TUG or FRT. Moreover, matching increased the effect size of discrimination for the MLSI and TUG, but decreased the effect size of the TUG. With regard to the generalizability of our finding, it is important to note the greater proportion of women in the faller (78%) than non-faller (31%) group. This difference in the proportion of sex across the 2 groups also biased the physical attributes between the 2 groups, height specifically, which can influence outcomes, in addition to age (27, 28). While the effect size for each test was modified by matching, the MLSI consistently maintained a higher effect size than for the TUG and FRT. Thus, the ability of the MLSI to discriminate between fallers and non-fallers was unaffected by age and the physical attributes of subjects, with the discriminating value for the MLSI being greater than the moderate accuracy previous reported for other fall assessments that have been used in the community (15, 30). Thus, we believe that the Unstable Board Balance Test might be superior in its ability to detect fall risk among healthy, high-functioning, elderly people. The inclusion of the unstable board balance test should be considered in future comparative studies.
The MLSI reflects the left-right tilt angle of the unstable board during the balance task, requiring maintaining the position of the centre of pressure (COP) in centre of the board being required to decrease the MLSI. Previous studies have demonstrated the reliability of using COP measurement to detect small decreases in balance capacity, which could not be detected by functional balance tests, such as the BBS (31–34). Maki et al. (34) reported that, while the anterior-posterior sway was larger in fallers than non-fallers, the ML component of COP displacement provided the best prediction of falls. In addition, Melzer et al. (35) reported a significant increase in ML sway (during narrow-base standing) among elderly individuals who have experienced falls compared with those with no fall history. Using COP measurements, previous studies have shown that tasks incorporating dynamic elements, such as a perturbation or leaning movement, provide a better discrimination of small decreases in balance capacity than static balance tasks, with age-related degradation occurring early for dynamic than static balance tasks (35–39). Thus, balance tasks with dynamic elements would be more effective in challenging balance capacity than static standing tasks (40). Therefore, measuring MLSI using an unstable board, which therefore includes a dynamic element, might be an effective method for early detection of a decrease in the balance ability of high-functioning elderly individuals.
Although COP measurements using a force platform, there are various limitations in using force platforms in the community-dwelling, including the prohibitive cost of devices and poor portability. In contrast, the Unstable Board Balance Test used in our study provided a dynamic balance task that was effective in discriminating fallers and non-fallers among healthy, high-functioning, community-dwelling individuals, while providing the low cost and portability that are not available with force platforms. Therefore, this balance board can be easily used in various environments and not only in a laboratory, and it provides easy-to-interpret outcomes.
This study has a few limitations that need to be acknowledged. First, because of the case-control design of the study, the predictive capacity of the MLSI for falls could not be evaluated, and thus, prospective studies are needed in this respect. Furthermore, the study group was rather homogeneous with regard to physical characteristics, age, and function, and therefore, it is unclear to which extent elderly individuals with different demographic and personal characteristics could complete the task. The usefulness of the assessment for individuals with different levels of functioning remains to be determined (29), thereby refining the MLSI for accurate detection of the risk of falling among elderly individuals.
The Unstable Board Balance Test was useful in discriminating between fallers and non-fallers, which was not possible using the FRT and TUG. Based on our results, we suggest that the Unstable Board Balance Test could be useful for early detection of elderly individuals at risk of falling, and allowing timely fall prevention programmes to be implemented.
The authors would like to thank the subjects in this study. This work was supported by JSPS KAKENHI Grant Number JP 18K17763.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize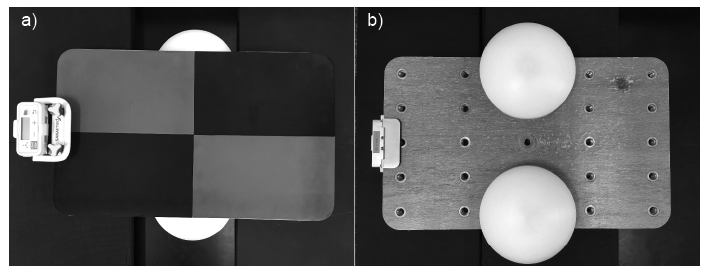 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize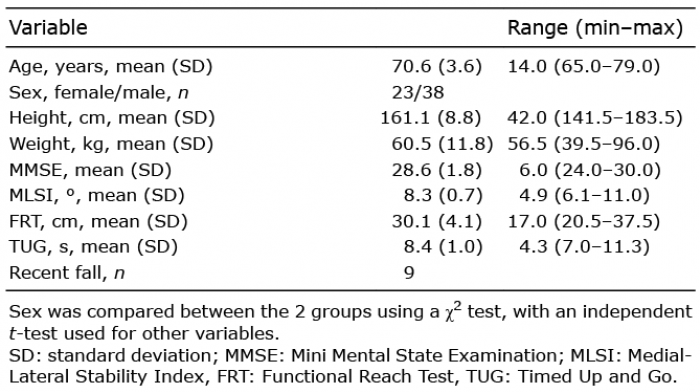 Click to show fullsize
Click to show fullsize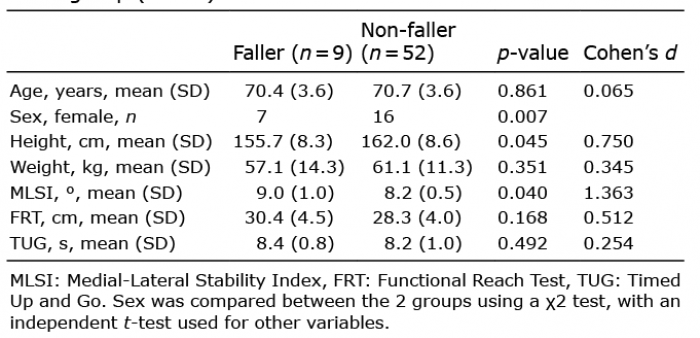 Click to show fullsize
Click to show fullsize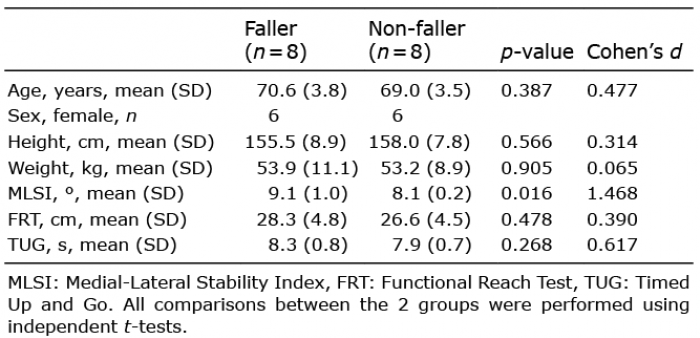 Click to show fullsize
Click to show fullsize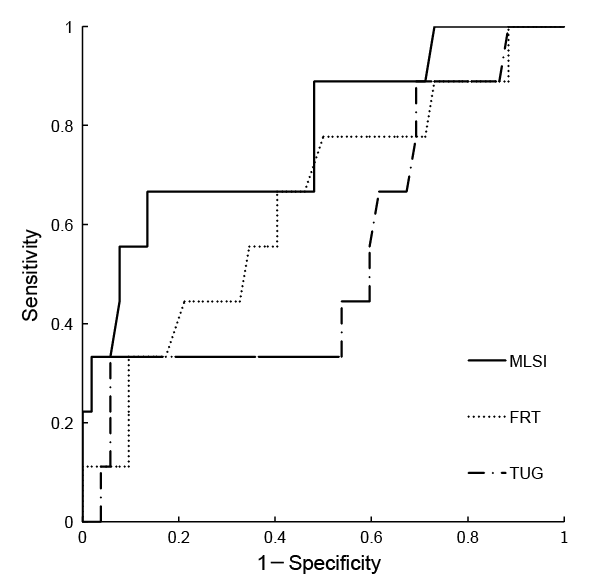 Click to show fullsize
Click to show fullsize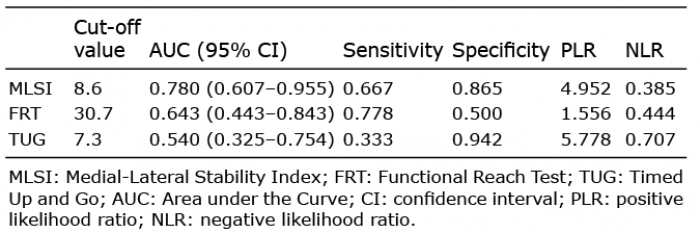 Click to show fullsize
Click to show fullsize