
From the 1Adelante Rehabilitation Centre, Department of Amputation, Traumatology and Orthopaedics, Hoensbroek, 2Maastricht University Medical Centre, Department of Trauma Surgery, Maastricht, 3Adelante, Centre of Expertise in Rehabilitation and Audiology, Hoensbroek, 4Nutrim School for Nutrition, Toxicology and Metabolism, Maastricht University, Maastricht and 5Maastricht University, Research School CAPHRI, Department of Rehabilitation Medicine, Maastricht, The Netherlands
*These authors contributed equally to this publication
Objective: To optimize rapid clinical recovery and restoration of function and functionality, permissive weight-bearing has been designed as a new aftercare mobilization regimen, within the upper boundary of the therapeutic bandwidth, yet safe enough to avoid overloading. The aim of the present paper is to describe a comprehensive protocol for permissive weight-bearing during allied health therapy and to report on the time to full weight-bearing, as well as the number of complications, in patients with surgically treated fractures of the pelvis and lower extremities undergoing permissive weight-bearing.
Patients and methods: This study included surgically treated trauma patients with (peri)- or intra-articular fractures of the pelvis and lower extremities. A standardized permissive weight-bearing protocol was used for all patients. Time to full weight-bearing and number of complications were recorded.
Results: This study included 150 patients, 69% male, with a median age of 48 years (interquartile range (IQR) 33.0, 57.0). The median time to full weight bearing was 12.0 weeks (IQR 6.8, 19.2). The complication rate during rehabilitation was 10%.
Conclusion: The permissive weight-bearing protocol, as described, might be beneficial and has potential to be implemented in trauma patients with surgically treated (peri)- or intra-articular fractures of the pelvis and lower extremities.
Key words: surgically treated fractures; rehabilitation; post-operative period; aftercare; guidelines; permissive weight-bearing.
Accepted Jan 30, 2019; Epub ahead of print Feb 15, 2019
J Rehabil Med 2019; 51: 290–297
Correspondence address: Pishtiwan Hassan Shaker Kalmet, Maastricht University Medical Center, Department of Traumatology, P. Debyelaan 25, 6229 HX Maastricht, The Netherlands. E-mail: pishtiwan.kalmet@mumc.nl
Aftercare in surgically treated trauma patients with fractures of the pelvis and lower extremities has remained largely unchanged during the past 60 years. To optimize rapid clinical recovery and the restoration of function and functionality, permissive weight-bearing has been designed as a new aftercare mobilization regime, within the upper boundary of the therapeutic bandwidth, yet safe enough to avoid overloading. The aim of the present paper is to describe a comprehensive protocol for permissive weight-bearing during allied health therapy and to report on both the time to full weight-bearing and the number of complications in patients with surgically treated fractures of the pelvis and lower extremities who undergo permissive weight-bearing.
A plethora of evidence is available about open reduction and internal fixation procedures in trauma patients with (peri)- or intra-articular fractures, as well as about the processes involved in bone healing (1, 2). However, the subsequent rehabilitation treatment, or early aftercare, has been less systematically documented and is often based on empirical, implicit knowledge of individual medical or allied health therapists, acquired throughout many years of clinical practice. No formal evidence-based guidelines are available on the aftercare of surgically treated fractures. In view of this lack of evidence, many orthopaedic and trauma surgeons tend to advise conservatively with regards to weight-bearing in rehabilitation, and hold on to the prevailing dogmas, i.e. recommending time-contingent progression of weight-bearing. In addition, even with specific advice from specialists, patients may not always be committed to complying with non-weight-bearing advice (3–5). It is remarkable that the recommendations for aftercare in patients surgically treated for fractures are still more or less the same as 60 years ago, without any sources of evidence being given for the advice (2, 6).
Fracture healing is a physiologically complex process (7). The pace at which bone formation processes take place, together with the aftercare treatment provided, determine what progression of weight-bearing may be applied. Weight-bearing dosage is often quantified in terms of percentage of body weight, or expressed in more general terms, such as non-weight-bearing/partial weight-bearing/full weight-bearing, without the therapist knowing which weight is actually borne at the level of the osteosynthesis and fracture during both rehabilitation training and daily activities. Despite this fairly ill-defined terminology, few complications due to overloading seem to occur in clinical practice. Nevertheless, both overloading and underloading may lead to a more complicated and extended recovery.
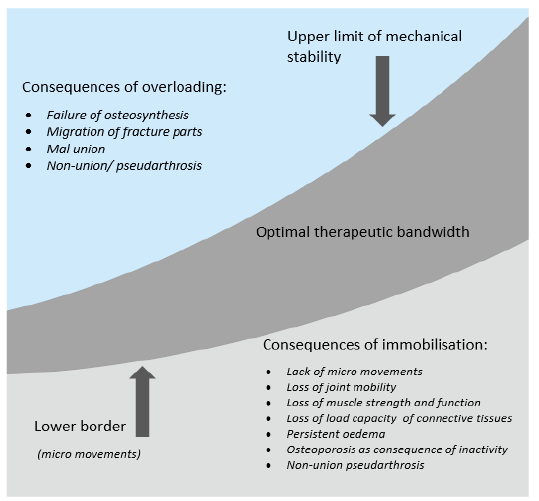
A schematic overview of the consequences of loading for the consolidation process is depicted in Fig. 1. Weight-bearing is necessary to elicit micro-movements between adjacent bony fracture components, stimulating biological processes that enhance fracture consolidation, and to minimize the negative effects of immobilization (8, 9).
Fig. 1. Schematic overview of the consequences of loading in the consolidation process.
To optimize rapid clinical recovery and the restoration of function and functionality, it may be useful to apply a treatment protocol that is near the upper boundary of the therapeutic bandwidth, yet safe enough to avoid overloading. However, no clear evidence on the location of this upper boundary is known from the literature. Therapy dosage in the early aftercare treatment of fractures is, to a large extent, determined by the load-bearing capacity of the bone, which, in turn, depends on the type of fracture, the bone quality, the soft-tissue quality, the stabilizing effects of the surrounding soft-tissue cuff, the stabilization method used (plaster/nail/plate) as well as the mechanical load-bearing capacity, and the point of application and direction of the forces relative to the line(s) of fracture (10, 11). However, functional outcome after fracture rehabilitation depends not only on mechanical stability, but also on an intricate complex of bio-psycho-social processes, involving physical tissue damage characteristics of the bone and other surrounding soft tissue, existing co-morbidities, and patients’ age, sex, physical and mental condition, as well as their cognitive abilities and coping styles (12–14). In International Classification of Functioning, Disability and Health (ICF) terms (15), this means that aftercare treatment should focus not only on the patients’ functioning, but also on their activity and participation levels. To date, the literature has reported no comprehensive, ICF-based protocol for the aftercare of patients with a surgically treated fracture that systematically addresses patient’s aftercare assessment, selection and provision of aftercare modalities, monitoring of therapy intensity, and evaluation of aftercare.
The aim of the present paper is to describe a comprehensive protocol for permissive weight-bearing (PWB) during allied health therapy and to report on both the time to full weight-bearing and the number of complications in patients with surgically treated fractures of the pelvis and lower extremities who undergo PWB.
Since PWB was implemented at our rehabilitation centre from 2003, and has been standard care since 2005, much experience has been gained in surgically treated trauma patients with (peri)- or intra-articular fractures of the pelvis and lower extremities. During this period, the research group has developed a PROtocol for permissive weight-bearing during allied health (paraMEdical in Dutch) THerapy and Evaluation of surgically treated fractUreS (acronym: PROMETHEUS) of the pelvis and lower extremities, which consists of 4 basic elements, viz. a patient assessment guide, an aftercare aims identification guide, a treatment guide, and a treatment evaluation guide. Fig. 2 shows a schematic representation of the use of the PROMETHEUS protocol. The fracture aftercare process starts by assessing the patient’s profile. Next, the generic and patient-specific treatment aims are identified, which, when combined, lead to the aftercare treatment aims. These aims are then compared with the patient’s profile descriptors, which, together with potential predictors of the outcome of the aftercare of the surgically treated fracture, may indicate: (i) the feasibility of the aftercare treatment aims, (ii) the estimated time frame in which the aims may be reached; and (iii) the intensity/dosage/weight-bearing needed to achieve the aims. Treatment progress and possible complications are assessed using the treatment evaluation guide, and may lead to alteration/adjustment of the treatment plan.
Fig. 2. Four basic elements of PROMETHEUS.
In addition to a description/classification of fracture(s), this guide consists of a set of patient profile descriptors that have been reported in the clinical literature as being potentially useful in predicting treatment progress and outcome of individual patients during fracture rehabilitation (12–14, 16). In effect, the guide serves to establish a patient profile, focusing on characteristics promoting or limiting fracture healing, therapy outcome and the occurrence or non-occurrence of complications during fracture healing. The PAG helps to draw clinical conclusions on: (i) the post-rehabilitation activity level to be expected, thus guiding the selection of attainable aims; (ii) therapy intensity; and (iii) the risk of complications occurring during the recovery process. Checking each PAG item results in a patient profile. The PAG is depicted in Fig. S11.
The AAIG helps to classify patient-defined treatment aims at the activity level (therapy milestones) aimed for during the recovery process. The classification embodies 5 areas of the ICF classification: mobility, self-care, domestic life, major life areas, and social and civic life. The early rehabilitation phase, which primarily aims at stance and ambulation, is subdivided into several sub-phases, of arbitrary length, i.e. with a certain bandwidth, during which weight-bearing on the fractured leg is gradually increased, with a simultaneous decrease in the use of mobilization-supporting aids, such as hydrotherapy, bars or crutches. The change from one sub-phase to the next is gradual and depends on the effectiveness with which the activity is performed by the patient, based on criteria defined in the protocol. Once a therapy milestone has been reached, it is marked and time-stamped in the AAIG, thus providing an overview of the progress of weight-bearing at the activity level and the progress of the patient’s functional activities. This also enables the
therapist to correlate information on the achievement of specific milestones to therapy effects recorded in the Treatment Evaluation Guide (TEG) (see below) and to the possible occurrence of complications. Table I presents an overview of the AAIG.
Table I. An overview of the aftercare aims identification guide
The TG (Fig. S2) aids in designing the treatment plan, i.e. selecting the means necessary to attain the treatment aims (at all 3 ICF levels) and the appropriate dosage of each of these means. In the early post-surgery rehabilitation phase, i.e. until the time when full weight may be borne by the patient, the patients’ treatment aims at the function/impairment and activity levels are, in general, similar for fractures of the pelvis and the acetabulum and other fractures of the lower extremities. At the function level, these rehabilitation aims are: control of oedema and hydrops, improvement of circulation, maintenance or improvement of mobility of the joint and the adjacent joints, as well as improvement of muscle function, endurance, and coordination. (See also Fig. S2 “select means”). Aims at the activity level are: performing all transfers necessary, maintaining stance, walking with and without aids, dressing and grooming. The purpose is to have the patient functioning independently (preferably without compensations) as soon as possible. The generic protocol designates the activities of “stance”, “walking”, and “transfers” as “milestones” (see also the AAIG in Fig. 2), because they have an inherent relationship to the load-bearing capacity of the fracture and can be translated into objectively quantifiable data representing the increase in the patient’s weight-bearing tolerance.
Ideally, the increase in load-bearing by the fracture takes place in parallel with fracture healing. In order to approximate this condition, the gradual increase in weight borne by the fracture is guided by the concurrent clinical symptoms. These symptoms are used to evaluate the progress during the rehabilitation treatment, based on the patient’s clinical manifestations and reactions to the therapy provided, as well as on the early signs or occurrence of possible complications that may necessitate adjustment of the therapy regime. The aim is to assess whether the therapy dosage is within the optimal therapeutic bandwidth throughout the aftercare process. The TEG screens for the possible effects of weight-bearing and for possible complications, using a number of clinical criteria and/or phenomena, i.e. pain (or changes in pain), temperature, erythema, oedema, hydrops, neurovascular signs, clinical control of bone alignment, instability, clinical weight-bearing capacity, control of adjacent soft tissue and control of mobility of adjacent joints, wounds, the patient’s therapy compliance, and changes in medication. Furthermore, if complications, such as infection, neurovascular issues, complex regional pain syndrome, failure of the osteosynthesis, and delayed union or non-union, occur, these have to be evaluated and graded by the rehabilitation physician or the surgeon in charge. Depending on the outcome of this evaluation, a decision is made to continue the current therapy regime, to adjust it, or to consult a medical specialist.
Permissive weight-bearing is operationalized in daily practice as follows: first, a patient profile is established by completing the PAG ( Fig. S11). This results in a comprehensive overview of patient and lesion characteristics that need to be taken into account when setting up a personalized rehabilitation treatment plan. Complications are gauged/inventoried in order to be able to adequately adjust the treatment plan when complications occur. Subsequently, the TG ( Fig. S21) assists the therapist in choosing the appropriate means and training intensities/dosages for setting up the aforementioned personalized training plan.
During the actual treatment phase, a gradual progression in functional activities guided by the subjective experience (pain and confidence to bear weight) and by objective clinical symptoms of the patient occurring during the process of rehabilitation. Symptoms such as the evolution of signs of inflammation, neuro-vascular status, weight-bearing tolerance, possible changes in alignment of the affected side of the body, quality and function of the soft tissue and involved joints.
The progression in functional activities is determined on the basis of the quality of the performance of a functional activity and is established in milestones to be achieved at activity level within the ICF areas: mobility, self-care, household, participation, and transport (Table I).
The therapy progress is determined not by the degree of loading the affected side of the body in kg or in percentage of bodyweight, because that, as discussed earlier, is an unrealistic representation of reality. When applying the permissive weight-bearing method, conscious choices are made to assess the maximum weight-bearing capacity of the fixed fracture and the damaged soft tissue. Within this process, we strive towards allowing the patient to apply the activities (formulated in the request for help (see Table I: aftercare aims identification guide)) with normal/optimal motor skills as quickly as possible. If necessary, these activities may be supported with walking aids and orthoses. The quality of the performance of the activity and safety (e.g. preventing stumbling) are leading in this approach. Progress is determined by the quality with which the activity is carried out and is recorded in the list with therapy milestones (see Table I) based on decreasing the use of walking aids. These walking aids contribute to the quality of the gait pattern and to safety, and may possibly compensate for a certain limitation in the patient’s conditional capacities, such as reduced muscle strength, stability or postural balance reactions. The milestone is reached only if the gait pattern is executed optimally, i.e. resembling normal gait as closely as possible, and can be performed independently and safely by the patient. In case of delayed recovery or permanent impairment (due to, for example, complications during rehabilitation), a choice must be made for the best possible gait pattern, optimal for each individual patient. It should include the following aspects:
In case of limited conditional abilities, such as lack of joint mobility, muscle strength, joint stability, endurance and/or postural balance, trade-offs have to be made regarding the above items. The patient will have to give a priority as to which of the above aspects are most important to them.
In order to assess the level of weight-bearing and the rate of complications when using the PROMETHEUS protocol, a pilot study was conducted in 2015, which included surgically treated trauma patients with (peri)- or intra-articular fractures of the pelvis and lower extremities who were admitted to our rehabilitation centre between 2005 and 2015.
Patients with pathological fractures, shaft fractures treated with intra-medullary nailing, or fractures treated with external fixation, and patients with amputations in the area of the lower extremity, were excluded. Also excluded were patients with cognitive dysfunction, due to the consequences of a severe neurotrauma or to concomitant or drug-based mental illness.
All data in the study were collected retrospectively from the electronic patient records, by 1 researcher. Demographics of patients retrieved included age, sex, date of accident, type of fracture and type of fixation.
Primary outcome measures included the time from surgery till full weight-bearing and the total number and type of complications at 1-year follow-up. Type of complications were defined separately, comprising adverse events that occurred during 1 year of the PWB regime. The rate of individual complications was also recorded.
The medical ethics committee approved this study, and informed consent was given by all patients.
Statistical analysis was performed with IBM SPSS Statistics, Version 23.0, Armonk, New York. Descriptive statistics were used to describe the demographic data and baseline characteristics of the entire population. Results are presented as frequencies and percentages. Data are described as median values, interquartile ranges [x,y] and the minimum and the maximum [min–max]. Binary logistic regression was performed to assess independent predictors of late full weight-bearing (> 12 weeks) throughout both PWB and RWB groups. The level of statistical significance was set at α = 0.05.
This pilot study included 150 patients, of whom 69% were male, with a median age of 48 years ([IQR 33.0, 57.0], [15–77] years). The sample included different types of surgically treated (peri)- or intra-articular fractures of the pelvis and lower extremities from the pelvis to the foot. Baseline characteristics are shown in Table II. In all, n = 124 (82.7%) of the patients had 2 or more fractures, and n = 19 patients (12.7%) had head injuries. In total, 201 lower extremity fractures were identified, which can be divided into 5 subtypes: pelvic/acetabular (n = 76), distal femoral metaphysis or (peri-)articular distal femur (n = 42), tibial plateau (n = 31), distal tibia/ankle (n = 31), and foot (talus, calcaneus) (n = 21).
Table II. Baseline characteristics of total sample
The median time from fracture surgery to the start of PWB was 2.0 weeks ([IQR 2.0, 3.25], [0–9] weeks). Fifty-two percent of the patients (n = 78) reached full weight-bearing within 12 weeks. The median time to full weight-bearing was 12.0 weeks ([IQR 6.82, 19.18], [2–52] weeks). Table III specifies for each group of fractures the median and percentage of patients reaching full weight-bearing.
Table III. Time to full weight-bearing for specific fracture types (n = 150)
The complication rate during postoperative rehabilitation was 10.0% (n = 15) of all patients included. Most complications involved non-unions (n = 5), wound infections (n = 4) or early removal of implants (n = 3) because of pain and/or infection. There was one implant failure and no secondary dislocations. The numbers and types of complications are shown in Table IV, specified for each fracture category.
Table IV. Number of fractures and types of complications
This pilot study found that 52% of the patients with surgically stabilized (peri)- or intra-articular fractures using a PWB regime according to our in-house PROMETHEUS protocol were able to walk with full weight-bearing within 12 weeks, indicating a mean shortening of 4 weeks compared with the current AO guidelines (2). The total complication rate with permissive weight-bearing was 10.0%. The fact that approximately half of the patients in our study did not reach full weight-bearing within 12 weeks might be due to hospitalization delay and the high comorbidity rate in our sample.
From a clinical point of view, the PROMETHEUS framework has been designed to be able to systematically, transparently, and falsifiably plan, implement and evaluate/measure patient-tailored allied health aftercare for surgically treated patients with fractures of the pelvis and the lower extremities, starting from the post-surgery phase and extending to the full weight-bearing phase and into activities of daily living. The protocol also facilitates the systematic collection of clinically relevant data (clinimetrics) that may guide the gradual (rather than stepwise) progression of the dosage of weight-bearing and therapy (based on the patient’s current clinical manifestations), as well as assessing complications or their prevention, and facilitating the setting of realistic rehabilitation aims. Initially, the patient’s characteristics, potential predictors of fracture consolidation and risks of complications are identified. During the protocolized treatment process, clinical symptoms are screened at the beginning of each therapy session, using the checklist to establish to what level weight-bearing and therapy intensity may proceed. It also identifies early warning signs as to possible complications, such as failures of the osteosynthesis material, bone alignment problems, non-unions, or infections. Data regarding treatment aims, means used, dosage, milestones achieved at the ICF activity level, etc. are recorded systematically.
The more scientifically relevant reason for developing a systematic and comprehensive protocol was the fact that, despite major improvements in surgical treatment and osteosynthesis materials, rehabilitation aftercare after surgical treatment of fractures has remained almost unchanged over the last 6 decades.
The PROMETHEUS protocol has been developed in close cooperation between rehabilitation specialists, allied health staff and trauma surgeons. It should serve as a general reference framework and starting point for a discussion of the systematic optimization of allied health aftercare in patients with surgically treated fractures, rather than as a library of predefined standard solutions (17).
It is widely assumed by surgeons that the fixation of pelvic and lower extremity fractures should not be absolutely rigid when physiological forces act on the bones during early weight-bearing (18). One of the key objections to allowing early weight-bearing is the possibility of fracture displacement (19). On the other hand, various authors, including those of more recent randomized controlled trials, have stated that weight-bearing does not pose an undue risk of complications or produce poorer outcomes than non-weight-bearing protocols (20). These 2 statements are contradictory and require further evaluation.
To our knowledge there have been no studies on early PWB and its complications during rehabilitation from (peri)- or intra-articular fractures of the pelvis and lower extremities treated with internal fixation. Recent literature has reported composite postoperative complication rates of up to 37% (range 0.7–37%) (21–30). A comparison of our complication data with published data based on applying the current guidelines shows comparable rates of complication for all our groups treated with the PWB protocol (21–30).
To our knowledge, no study has found any difference in fracture displacement or healing between early and late weight-bearing regimes using radio-isometric analysis. One study of ankle fractures did find a small (0.4 mm) widening of the talar mortise, but this had no clinical or functional significance (31). The participants in the study had stable, anatomically adequate fixation of the distal fibula and/or medial malleolus prior to being included in the trials. Recent studies on early weight-bearing of surgically treated fractures of the ankle joint showed good outcome and even a lower rate of plate removal (31, 32). In one radiostereometric study with fractures of the tibial plateau, the mean cranio-caudal migration of the fracture fragments at 1 year after the start of early weight-bearing was insignificant –0.34 mm (–1.64 to 1.51) (33). This case series showed that, in the Schatzker type II fractures that were investigated, internal fixation with subchondral screws and a buttress plate provided enough stability to allow post-operative permissive weight-bearing, without harmful consequences (33). While a certain minimum level of loading is required to elicit micro-movements between adjacent bony fracture components, stimulating the biological processes that enhance fracture consolidation and minimizing the effects of immobilization (4, 8), both over- and under-loading may lead to prolonged and complicated recovery.
While instructions for rehabilitation given to patients may be clear, patient compliance with a non-weight-bearing or limited weight-bearing regime has been found to be poor (34, 35). A number of studies found that patients had actually exceeded the prescribed amount of partial weight-bearing even though their self-reported compliance was high (35, 36). For example, Braun et al. used for their study a continuously measuring pedobarography insole to measure weight-bearing in trauma patients with fractures of the lower extremities. The study showed that, despite physical therapy training, weight-bearing compliance to recommended limits was low (36). Overall, despite their willingness to comply, patients often do not adhere to the suggested restrictions on weight-bearing and increase their weight-bearing as fracture healing progresses.
To optimize recovery with a minimal complication rate, we recommend a treatment that is near the upper boundary of the therapeutic bandwidth, yet safe enough to avoid overloading, and this treatment is a key component of our PROMETHEUS protocol.
The lack of evidence on aftercare protocols and on permissive weight-bearing was the reason for designing the PROMETHEUS protocol. In this study a description of a comprehensive protocol for permissive weight-bearing has been presented, together with data on both time to full weight-bearing and the number of complications in patients with surgically treated fractures of the pelvis and lower extremities. This pilot study is quintessential for estimating the sample size in future prospective trials and for gaining insight into the heterogeneity that exists within and between different kind of fractures of the lower extremity with regard to time to full weight-bearing and number of complications. However, limitations of the current study include the retrospective nature of the study and, due to this retrospection, not taking into account surgeon-oriented functional outcome scores (e.g. knee function) or generic patient satisfaction scores. Furthermore, no radiological controls have been performed to investigate the alignment of the fractures and the fracture healing. Another limitation of the study is the lack of monitoring patient compliance.
To mitigate the aforementioned limitations, and to determine whether a PWB protocol results in more favourable process outcomes and patient outcomes, requires further research to establish the added value in terms of effectiveness and cost-effectiveness. To that aim, we have started a prospective cohort study with a control group, also including patient-reported outcome measures to cover the appropriate ICF levels (37).
The PROMETHEUS protocol is a patient-tailored permissive weight-bearing protocol. Given the low complication rate, the protocol might be beneficial to implement in the treatment of trauma patients with surgically treated articular or (peri)- or intra-articular fractures of the pelvis and lower extremities.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize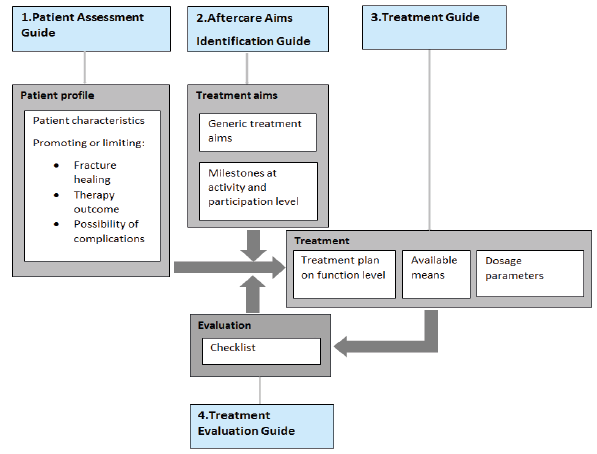 Click to show fullsize
Click to show fullsize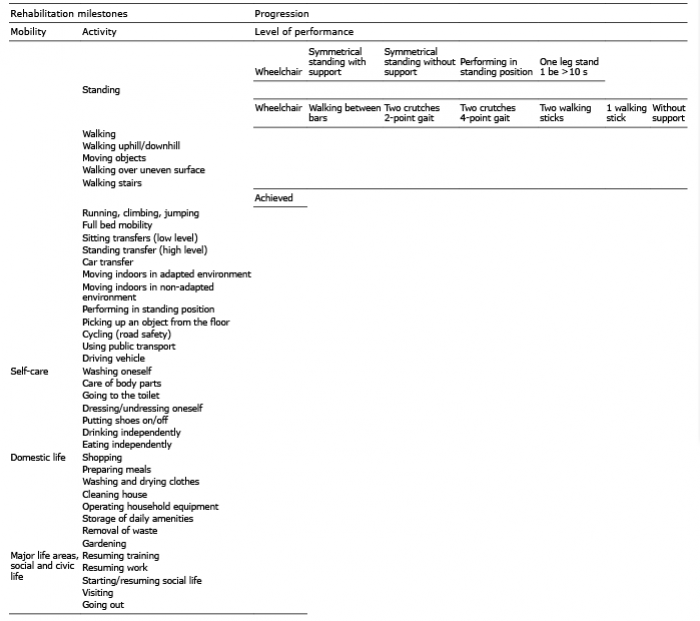 Click to show fullsize
Click to show fullsize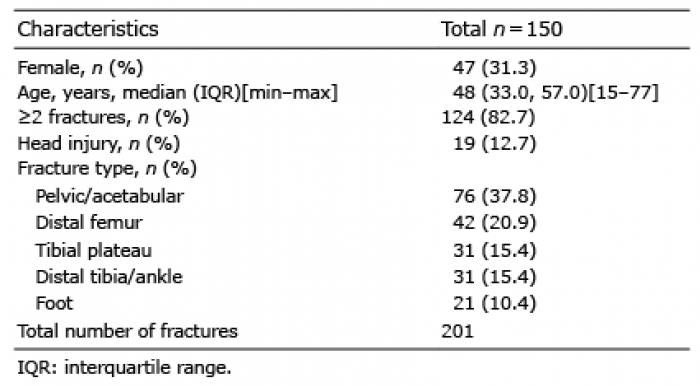 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize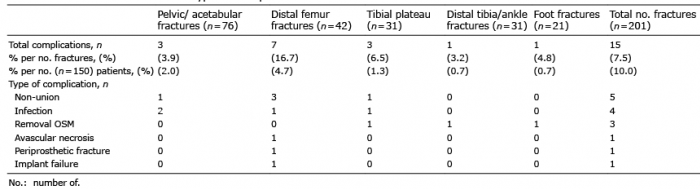 Click to show fullsize
Click to show fullsize