
From the 1Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Huddinge, 2Department of Neuroscience, Rehabilitation Medicine, Uppsala University, Uppsala, 3Theme Neuro, Karolinska University Hospital, Stockholm, 4Department of Neurobiology, Care Sciences and Society, Division of Physiotherapy, Karolinska Institutet, Huddinge and 5Function Area Occupational Therapy & Physiotherapy, Karolinska University Hospital, Huddinge, Sweden
Objective: To explore the importance of client characteristics (age, sex, stroke severity and participation before stroke), rehabilitation context (in-patient or client’s home) and approach (enhanced client-centeredness or not) on participation in every-day life after stroke.
Methods: A secondary analysis of data on 237 participants from a previous randomized controlled trial evaluating an enhanced client-centred intervention after stroke. Plausible associations between client characteristics, context and rehabilitation approach, and a positive outcome regarding participation were explored. Three different outcome measures for participation were used: Stroke Impact Scale 3.0, domain participation; Frenchay Activities Index; and Occupational Gaps Questionnaire.
Results: For all participants there was a significant association between mild stroke and a positive outcome using the Frenchay Activities Index. Among participants who had not received the enhanced client-centred approach, there was a significant association between mild stroke and a positive outcome using the Stroke Impact Scale. The context of rehabilitation, i.e. receiving home rehabilitation, was also associated with a positive outcome in the Frenchay Activities Index for the control group.
Conclusion: In order to increase participation in every-day life for people after stroke it appears to be important to use an enhanced client-centred approach, particularly when working within in-patient rehabilitation and with people with moderate or severe stroke.
Key words: stroke rehabilitation; activities of daily living; occupational therapy; brain injury; logistic regression; client-centredness.
Accepted Jan 22, 2019; Epub ahead of print Feb 27, 2019
J Rehabil Med 2019; 51: 160–166
Correspondence address: Martha Gustavsson, Alfred Nobels Allé 23, 141 83 Huddinge, Sweden. E-mail: martha.gustavsson@ki.se
This secondary analysis of a previous study evaluated the effects of enhanced client-centred intervention after stroke. The aim was to explore factors that could impact the client’s participation in everyday life after stroke. The factors explored were the characteristics of the client (their age, sex, stroke severity, and level of participation in everyday life before the stroke); the context in which the rehabilitation took place (at hospital or in the client’s home) and rehabilitation approach (receiving rehabilitation with an enhanced client-centred approach or not). In order to increase participation in everyday life for people after stroke it appears to be important to employ an enhanced client-centred rehabilitation approach, particularly when working within in-patient rehabilitation and with people with moderate or severe stroke.
A stroke may impact a person on many different levels, and returning to life as it was before stroke can be a long-term struggle (1). For many years after stroke, the physical, cognitive and emotional consequences can have a substantial impact on a person’s participation in everyday life at home and in society (2–5). The client-centred approach is highlighted in occupational therapy models (6, 7) and recommended for rehabilitation after stroke in order to achieve a successful rehabilitation outcome. To increase the clients’ involvement in the rehabilitation process it is important to collaborate with the client, and to focus on the needs and wishes of the client (8–10). Being able to participate in meaningful activities can promote health and life satisfaction for people with long-term conditions such as stroke, and is often expressed as the overall goal in rehabilitation (11, 12). However, participation is a complex concept that has been defined in various ways, such as being included and accepted in society, involvement in one’s life situation (13), and having the will, ability and opportunity to perform an activity (14). In this study, participation in everyday life was considered to include actual performance of activities, the meaning of and engagement in activities, and having control and freedom of choice (6, 7, 11).
An enhanced client-centred activities of daily living (ADL) intervention has previously been developed for rehabilitation after stroke and evaluated in a cluster randomized controlled trial (RCT) (15, 16). The enhanced client-centred intervention provided therapists with a structure for a client-centred approach when interacting with the client. The intervention included training the occupational therapists in having the client’s unique life-world experiences as the point of departure, and seeing the client as an active agent in goal setting, and in collaboration with the therapist in the rehabilitation process (15). The concept of ADL was widened to include both self-maintenance and domestic activities, as well as other ADL, such as leisure and social activities, that were meaningful for the client (11, 17).
The results from the RCT showed no difference in participation between participants who had received enhanced client-centred rehabilitation and those who had received usual rehabilitation (16). There was, however, a trend towards a clinically meaningful positive change in perceived participation in favour of the enhanced client-centred rehabilitation (16). Among all participants, both those receiving the enhanced client-centred rehabilitation and those receiving usual rehabilitation, some individuals reported a positive outcome in participation in everyday life at 12 months. In this present study secondary analyses were performed on data from the previous RCT in order to explore what characterized those individuals.
Thus, the aim of the current study was to explore the importance of client characteristics (age, sex, stroke severity, and participation before stroke), rehabilitation context (inpatient or client’s home) and approach (enhanced client-centeredness or not) on participation in everyday life after stroke.
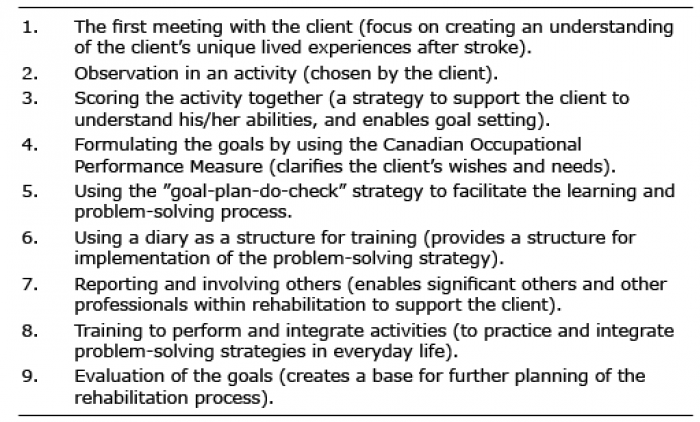
This study was a secondary analysis of participants from the RCT (15, 16) and included data on participants from both the intervention group and the control group. The enhanced client-centred ADL intervention was performed in 3 county councils in Sweden. Sixteen units within primary care and inpatient hospital-based rehabilitation units were randomized to the enhanced client-centred intervention or usual interventions, i.e. a control group (15). The intervention group received an enhanced client-centred intervention comprising 9 components (see Table I) and provided by trained occupational therapists. The control group received usual interventions that included a variety of strategies commonly used at each unit. The number of sessions and length of treatment period were not predetermined, but instead based on the needs of the clients (15). The number of sessions or contacts with an occupational therapist thus varied between 2 and 74 (mean 24) for the intervention group and between 1 and 167 (mean 18) for the control group during 1 year, between inclusion and the 12-month follow-up (16). Ethical approval has been obtained for this study from the Regional Ethical Review Board in Stockholm, Sweden. Registration Clinical Trials government identifier: NTCO 1417585.
Table I. The client-centred activities of daily living intervention
Included in the previous RCT (15, 16) were: people treated for acute stroke, less than 3 months after onset and referred to one of the 16 participating units; dependent in at least 2 ADL domains according to the Katz Extended Index of Independence in ADL (18); not diagnosed with dementia; and able to understand and follow instructions. Included in the present secondary analysis were participants from the RCT (15, 16) with complete data on at least 1 of 3 measurements on participation. Demographic data were collected at inclusion regarding the participants’ age, sex and co-habitation. The Barthel Index (19) was used to grade levels of stroke severity into mild = 50–100, moderate = 15–49, and severe ≤15 (18). Independence/dependence in ADL before stroke was assessed according to the Katz Extended Index of Independence in ADL (21) and the Frenchay Activities Index (FAI) was used as a pre-stroke measurement for participation in everyday social and domestic activities 3–6 months before the stroke (21).
Because a client-centred approach was adopted with the client’s perspective in focus, self-reported outcome measures were used to capture the complexity of participation in everyday life.
Stroke Impact Scale 3.0 (SIS), domain 8 “participation” was used at 3 and 12 months after inclusion to measure perceived impact of stroke on participation in ADL (22, 23). The score ranges from 0–100 and the higher the score the less impact of stroke. An improvement of ≥ 15 points or a maximum score of 100 at 12 months was defined as a clinically meaningful change (22) and considered to be a positive outcome.
Frenchay Activities Index (FAI) was used at inclusion as a pre-stroke measurement and at 12 months after inclusion to assess the frequency of participation in everyday social and domestic activities during the previous 3 or 6 months (21). The score ranges from 0 (inactive) to 45 (very active). A return to pre-stroke level of activity or a level of activity within age- and sex-related norms at 12 months were considered to be a positive outcome (24).
Occupational Gaps Questionnaire (OGQ) was used at 3 and 12 months after inclusion to measure the gap between activities a person performs (or not) and wishes to perform (or not) (25). A positive outcome was defined as: no gaps were reported, the number of gaps was reduced to a normal level according to age (26), or the number of gaps was reduced by 4 gaps (< 49 years of age); 2 gaps (50–64 years) or 1 gap (> 65 years of age).
In the analyses, the same covariates that were included in the previous RCT (15) were included as independent variables. The hypothesis was that client characteristics (age, sex, stroke severity and participation before stroke), rehabilitation context (inpatient or client’s home), and approach (enhanced client-centeredness or not) would differ between participants reporting a positive outcome and those reporting no positive outcome in participation in everyday life after stroke. Data from the intervention group and the control group were analysed separately. As a first step, univariable logistic regression analyses were performed to explore plausible associations in relation to the independent variables and a positive outcome regarding participation 12 months after inclusion. The independent variables were: age, sex, stroke severity according to the Barthel Index, rehabilitation context (inpatient medical-, inpatient geriatric-, or primary care home rehabilitation units) and participation in everyday life before stroke according to the FAI. Participants with moderate and severe stroke according to the Barthel Index were pooled and analysed as a single group due to a low number of participants with severe stroke.
In addition, multivariable logistic regression analyses were performed, in which both the intervention and the control group were included. Since the results from the univariate analyses indicated a greater difference in outcome between home and the medical rehabilitation (reference in the univariate analyses) than between geriatric and medical rehabilitation and due to few participants from the medical rehabilitation unit, participants treated at medical and geriatric rehabilitation units were pooled to a single inpatient rehabilitation group.
These analyses explored the relationship between context (inpatient or home rehabilitation) and approach (enhanced client-centred intervention or usual ADL intervention) of rehabilitation and having a positive outcome in any of the 3 outcome measures. The p-value was 0.05.
Included in this study were 237 participants from the previous RCT; 123 from the intervention group and 114 from the control group. Of the 237 participants, 7 were missing data for SIS; 7 were missing data for FAI; and 1 was missing data for OGQ. The characteristics of the participants are presented in Table II. Data on the 3 outcome measures of participation at inclusion (0 or 3 months) and 12 months after inclusion are presented in Table III. Positive outcomes in participation in everyday life were found for: 208 (90%) participants using SIS, 154 (67%) using FAI, and 162 (69%) using OGQ.
Table II. Participants’ characteristics
Table III. Outcome measures at baseline and 12 months after inclusion
The univariable analyses for the 3 outcome measures (SIS, FAI and OGQ) are presented in Tables IVa–IVc. Among participants in the control group, there was a significant association between mild stroke and a positive outcome using SIS domain 8 (OR 1.00 vs 0.25 for moderate/severe stroke) (see Table IVa). There was a significant association between mild stroke and a positive outcome using FAI for both the intervention group (OR 1.00 vs 0.36 for moderate/severe stroke) and the control group (OR 1.00 vs 0.12 for moderate/severe stroke) (see Table IVb). In addition, among participants in the control group there was a significant association between type of rehabilitation and a positive outcome using FAI (OR 3.20 for home rehabilitation vs 1.00 for medical rehabilitation) (see Table IVb). No significant associations were found with OGQ (see Table IVc).
Table IVa. Characteristics of persons categorized according to positive outcome or no positive outcome using Stroke Impact Scale 3.0, domain 8 (SIS), and univariable logistic regression for the association between the independent variables and a positive outcome in SIS, odds ratios (OR), 95% confidence intervals (95% CI) and p-values
Table IVb. Characteristics of persons categorized according to positive outcome or no positive outcome using Frenchay Activities Index (FAI) and univariable logistic regression for the association between the independent variables and a positive outcome in FAI, odds ratios (OR), 95% confidence intervals (95% CI) and p-values
Table IVc. Characteristics of participants categorized according to positive outcome or no positive outcome in Occupational Gaps Questionnaire (OGQ) and univariable logistic regression for the association between the independent variables and a positive outcome in OGQ, odds ratios (OR), 95% confidence intervals (95% CI) and p-values
Table V presents the results from the multivariable logistic regression analyses for both groups combined for the associations between the independent variables and positive outcome for the 3 outcome measures of participation. There were significant associations between having a mild stroke and a positive outcome using FAI (OR 1.00 vs 0.24 for moderate/severe stroke). Furthermore, a nearly significant association (p-value = 0.051) was found between home rehabilitation and a positive outcome using FAI for those in the control group (OR 1.00 vs 2.42 for in-patient rehabilitation) (see Table V). For the participants receiving the enhanced client-centred intervention, there were no significant associations between rehabilitation context and a positive outcome using the FAI, SIS or OGQ. Neither age, sex nor participation in everyday life before stroke were associated with a positive outcome in participation in everyday life after stroke.
Table V. Multivariable logistic regression for the association between the independent variables and a positive outcome using Stroke Impact Scale 3.0, domain 8 (SIS), Frenchay Activities Index (FAI) and Occupational Gaps Questionnaire (OGQ), odds ratios (OR), 95% confidence intervals (95% CI) and p-values
The aim of this study was to explore the importance of client characteristics (age, sex, stroke severity and participation before stroke), context (inpatient or client’s home), and approach (enhanced client-centeredness or not) of rehabilitation on participation in everyday life one year after stroke. The main findings were that, among participants receiving usual rehabilitation, stroke severity and rehabilitation context were associated with a positive outcome in participation, whereas only stroke severity was associated with a positive outcome for participants receiving an enhanced client-centred intervention.
Stroke severity, i.e. having had a mild stroke, was, in this study, associated with a positive outcome, using FAI for all participants, and SIS domain 8 for those in the control group. This result may reflect natural recovery in those with mild stroke, regardless of which rehabilitation they received. However, one explanation for the different results, depending on the instrument used, could be that the instruments assess different aspects of participation. The FAI measures the frequency of participation in daily activities, and the results of the current study show that a mild stroke is associated with an increased frequency of participation regardless of intervention received. The SIS, on the other hand, measures the perceived impact of stroke on participation in daily activities, and the results of this study imply that, although the actual frequency of participation did not change, using an enhanced client-centred approach may reduce the perceived impact of stroke on participation in everyday life. These results imply that stroke severity does impact the outcomes in participation in everyday life; however, stroke severity may be of less importance for outcome in perceived impact of stroke on participation when receiving an enhanced client-centred intervention. Thus, a client-centred approach may be particularly important for those with moderate to severe stroke. Results from previous studies on the association between stroke severity and participation are inconsistent. While some studies have shown that stroke severity, i.e. that a mild stroke could have a positive impact on participation both early on (at 1 month) (27) and a long time (at 6 years) after stroke (5), other studies have failed to confirm this association (2, 28).
In addition to stroke severity, context of rehabilitation, i.e. receiving home rehabilitation, was associated with a positive outcome in participation according to the FAI for the control group. One could argue that participants receiving home rehabilitation have usually had a less severe stroke and therefore are more likely to achieve a positive outcome in participation than those receiving in-patient rehabilitation. However, interestingly, the difference in outcome with regard to context of rehabilitation was found only in the control group. This result might reflect that the home environment itself induces a more client-centred approach, i.e. the needs are more easily identified by the client and supported by the therapist in the client’s real-life world, as has been suggested in previous studies (29, 30). Thus, it is plausible that, in the context of the home environment, the difference in client-centred behaviour between the occupational therapists who used an enhanced client-centred approach and those who delivered usual rehabilitation was too small or non-existent, whereas there was a difference in client-centeredness within the in-patient rehabilitation in the hospital between occupational therapists who used the client-centred approach and those who delivered usual rehabilitation.
This leads us to propose that, in contrast to the inpatient hospital environment, the home environment empowers the client and, as a consequence, facilitates the team members in adopting a more client-centred approach. Receiving rehabilitation in one’s home environment has previously been shown to contribute to individualization of the rehabilitation, and increased patient participation in goal-setting and participation in everyday life (31, 32). Furthermore, multi-professional teams providing rehabilitation in the clients’ homes described that the context enabled them to propose strategies to assist the clients to manage daily life (32). In addition, the home environment has been reported to make the clients aware of their limitations and to facilitate identification of difficulties in ADL that they wanted to address. It also allowed the clients to become partners in the rehabilitation process, in goal-setting and in planning their rehabilitation (33). Rehabilitation at home after stroke is recommended in the Swedish national guidelines for stroke care for those with mild to moderate stroke (1). Based on this study, providing an enhanced client-centred approach could be beneficial for those receiving rehabilitation at home, although it might be even more important for those receiving rehabilitation at an in-patient unit.
Since this study was a secondary analysis of a previous RCT, the result should be interpreted with caution. However, although the results from the RCT showed no differences in participation between participants who had received the enhanced client-centred rehabilitation and those who had received usual rehabilitation, the results from the secondary subgroup analyses of the present study complement our previous results.
When interpreting the results, the plausible difference in number of contacts with an occupational therapist should be taken into consideration, since the intervention group seemed to have had a higher mean number of contacts, whereas the total number of contacts seemed to be higher in the control group. However, these plausible differences have not been statistically confirmed.
Participation in everyday life is a complex concept that includes both the performance of, the meaning of, and engagement in activities (6, 7, 11). It is a challenge to find measures that capture the multifaceted concept of participation and that are sufficiently sensitive to detect change (34). One strength of this study was the inclusion of 3 different measures enabling capture of different aspects of participation. The measurements used; SIS (22), FAI (21) and OGQ (26) overlap in some areas and, combined, they cover the areas of instrumental ADL, leisure, social activities and work. The SIS 3.0 and FAI are 2 of the 5 most frequently used measurements in rehabilitation research on people after stroke (35). We also used OGQ to highlight participation in desired occupations, although it has been proven that the questionnaire is not sufficiently sensitive to be used to evaluate outcome of interventions, but is more suitable as a tool for goal-setting (36). Our results, showing that the 3 instruments identified different subgroups of participants as having a positive outcome, imply that in order to operationalize participation several measurements need to be used.
In order to increase participation, it is recommended that rehabilitation after stroke is carried out with a client-centred approach by multidisciplinary teams (1, 38). The client-centred ADL intervention has been used solely by occupational therapists, and it is not known to what extent other team members have used a client-centred approach.
Using an enhanced client-centred rehabilitation after stroke may reduce the perceived impact of stroke on participation in everyday life for those with moderate or severe stroke. In addition, it seems particularly important within in-patient rehabilitation to use an enhanced client-centred approach in order to increase participation in everyday life for people after stroke.
Financial support was provided by the Doctoral School in Health Care Sciences at Karolinska Institutet; The Swedish Research Council (VR); Swedish Research Council for Health, Working Life and Welfare (FORTE) and the Swedish Stroke Association.


 Click to show fullsize
Click to show fullsize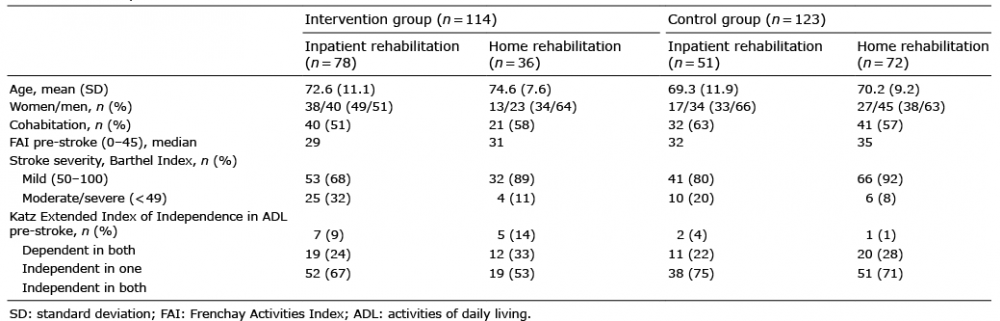 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize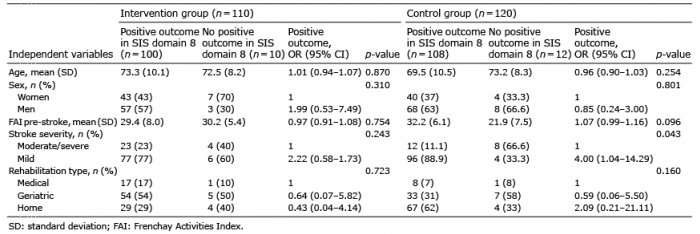 Click to show fullsize
Click to show fullsize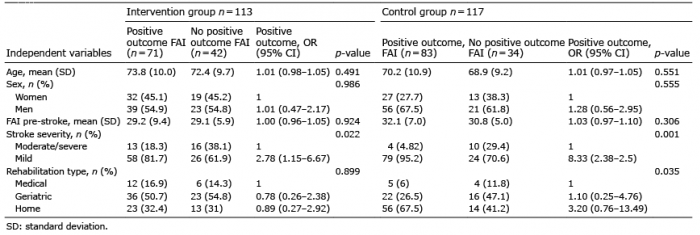 Click to show fullsize
Click to show fullsize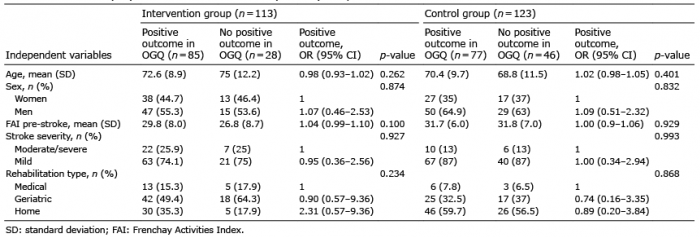 Click to show fullsize
Click to show fullsize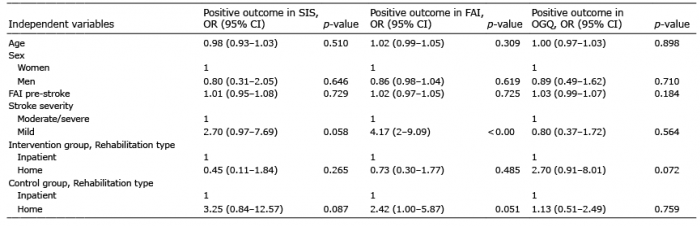 Click to show fullsize
Click to show fullsize