
From the 1Department of Public Health and Nursing, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, Trondheim, 2Unicare Helsefort Rehabilitation Centre, Rissa, 3Department of Physical Medicine and Rehabilitation, St Olavs Hospital, Trondheim University Hospital and 4Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, Trondheim, Norway
Objectives: To assess: (i) whether changes in the Fear-Avoidance Beliefs Questionnaire (FABQ) were greater for multicomponent inpatient rehabilitation vs outpatient cognitive behavioural therapy, and (ii) whether baseline scores and changes (pre- to post-intervention) in FABQ were associated with future work-participation.
Methods: Individuals sick-listed for 2–12 months were randomized to inpatient multicomponent rehabilitation (3.5 weeks or 4+4 days) or outpatient cognitive behavioural therapy (6 sessions/6 weeks).
Results: A total of 334 subjects were included. There were no significant differences on FABQ between the in- and out-patient programmes during follow-up. Participants with consistently low scores on the work subscale had more work-participation days, followed by those who reduced their scores. Participants who increased, or had consistently high scores had the least workdays. For the physical activity subscale, the associations were weaker. FABQ-work scores at baseline were associated with number of work-participation days for both musculoskeletal and psychological diagnoses, and more strongly for the latter group.
Conclusion: This study suggests that FABQ could be a useful prognostic tool for individuals on sick leave due to musculoskeletal or psychological disorders. There was no evidence that inpatient occupational rehabilitation reduces FABQ scores more than outpatient cognitive behavioural therapy.
Key words: return to work; sick leave; musculoskeletal diseases; mental health.
Accepted Jan 15, 2019: Epub ahead of print Feb 15, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Lene Aasdahl, Norwegian University of Science and Technology, NTNU, Department of Public Health and Nursing, Faculty of Medicine and Health Sciences, Postboks 8905, MTFS, 7491 Trondheim, Norway. E-mail: lene.aasdahl@ntnu.no
Psychological factors are important in sick-listed workers’ return to work process. The fear-avoidance model suggests that negative beliefs about pain and its consequences may lead to catastrophizing thoughts and avoidance of activities believed to be harmful or to worsen the pain. This study evaluated whether the Fear-Avoidance Beliefs Questionnaire (FABQ), was associated with future work outcomes for sick-listed workers in occupational rehabilitation. FABQ is traditionally used for individuals with low-back pain, but this study also used it for individuals with common mental health disorders. The results suggest that the FABQ could be a useful prognostic tool for individuals on sick leave due to both musculoskeletal and psychological disorders.
Psychological factors are important in prevention of disability and promotion of return to work (RTW) (1). One model to explain how psychological factors influence disability in patients with low-back pain is the fear-avoidance model (2, 3). This model describes how negative beliefs about pain and its consequences may lead to catastrophizing and avoidance of activities believed to be harmful or to worsen the pain, which again may lead to inactivity and reduced functioning (3). One of several questionnaires developed to measure fear-avoidance beliefs is the Fear-Avoidance Beliefs Questionnaire (FABQ) (4), consisting of 2 subscales: work and physical activity.
High fear-avoidance beliefs have repeatedly been associated with lower RTW rates (5–7). However, few studies have evaluated whether RTW interventions reduce fear-avoidance beliefs (8). A recent study of patients with neck or back pain participating in a multidisciplinary intervention found no difference in FABQ scores within 4 months follow-up between interventions with added work-focus vs conventional rehabilitation (9). However, with reduced FABQ-work scores (12 points or more) the odds for RTW increased at 12 months of follow-up.
The FABQ was developed for patients with low-back pain. However, avoidance of activities believed to be harmful by the patient, as described in the fear-avoidance model, is not specific for low-back pain. Hence, the physiological responses seen in patients with back pain have common features with responses seen in anxiety and depression disorders (3). There is also considerable overlap in symptoms between different diagnoses, such as back pain, anxiety and depression (10, 11). Øyeflaten et al. (6) found that FABQ was a prognostic factor for RTW in a group of participants with mixed diagnoses. However, we are not aware of studies that used the FABQ specifically for psychological disorders.
In Norway, there is a long tradition of offering inpatient occupational rehabilitation to patients with different diagnoses, mainly musculoskeletal complaints, anxiety, depression and unspecific diagnoses. We recently evaluated the effects of 2 inpatient occupational rehabilitation programmes. Both were compared with an outpatient programme consisting of group-based cognitive behavioural therapy (12, 13). One of the inpatient programmes (3.5 weeks) enhanced RTW compared with the outpatient programme [14] (personal communication), while the other (4+4 days) had no effect on RTW (13).
The present study evaluated whether inpatient occupational rehabilitation reduced fear-avoidance beliefs more than outpatient cognitive behavioural therapy. As the inpatient programmes were more comprehensive and included several work elements intended to reduce fear-avoidance beliefs about work (e.g. work-related problem solving) and physical activity (e.g. supervised exercise sessions), it was hypothesized that the inpatient programmes would reduce fear-avoidance beliefs more than the outpatient programme. Furthermore, we assessed whether baseline scores and changes (pre- to post-intervention) in FABQ were associated with future work-participation.
This study is based on data from 2 randomized clinical trials. Both trials were designed with parallel groups (Fig. 1) (12). The first trial compared a short inpatient multicomponent occupational rehabilitation programme (4+4 days) to a less comprehensive outpatient programme (6 sessions during 6 weeks) (hereafter referred to as the short inpatient and outpatient programmes, respectively) for individuals on sick-leave due to musculoskeletal, unspecific, or common mental health disorders. The second trial compared a long inpatient programme (3.5 weeks) with the same outpatient programme (hereafter referred to as the long inpatient and outpatient programme, respectively). The primary outcome was sickness absence days. The study protocol and results from one of the randomized trials have been published, and the description of the methods is partly overlapping with previous studies (12, 13, 15). The study was approved by the Regional Committee for Medical and Health Research Ethics in Central Norway (no.: 2012/1241), and is registered in clinicaltrials.gov (no.: NCT01926574).
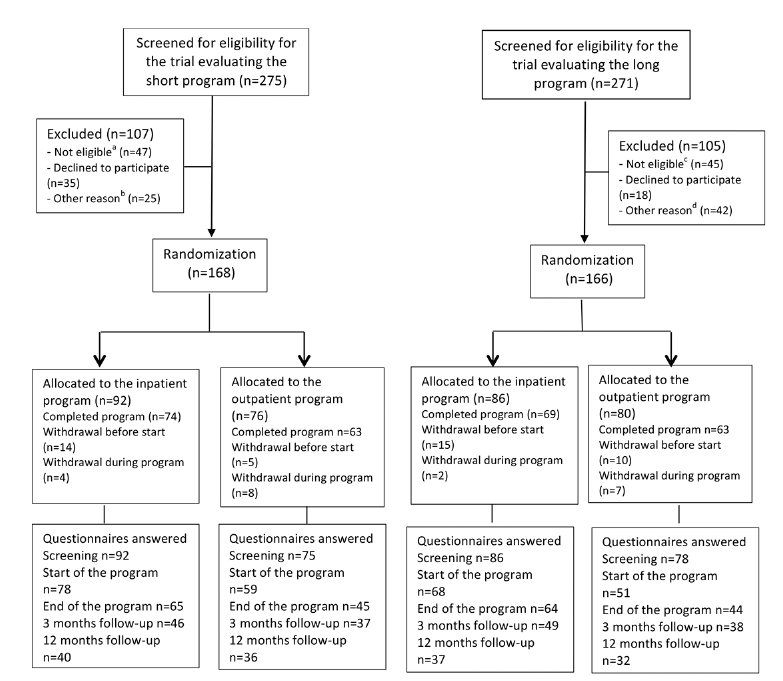
Fig. 1. Flow of participants in the study. aNot eligible: serious somatic/psychiatric illness (n = 20), a specific disorder requiring specialized treatment (n = 10), currently participating in another treatment programme (n = 15), insufficient Norwegian comprehension (n = 1), scheduled surgery next 6 months (n = 1). bOther reason: not met (n = 10), medical assessment not completed (n = 8), not motivated (n = 5), no longer on sick-leave (n = 2). cNot eligible: participating in another treatment programme (n = 22), serious somatic/psychiatric illness (n = 11), specialized treatment needs (n = 4), problems with functioning in groups (n = 3), surgery scheduled next 6 months (n = 2), insufficient language skills (n = 2), alcohol/drug abuse (n = 1).
dOther reason: medical assessment not completed (n = 15), no longer on sick-leave (n = 10), not motivated (n = 6), inability to participate in an inpatient intervention (n = 7), unknown (n = 4).
Eligible participants were aged 18–60 years, and sick listed 2–12 months with a diagnosis within the musculoskeletal (L), psychological (P) or general and unspecified (A) chapters of the International Classification of Primary Care, second edition (ICPC-2). The current sick-leave status at inclusion had to be at least 50% off work. Sick-listed individuals fulfilling the inclusion criteria were identified in the Social Security Registry and randomized to receive an invitation to either the long or the short trial. Invited participants completed a short initial questionnaire assessing eligibility. Those eligible were invited for an outpatient screening assessment. Exclusion criteria were: (i) alcohol or drug abuse; (ii) serious somatic (e.g. cancer, unstable heart disease) or psychological disorders (e.g. high risk of suicide, psychosis, ongoing manic episode); (iii) disorders requiring specialized treatment; (iv) pregnancy; (v) currently participating in another treatment or rehabilitation programme; (vi) insufficient oral or written Norwegian language skills to participate and benefit from group sessions and complete questionnaires; (vii) scheduled for surgery within the next 6 months; or (viii) serious problems with functioning in a group setting.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
The inpatient programmes consisted of group-based acceptance and commitment therapy (ACT) (16), a form of cognitive behavioural therapy (third-generation), individual and group-based physical training, mindfulness, education on various topics, and individual meetings with the coordinators in work-related problem-solving sessions and creating a RTW plan. One programme lasted 3.5 weeks and the other 4+4 days (with 2 weeks at home in-between).
The outpatient programme, which was identical in the 2 trials, consisted mainly of group-based ACT once a week for 6 weeks, each session lasting 2.5 h. The common component for the inpatient and outpatient programmes was ACT, in which the aim was to facilitate RTW through increased psychological flexibility (17), which presumably would increase self-efficacy and RTW expectations. A more detailed description of the programmes has been published previously (12).
Questionnaires. Self-reported data on fear-avoidance beliefs and other questionnaires were collected via web-based questionnaires answered at screening before inclusion (baseline, T0), at the start (T1) and the end of the programme (T2), and at 3 months (T3) and 12 months (T4) of follow-up after the end of the programmes.
Fear-avoidance beliefs were recorded using the FABQ (4). It consists of 2 subscales: (i) a 7-item work subscale (FABQ-Work, range 0–42 points), and (ii) a 4-item physical activity subscale (FABQ-Physical activity, range 0–24 points). To make the questionnaire usable for participants with other complaints than back pain, “complaints” replaced “pain” and “body” replaced “back”. There are no established cut-offs for minimal detectable change in FABQ, but 12 points have been suggested for the work subscale and 9 for the physical activity subscale (18).
Other variables registered by questionnaires at the start of the rehabilitation programmes were anxiety and depression symptoms (measured using the Hospital Anxiety and Depression scale (HADS) (19)), mean pain last week, level of completed education (dichotomized as high (college/university) or low) and employment status (dichotomized as having a current job, or not).
Sick leave was measured using data from the Norwegian National Social Security System Registry. All individuals receiving any form of sickness or disability benefits in Norway are registered by their social security number. The data consisted of all individual registrations of periods with any medical benefits.
Work participation was measured as the number of days not receiving medical benefits during 9 months of follow-up after the end of the rehabilitation programmes. It was adjusted for graded sick leave, employment fraction, and calculated as a 5-day work-week, yielding 196 possible working days.
If the outpatient screening was passed, the second randomization allocated the participant to either the inpatient or the outpatient programme (Fig. 1). A project co-worker performed the first randomization. In the second allocation, a flexibly weighted randomization procedure was provided by the Unit of Applied Clinical Research (third-party) at the Norwegian University of Science and Technology (NTNU), to ensure that the rehabilitation centre had enough participants to run monthly groups in periods of low recruitment.
It was not possible to blind the participants or the caregivers for treatment. The researchers were not blinded.
Sample size was calculated based on the primary outcome, i.e. number of sickness absence days, resulting in 80 persons in each arm (12).
Linear mixed-effects models were used to compare scores on the FABQ-work and physical activity subscale over time between the inpatient and outpatient programme, separately for the 2 trials. In addition to programme and time, an interaction term between programme and the 5 time-points (T0–T4) was included in the analyses to assess whether the effects of the programmes differed over time. A random intercept for person was included in the models to allow the participants to start at different levels. The main analyses were not adjusted for baseline characteristics, but the sensitivity analysis was adjusted for sex, age and education level to assess the robustness of the results. In a second sensitivity analysis, a per protocol analysis was performed, excluding participants who withdrew after randomization and/or attended less than 60% of the sessions in the outpatient programmes.
To assess whether changes in fear-avoidance beliefs during rehabilitation were associated with work-participation days linear regression was used. The 2 FABQ subscales were dichotomized into low risk and moderate/high risk using the cut-offs recommended by Wertli et al. (7). For the FABQ-work subscale a score of less than 21 was categorized as low risk and for the physical activity subscale a score of less than 14 was categorized as low risk. Based on the 2 categories, the participants were classified into 4 groups (for the 2 subscales separately) based on their scores at the start (T1) and the end of the rehabilitation programmes (T2): (i) consistently low fear-avoidance beliefs; (ii) increasing from low to high scores; (iii) decreasing from high to low scores; and (iv) consistently high fear-avoidance beliefs. The new categorical variable was included in the regression analyses. The analyses were performed both unadjusted and adjusted for age, sex and education. In addition, a sensitivity analysis adjusting for intervention programme was performed (in addition to the aforementioned variables). All analyses were performed separately for the 2 FABQ subscales. To evaluate the association between FABQ at baseline (T0) and future work participation for the different diagnosis groups, linear regression was used and the analyses performed separately for participants with musculoskeletal diagnoses and psychological diagnoses. As there were few participants with unspecific diagnoses (chapter A in ICPC-2) they were not included in these analyses. For the association analyses, participants from both trials were included.
p-values (2-tailed) < 0.05 were considered statistically significant. Precision was assessed using 95% confidence intervals (95% CI). All analyses were performed using STATA 14.1 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX, USA: StataCorp LP).
The flow of participants through the 2 trials is illustrated in Fig. 1. After screening, 168 participants remained in the short trial and were randomized to the short inpatient programme (n = 92) or the outpatient programme (n = 76). In the long trial, 166 participants were included and randomized to the long inpatient programme (n = 86) or the outpatient programme (n = 80). The number of people who answered the questionnaires decreased steadily through the study (Fig. 1).
The mean age of the participants was 45 years and most were women (79%). Approximately half had a musculoskeletal sick-leave diagnosis (54%), while 37% had a psychological diagnosis, and 9% a diagnosis from the general and unspecified chapter of ICPC-2. Most participants (65%) worked full-time before they were sick-listed, 18% worked part-time, 12% did not have employment, and 5% had a graded disability pension. The median number of sickness absence days at inclusion was 217 (interquartile range (IQR) 179–268). Baseline characteristics of the participants in the intervention vs the comparator were similar in both trials (Table I).
Table I. Baseline characteristics of participants
There was no statistically significant difference in the short trial between the 2 programmes in fear-avoidance beliefs from baseline to 12 months of follow-up, for either FABQ-work scores (1.82, 95% CI –2.19 to 5.83) or FABQ-physical activity scores (1.36, 95% CI –0.75 to 3.47). Both programmes showed a reduction in scores for both the work and physical activity subscales during follow-up (Fig. 2). Similarly, in the long trial there was no statistically significant difference between the 2 programmes on FABQ-work (1.14, 95% CI –2.94 to 5.22) or FABQ-physical activity (0.08, 95% CI –2.51 to 2.67). Also in the long trial, both programmes showed a reduction for both subscales (Fig. 2). Neither of the sensitivity analyses changed the findings (results not shown).
Fig. 2. Fear Avoidance Beliefs Questionnaire (FABQ) scores for the 2 programmes in the short and long trial during follow-up. Data are estimated means with 95% confidence intervals for: (a) FABQ work in the short trial, (b) FABQ work in the long trial, (c) FABQ physical activity in the short trial, and (d) FABQ physical activity in the long trial. Analyses performed with linear mixed-effects models.
There was an association between changes in the FABQ-work subscale scores from the start to the end of the rehabilitation programmes and work-participation days during 9 months of follow-up (Table II). Participants with consistently low scores had the most work-participation days (149 days (95% CI 136–162)), while those with consistently high scores had 57 days less (95% CI –77 to –37). Of 163 participants who answered the questionnaire at both the start and the end of the programme, 20 reduced their FABQ-work scores. These participants had 23 fewer work days (95% CI –52 to 5) than those with consistently low scores, while those increasing their scores had 54 fewer work days (95% CI –89 to –18).
Table II. Associations between changes in scores on the Fear Avoidance Beliefs Questionnaire (FABQ: work and physical activity) before and after rehabilitation with work participation during 9 months’ follow-up
For the FABQ-physical activity subscale, there was a weaker association between changes in FABQ-scores and work participation during follow-up (Table II). Participants who reduced their FABQ-scores had 22 fewer work days (95% CI –54 to 11) than those with consistently low scores, while those increasing their scores had 15 fewer days (95% CI –46 to 16). Those with consistently high scores had 41 fewer work days (95% CI –69 to –12).
The sensitivity analyses including adjustment for intervention programme in addition to age, sex and education, showed similar results (results not shown).
Participants with psychological diagnoses had lower scores than those with musculoskeletal diagnoses on both FABQ-subscales at baseline (mean 18.7 (SD 10.7) vs 23.1 (SD 11.7) for FABQ-work and mean 5.8 (SD 6.5) vs 11.0 (SD 6.4) for FABQ-physical activity, respectively). Of participants answering the FABQ at both baseline and 12 months of follow-up, 74% with a psychological diagnosis and 63% of those with a musculoskeletal diagnosis, reduced their FABQ-work score. For the physical activity subscale, the numbers were 45% and 67%, respectively. The mean reduction in fear-avoidance beliefs for work was 7.0 (SD 11.7) for psychological diagnoses and 4.8 (SD 11.1) for the musculoskeletal diagnoses. For the physical activity subscale the numbers were 1.4 (SD 5.6) and 3.0 (SD 5.3), respectively.
FABQ-work scores at baseline were associated with number of work-participation days during 9 months of follow-up for both musculoskeletal and psychological diagnoses (Table III). The association was stronger, and explained variance was larger, for psychological diagnoses (0.16 vs 0.08). Baseline scores for the physical activity subscale were associated with work-participation days for those with psychological diagnoses, but not for musculoskeletal diagnoses. The explained variance was small for both groups (< 0.01) for this subscale.
Table III. Associations between participants’ fear-avoidance beliefs at baseline and number of work-participation days during 9 months of follow-up, for musculoskeletal and psychological diagnoses
Participants with missing questionnaires at 12 months were somewhat younger (mean age 44 years (SD 9.6) vs 48 years (SD8.2)), and more likely to be men than women (66% vs 54%). Baseline scores for the 2 FABQ subscales were similar for those not responding and those responding (work subscale 22.0 (SD 11.6) vs 20.5 (SD11.3); physical activity subscale 9.4 (SD 6.9) vs 8.2 (SD 6.6)).
The median number of work-participation days during follow-up was similar for participants who answered the FABQ at both the start and the end of the programmes compared with those answering only at one time-point, and thus were excluded from the analyses (work subscale 123 days (IQR 81–182) vs 116 days (IQR 64–178); physical activity subscale (119 days (IQR 70–180) vs 125 days (IQR 69–178)).
There were no differences in fear-avoidance beliefs about work or physical activity between inpatient occupational rehabilitation and outpatient cognitive behavioural therapy during 12 months of follow-up. The change in FABQ-work during the programmes was associated with the number of work days during 9 months of follow-up. For FABQ-physical activity, the association with future work participation was weaker. The association between fear-avoidance beliefs at baseline and future work participation was stronger for those with psychological complaints than for those with musculoskeletal complaints.
The lack of additional effect of the inpatient programmes on fear-avoidance beliefs was not in line with our hypothesis. However, the results are in line with a previous study comparing effects of work-focused and standard rehabilitation on FABQ (9). FABQ was reduced after all the programmes in our study, but the reductions were smaller than the suggested minimal detectable change (18). This was surprising, as the inpatient programmes included physical activity designed to reduce fear of movement. Fear-avoidance beliefs about work were targeted by work-related problem solving through group discussions and creating an individual RTW plan. It is possible that graded work exposure at the workplace could have been more effective. However, the participants had been sick-listed for approximately 7 months on average; hence changing their fear-avoidance beliefs could be difficult. Another possible explanation is the use of ACT as the cognitive behavioural therapy. A key component in ACT is acceptance, meaning that participants are encouraged to acknowledge and accept their symptoms rather than try to control them. This could result in participants accepting, and thus reporting, more fear-avoidance beliefs after participating in the programme than they otherwise would, which might explain the small reductions observed (20). This might explain why one of the inpatient programmes was successful in terms of RTW despite small changes in fear-avoidance beliefs. Conversely, previous studies have suggested that the responsiveness of the FABQ might be low (18, 21), which should be evaluated further in future research.
The results of the current study indicate that using a cut-off between low-risk and medium/high-risk patients could be useful to predict whether patients will RTW. The cut-offs recommended by Wertli et al. (7) were used. These cut-offs are widely used in Norway, as they are included in the Norwegian neck and pain registry, used at back- and neck-pain clinics at all university hospitals. We are not aware of previous studies assessing the association between FABQ and future work participation using these cut-offs. Our findings are in line with a study by Staal et al. (22) reporting that participants with high fear-avoidance beliefs (median-based cut-offs: work 26; physical activity 16) returned to work more slowly than those with low scores. Due to the limited number of participants, it was not possible to differentiate between medium- and high-risk patients in the present study, and this should be done in future studies. As FABQ-work measures fear-avoidance beliefs about work specifically, it is not surprising that this subscale had a stronger association with future work participation than the physical activity subscale.
Øyeflaten et al. (6) found FABQ-work to be a strong predictor for RTW in a group of participants with mixed diagnoses (musculoskeletal, psychological and unspecific diagnoses). However, we are not aware of studies evaluating the FABQ separately for diagnoses other than musculoskeletal complaints. The reduction in fear-avoidance beliefs was quite similar for the 2 diagnosis groups during follow-up, despite participants with psychological diagnoses having lower baseline values. The results also suggest that the work subscale is associated with future work participation for participants with psychological disorders. The association was, in fact, somewhat stronger for this diagnosis group than for the musculoskeletal group. Avoidance behaviour is seen in many psychological disorders. However, the FABQ could measure different characteristics for the 2 diagnosis groups. In psychological disorders, it might be measuring a more central part of the disorder itself, and not just a prognostic factor. This could also explain why the physical activity subscale showed a stronger association with future work participation for participants with a psychological diagnosis, compared with those with a musculoskeletal diagnosis.
The main strengths of this study were the randomized design and the use of registry data to assess sickness absence. The latter ensured no recall bias or missing data. Some limitations of this study should be addressed. Firstly, the response rate was low on follow-up questionnaires, gradually decreasing, from approximately 100% for the first questionnaire to 40–47% at 12 months’ follow-up. At the start and the end of the programme there were more missing questionnaires for the outpatient programmes, which we assume is due to organizational differences, as the inpatient participants answered the questionnaire at the centre, while the outpatient participants had to answer them at home. For the rest of the time-points, the response rate was similar between the programmes. To compare between-group changes over time, linear mixed models were used, which are less sensitive to missing values in outcome data. However, these models rely on the assumption of “missing at random”, and the possibility of bias due to differential loss to follow-up cannot be disregarded. The observed association between FABQ and future work had low precision, due to the low number of participants answering questionnaires at both the start and end of the programmes. However, other than the loss of statistical power, we do not expect missing questionnaires to affect these results significantly. We do not expect that those replying would differ from those not replying, in the association between the change on FABQ and work-participation days. Finally, in order to make the FABQ questionnaire usable for participants with conditions other than back pain, some of the wording was changed. Hence, the questionnaire was an adapted version of the previous validated version.
This study did not find any evidence to show that inpatient occupational rehabilitation reduced FABQ scores more than outpatient cognitive behavioural therapy. An association between changes in FABQ and future work participation was found. Participants with decreasing fear-avoidance beliefs had more work-participation days than those with consistently high or increasing fear-avoidance beliefs. Those with consistently low fear-avoidance beliefs had the most working days. The association was stronger for the work subscale than for the physical activity subscale. The results indicate that using a cut-off between low-risk and medium/high-risk patients could be useful in clinical practice to predict work participation. A novel finding is that baseline scores for the FABQ were associated with future work participation for participants with psychological diagnoses, indicating that this questionnaire might be useful to patient groups other than those with low-back pain, although further research is needed to substantiate this.
The authors thank project co-worker Guri Helmersen for valuable assistance, Tryggve Skylstad at the Norwegian Welfare and Labor Service for providing lists of sick-listed individuals, and Ola Thune at the Norwegian Welfare and Labor Service for providing sick leave data and insight to the National Social Security System Registry. We also thank clinicians and staff at Hysnes Rehabilitation Center and the Department of Physical Medicine and Rehabilitation at St Olavs Hospital, and the participants who took part in the study.
Funding. The Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology; The Research Council of Norway; and allocated government funding through the Central Norway Regional Health Authority.


 Click to show fullsize
Click to show fullsize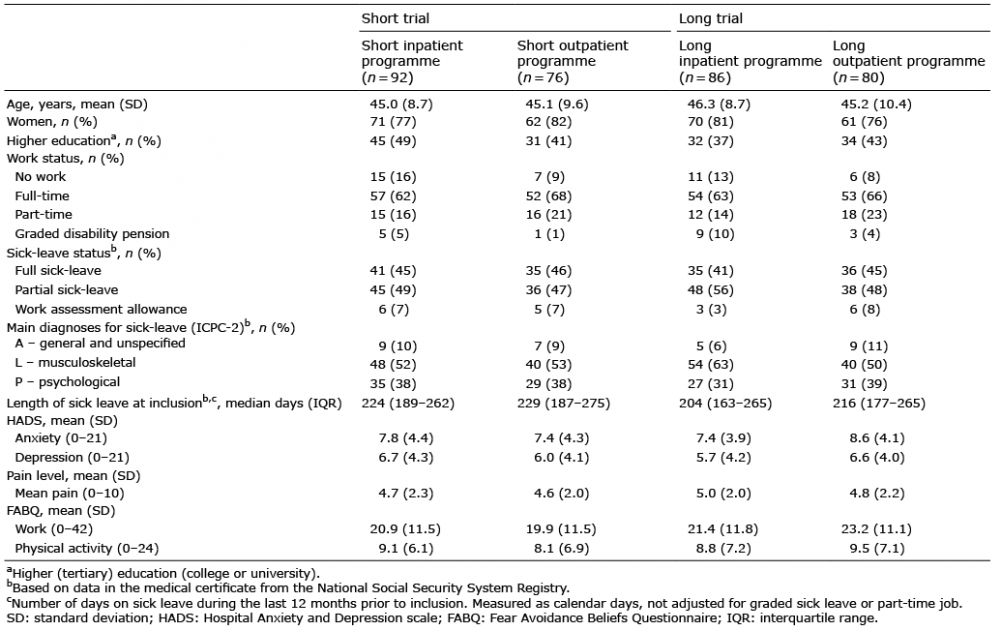 Click to show fullsize
Click to show fullsize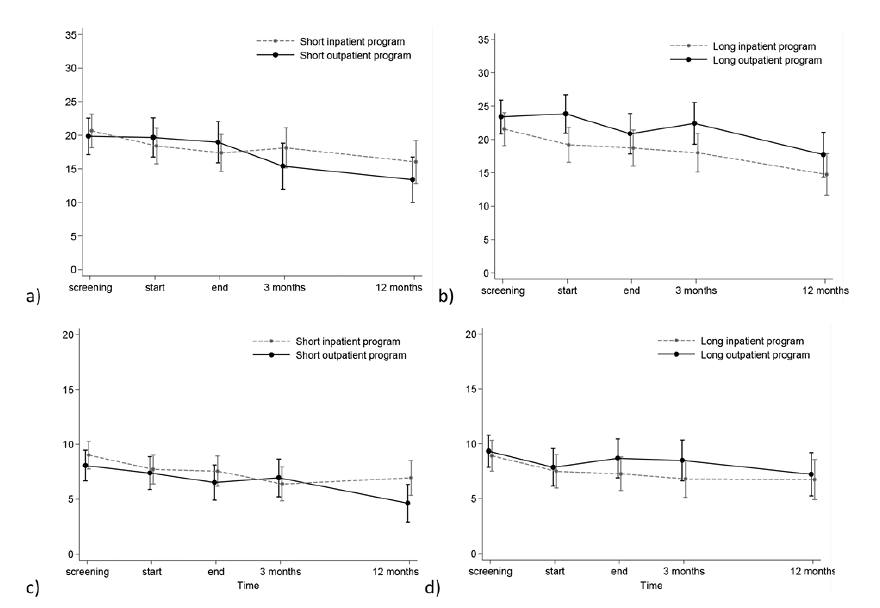 Click to show fullsize
Click to show fullsize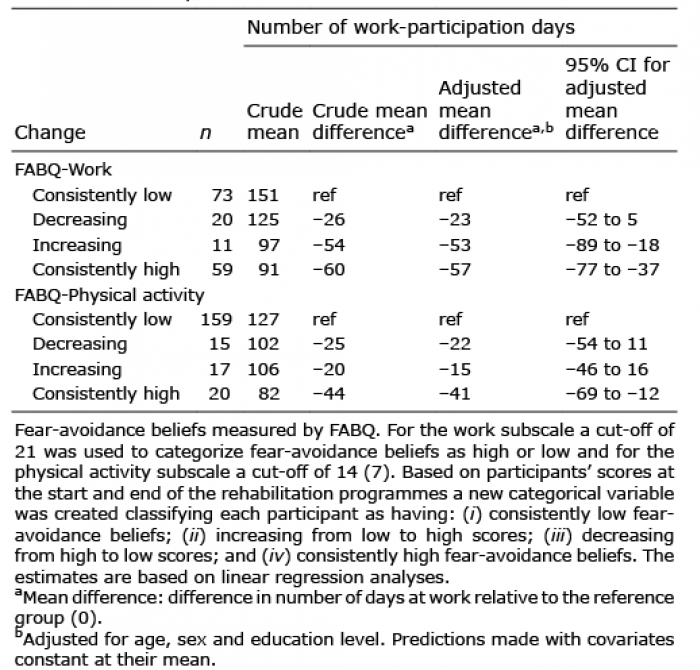 Click to show fullsize
Click to show fullsize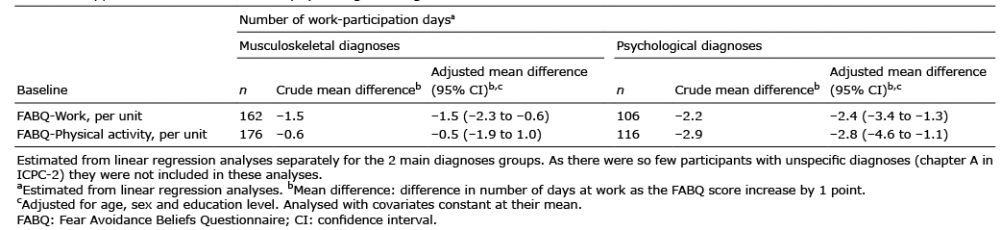 Click to show fullsize
Click to show fullsize