
From the 1University of Helsinki, Faculty of Medicine, 2The Finnish Association of People with Physical Disabilities, Helsinki, 3The National Institute for Health and Welfare, Welfare Department, Ageing, Disability and Functioning Unit, 4Central Finland Central Hospital, Rehabilitation Department, Jyväskylä, 5Center for Life Course Epidemiology Research, University of Oulu, Oulu, 6Tampere University Hospital, Department of Neurosciences and Rehabilitation, Tampere, 7Helsinki University Hospital, Department of Internal Medicine and Rehabilitation/Spinal Cord Injury Outpatient Clinic, Helsinki, 8Oulu University Hospital, Department of Medical Rehabilitation/Spinal Cord Injury Outpatient Clinic, Oulu, 9The Finnish Association of Spinal Cord Injured Akson, Helsinki, 10Seinäjoki Central Hospital, Department of Rehabilitation, Seinäjoki and 11Validia Rehabilitation, Helsinki, Finland
Background and purpose: The purpose of the Finnish Spinal Cord Injury Study (FinSCI) is to identify factors related to the health and functioning of people with spinal cord injury, their challenges with accessibility, and how such factors are interconnected. The International Classification of Functioning, Disability and Health (ICF) is used as a structured frame-work in the study.
Design: Protocol of mixed methods study.
Results: Study participants were recruited from all 3 spinal cord injury outpatient clinics in Finland. The final target group consists of 1,789 subjects with spinal cord injury. The final questionnaire was formed from 5 different patient-reported instruments. The spinal cord injury-specified instruments are the Spinal Cord Injury Secondary Condition Scale, the Spinal Cord Independence Measure, and the Nottwil Environmental Factors Inventory Short Form. In addition, questions from the following generic instruments were chosen after a selection process: the Patient-Reported Outcomes Measurement Information System, PROMIS®, and the National Study of Health, Well-being and Service, FinSote. Altogether, the final questionnaire covers 64 ICF categories and consists of 151 ICF-linked questions.
Conclusion: The formulated questionnaire covers widely different aspects of health, functioning and accessibility. The questionnaire results and subsequent interviews will help in developing care and rehabilitation policies and services for people with spinal cord injury.
Key words: spinal cord injury; International Classification of Functioning Disability and Health; data collection; questionnaire design; community survey; methodology.
Accepted Feb 6, 2019; Epub ahead of print Feb 25, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Susanna Tallqvist, Faculty of Medicine, University of Helsinki, FI-00014 Helsinki, Finland. E-mail: susannatallqvist@gmail.com
The Finnish Spinal Cord Injury Study (FinSCI) collects information from people with spinal cord injury about their own health, ability to function, and their challenges in terms of accessibility. The study includes a questionnaire and interviews. The questionnaire is based on international guidelines. Participants are recruited from the registers of Oulu, Tampere and Helsinki university hospitals. Almost 1,800 people met the criteria and it is hoped that at least half of them will answer the questionnaire. Interviews will be performed with 45 persons. Interviews have several different themes, such as returning home, housing and living arrangements, employment situation and pathways to employment. The aim of this study is to help to develop the care and rehabilitation policies for the spinal cord injury population, to plan training models, and to provide information for different parties and gain understanding of the lived experience of people with spinal cord injury.
Spinal cord injury (SCI) can be traumatic (TSCI), resulting from an accident or injury, or non-traumatic (NTSCI), resulting from a congenital disorder, disease or degenerative condition (1). The level and completeness of injury determine the remaining sensory and motor functions (2). Damage to the autonomic nervous system leads to dysfunction in several other organs, such as the urinary bladder, bowel and sexual organs (3), as well as in the respiratory tract, blood vessels and sweat glands (4). Due to the multifaceted nature of their injury, people with SCI are significant consumers of rehabilitation and healthcare services (5). Despite experiencing limitations in functioning, people with SCI pursue ordinary lives that encompass a home, family, functioning in various domains, employment and their own well-being and quality of life (6).
Health and functioning play a major role in enabling people with SCI to participate in daily activities, social events and society in general (6). In the International Classification of Functioning, Disability and Health (ICF) limitations in human functioning are viewed as a mismatch between an individual’s health and the concrete requirements of his or her life situation (7). ICF includes over 1,600 categories with Core Sets to help focus on the most important factors of certain health statuses, such as SCI (8). In the latest studies of SCI, the International Spinal Cord Injury Community Survey (InSCI) and the Swiss Spinal Cord Injury Cohort Study (SwiSCI), the categories from the ICF long-term Brief Core Set and the rehabilitation Core Set have been seen as a the most suitable approach to identify what to measure (9, 10). In Finland, however, current documentation is focused on biomedical issues, e.g. body structures and functions, while data collection on comprehensive functional ability is still lacking.
According to the new Health Care Act and government decree in 2011, acute care, immediate rehabilitation and life-long multi-professional follow-up, care and rehabilitation of SCI have been centralized at 3 university hospitals in Finland: Oulu (OYS), Tampere (Tays) and Helsinki (HUS) University Hospitals (11). These hospitals serve the whole SCI population, both previously and newly injured patients, in their hospital district areas. The main goal of these clinics is to provide specialized care for SCI-related health problems and to counsel and plan rehabilitation according to recently published rehabilitation practice guidelines (12). In Finland, as in the rest of the world, the population is ageing, which is setting new demands for the system (13). A recent Finnish study in the OYS and Tays districts shows that the number of SCI incidents is increasing (14). This is due to the ageing population, since degenerative changes in the spine increase the risk of SCI (15). Elderly people are more vulnerable both to traumatic and non-traumatic injuries (16). Thus, the purpose of the Finnish Spinal Cord Injury Study, FinSCI, is to identify factors related to the health and functioning of people with SCI, their challenges with accessibility and how such factors are interconnected in Finland.
FinSCI comprises a quantitative component (the questionnaire) and a qualitative component (the interviews). Thus, it aims to reinforce and complement the data produced by establishing a dialogue among various types of data.
The study subjects were recruited by exploring the patient registers in OYS, Tays and HUS. A more systematic data collection of the SCI population started in different outpatient clinics at different times (OYS, January 2012; Tays, May 2011; and HUS, August 2013). The selection of patients for the study was performed at the start of the systematic data collection, and lasted until the end of 2017 at OYS and Tays and until the end of June 2018 at HUS.
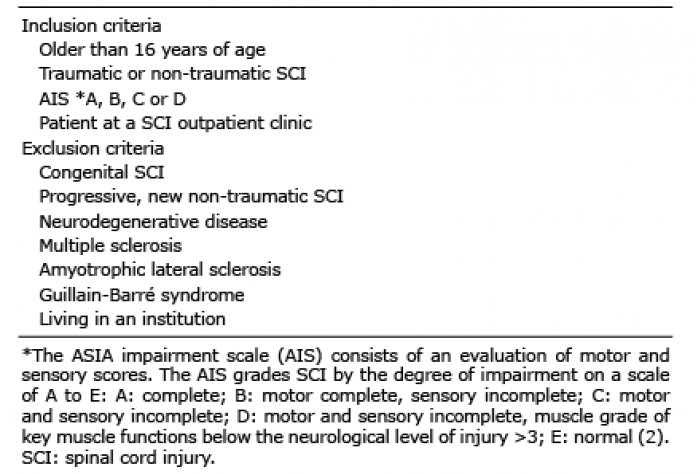
The inclusion and exclusion criteria for research participants are presented in Table I. Patient registers were explored to collect participant social security numbers and sex. The ASIA impairment scale (AIS) and the neurological level of injury were assessed based on the International Standards for the Neurological Classification of Spinal Cord Injury (ISNSCI) (2). The aetiology and date of the SCI (TSCI or NTSCI) were also collected from patient registers. For some patients who were injured before the legislative amendments were enacted, the information was requested from Validia Rehabilitation in Helsinki (previously the Käpylä Rehabilitation Centre), where the patients with most severe SCI in Finland were rehabilitated prior to the legal changes. The study was approved by the HUS Coordinating Ethics Committee (HUS/1776/2017).
Table I. Inclusion and exclusion criteria
CF as a background for the questionnaire. FinSCI utilizes 5 different ICF Core Sets: (i) rehabilitation Core Set (n = 30 categories), (ii) long-term comprehensive core sets for SCI (n = 168), (iii) long-term brief core sets for SCI (n = 33), (iv) post-acute comprehensive Core Set for SCI (n = 162), and (v) post-acute brief core set for SCI (n = 25) (7). The ICF categories included in both Brief Core Sets or in 3 different Core Sets including rehabilitation were chosen to be the most important categories and form the FinSCI data-set. The data-set includes 43 categories to which items from the preselected instruments are linked.
Outcome instruments of the questionnaire. As part of the questionnaire, sociodemographic data, such as the living and working situation and other patient characteristics, were collected. The level (tetraplegia/paraplegia) and completeness (complete/incomplete) of the SCI will also be asked from the participants themselves.
To cover the 43 chosen ICF categories from the different areas of health, functioning and environmental factors, 3 self-reported SCI-specific and 2 generic instruments were preselected (Table II). The selection of SCI-specific measures was based on InSCI, which recommends the use of these measurements (17), which were used as a whole. Generic instruments were chosen to be part of the questionnaire, since they are comparable across the subject groups and recommended by the National Institute for Health and Welfare. All instruments have been translated into Finnish using official translation processes (18), and they are presented in the chapters following Table II. The final questions from the generic instruments were based on a selection process (see the Selection process of generic instruments).
Table II. Outcome instruments used for the questionnaire in the Finnish Spinal Cord Injury Study
Spinal Cord Injury Secondary Condition Scale (SCI-SCS). The SCI-SCS is a self-reported health instrument scale used by SCI patients. Respondents are asked to rate their health over the last 3 months. The questionnaire comprises 16 items in which health conditions are evaluated on a scale of 0 to 3 (0 = not experienced in the last 3 months or is an insignificant problem, 1=mild or infrequent problem, 2 = moderate or occasional problem, 3 = significant or chronic problem). The maximum score on the scale is 48. The higher the score, the more health problems the respondent experiences. SCI-SCS has a proven reliability and validity (19, 24) and is included in the Spinal Cord Injury Research Evidence (SCIRE) database as a recommended health measure to be used for people with SCI (25).
Spinal Cord Independence Measure – Self Report (SCIM-SR). The SCIM-SR is a self-report questionnaire developed on the basis of the SCIM (Spinal Cord Independence Measure) and was designed to assess functioning in people with SCI. The SCIM is recommended by The International Spinal Cord Society (26) and by experts of functional ability from the National Institute for Health and Welfare in Finland (27). The SCIM-SR shows an excellent correlation with the SCIM. The self-reported version is preferred because it enables active self- assessment by patients with SCI. SCIM-SR is a valid and reliable measure (20). SCIM-SR comprises 17 items collected from 3 sub-scales: self-care, respiration, and sphincter management and mobility. For each item, the person evaluates the extent of assistance or assistive devices needed to complete activities and items on a scale from 0 to 15 points. The maximum score is 100, and the minimum is 0. The higher the score, the better the respondent’s independent functioning (20).
Nottwil Environmental Factors Inventory Short Form (NEFI-S). NEFI-S is a self-reported measure for assessing the impact of environmental factors. The measure is based on the ICF classification and comprises 14 questions. In the NEFI-S measure, respondents rate statements regarding accessibility and attitudes based on their experiences in the previous 4 weeks. The response alternatives are 0 = ”no influence”, 1 = ”made my life a bit harder”, and 2 = ”made my life a lot harder”. The maximum score is 28. The higher the score, the more difficult the respondent perceives his or her life to be and the more barriers he or she has experienced over the preceding 4 weeks (21). As NEFI-S is quite a new measure, minimal feedback exists on its suitability and usage. NEFI-S has proven to be valid in 2 studies (28, 29).
Patient Reported Outcomes Measurement Information System (PROMIS®). PROMIS® is a dynamic and extensive set of self-report measures to evaluate various aspects of functioning or quality of life. It comprises item banks relating to the physical, social and psychological dimensions of functioning and a generic global health short form. Single questions are also valid to use alone. The measures have undergone extensive qualitative and quantitative evaluations during the development phase from 2004 to 2014 (22). Following this, validation efforts have continued in several studies of general and clinical populations, including people with SCI (30, 31). The response options are mainly 5- or 6-level Likert scales measuring time or quantity (22).
The National Study of Health, Well-being and Service (FinSote). The FinSote survey form includes 92 questions addressing several areas. The study enables the monitoring of changes in the well-being and health of different population groups and regions, and it produces follow-up and evaluation data. The FinSote survey produces important information required for the management of the changes in health and social service (23). The answers are given mainly in 4- or 5-level Likert scales, measuring time, opinion or quantity.
Selection process of generic instruments
First, the research group selected the preliminary PROMIS® and FinSote measures according to how they were linked to the ICF. The PROMIS® questions consisted of Physical Function (120 questions) and Emotional Support (16 questions) item banks, Satisfaction with Sex Life domain (5 questions) and 10 short forms (SF) of the item banks; Fatigue SF8a, Sleep Disturbance SF8a, Depression SF8b, Pain Interference SF6b, Pain Intensity SF3a, Satisfaction with Social Roles and Activities SF8, Self-Efficacy for Managing Symptoms 8a, Ability to Participate in Social Roles and Activities SF8a, Satisfaction with Participation in Discretionary Social Activities SF7a and Psychosocial Illness Impact Positive (customized SF of 8 questions). The number after each short form indicates the number of questions in each instrument. The 8 FinSote questions consisted of social affairs and health. In addition, the research group formulated 7 questions. Finally, the PROMIS Global Health (10 questions) was taken as a whole without evaluation.
Thereafter, the generic instruments were evaluated by 7 subjects with SCI. The aim was to select the most relevant items for the SCI population as well as to maintain a reasonable level of burden for the patients, a consequence of completing multiple questions. Participants were asked to evaluate the relevance of the preselected PROMIS® and FinSote items, as well as the questions made by the FinSCI research group. A Webropol survey tool was used for this evaluation. Participants announced their willingness to evaluate questions voluntarily and rated questions privately to avoid changes in opinions during evaluation.
Altogether, 220 questions were evaluated. Participants scored each question on a scale of 1–4 (1 = not relevant, 2 = somewhat relevant, 3 = very relevant, 4 = highly relevant). This content validity indexing (CVI) technique produces an item-level content validity index (I-CVI) and scale content validity (S-CVI). In the present study, the I-CVI was used as a selection method. The recommendation for good content validity is to have at least 3 evaluators. In the case of 7 evaluators, like in the FinSCI study, I-CVI 0.71 is interpreted as good and 0.86 or higher as excellent (32). Only questions with I-CVI 0.71 or higher were chosen for the final questionnaire.
The Finnish Association of People with Physical Disabilities and the Finnish Association of Spinal Cord Injured Akson will encourage survey recipients to respond to the questionnaire by providing information on the study. The questionnaire will be sent 2 times 2–3 weeks apart to get the highest possible response rate.
A total of 45 volunteer survey respondents, 15 from each university hospital district (OYS, Tays, HUS), will be asked to participate in thematic interviews. To get a wide variety of Subjects with SCI who will mirror the distribution of the SCI population in Finland, the selection will be based on age, sex, lesion level, municipality of residence and time since the onset of SCI. This information is based on collected data from the FinSCI study. One or 2 researchers will conduct the semi-structured interviews, which will be formed on the basis of the research questions. The following topics will be discussed:
Statistical analyses will be used to draw inferences on health and functioning in people with SCI. Quantitative data analysis will be based on descriptive methods, e.g. on frequencies (categorical variables) and means (continuous variables). In addition, cross-tabulation and the χ2 test will be used to test group differences and interactions between health and functioning. Functioning profiles across all functioning limitations will be created. Factor analysis will be applied to investigate the dimensionality of certain variables. Graphs will be used to visualize the extent of functioning limitations in hospital district samples (OYS, Tays and HUS) and in SCI subgroups. Comparisons will be made using the SCI grade by AIS (A, B, C and D), level of injury (tetraplegia/paraplegia), completeness of injury (complete/incomplete), aetiology (TSCI/NTSCI), time since injury (years), age and sex (male/female). These meaningful comparisons will be viewed in relation to health, functioning and accessibility.
Qualitative data will be transcribed and analysed using a computer-assisted content analysis programme. Content analysis is expected to potentially reveal new information about the functioning and health of people with SCI, as well as information on the challenges experienced, which may receive less attention in the survey. It is assumed that content analysis will highlight experiences that are highly meaningful to the subjects. To identify the experiences and their meaning, part of the interview data will be analysed using a phenomenological analysis, which aims to gain a deeper understanding of the perspectives related to the everyday life and coping skills of people with SCI.
A formulation of the protocol produced 2 results: the number of subjects and the number of questions in a survey in the FinSCI study. At first, patient registers were investigated and a group of suitable participants was selected. The systematic data collection resulted in 2,322 subjects who had visited outpatient clinics over approximately 6 years. The inclusion criteria were not filled by 533 subjects. As a result, the number of suitable subjects in the FinSCI study is 1,789 (Fig. 1). The flow chart of the protocol and the selection process of subjects is presented in Fig. 1.
Fig. 1. Study design. SCI: spinal cord injury; MMC: meningomyelocele; AIS E: ASIA impairment scale; Oulu (OYS), Tampere (Tays) and Helsinki (HUS) University Hospitals
Secondly, the questionnaire was formulated. The final questionnaire consists of 151 ICF-linked questions. The overview of questions is presented in 3 tables (Tables III, IV and V). The tables show the 43 preselected FinSCI data-set ICF categories, the instruments and the number of final questions. These categories are covered by 124 questions. Altogether, The FinSCI study includes 64 categories because the SCI-specified measures and PROMIS Global Health were included as a whole. The additional 21 ICF categories, which include 27 questions, are not shown in the tables. In addition, some sociodemographic and background information is collected.
Table III. Overview of the Finnish Spinal Cord Injury Study questionnaire instruments to assess body functions
Table IV. Overview of instruments in the Finnish Spinal Cord Injury Study questionnaire to assess activity and participation
Table V. Overview of instruments in the Finnish Spinal Cord Injury Study (FinSCI) questionnaire to assess environmental factors
Fatigue, Global health, Sleep disturbance, Emotional distress depression, Pain interference and Pain intensity. In addition, AIS covers 1 ICF category (Table III).
The evaluation of activity and participation will be covered by 64 questions from 1 SCI-specific measure, FinSote, and 7 PROMIS domains (Table IV): Satisfaction with Social Roles and Activities, Illness Impact Positive, Physical Function, Self-Efficacy for Managing Symptoms, Satisfaction with Sex Life, Ability to Participate in Social Roles and Activities and Satisfaction with Participation in Discretionary Social Activities.
Environmental factors are measured using 2 SCI-specific measures, FinSote, PROMIS Emotional Support and questions set by the FinSCI Research group, and they are covered by 21 questions (Table V).
The FinSCI study is the first nationwide community survey for the SCI population in Finland. By gathering participants from every SCI outpatient clinic, FinSCI can reach most of Finland’s SCI population in need of special healthcare or services. Furthermore, it can reinforce and complete the survey collection by creating a dialogue between quantitative and qualitative data. This is unique internationally. The need for more patient-reported information has been acknowledged since 2016 when Finland signed the UN Convention on the Rights of Persons with Disabilities (UN-CRPD). We believe that true understanding can be gained only if the people who live with a certain health condition can report issues that are meaningful to them. At present, the ongoing InSCI survey is gathering data from 28 countries on 5 continents (17). Since FinSCI is using the same SCI-specified instruments as InSCI (SCI-SCS, SCIM-SR, NEFI-S), we have a great opportunity to combine and compare our results internationally. In addition, we deepen the data with interviews.
The applicability of studying functioning through ICF in people with SCI was already established in the early 2000s (33, 34). ICF has been seen as a comprehensive framework for describing factors related to health, functioning and environment in people with SCI (34). Previously, the functioning of people with SCI has been examined in only 2 cohort studies. In the Canadian study, the emphasis was on gaining understanding of the service needs of the SCI population (35). In the Swiss study, the ICF has been widely used to study functioning, health maintenance and quality of life (10, 36). The ICF long-term context Brief Core Set for SCI has been seen as the most important factor when describing functioning, health and participation among the SCI population. The rehabilitation Core Set is always recommended when reporting clinical settings (7). In the present study, all 4 Core Sets for SCI and the rehabilitation Core Sets are utilized by linking ICF categories to instrument items. The SCI-specific questionnaires are used as such, and by selecting the general questions in a selection process performed by 7 persons with SCI, the study contains the general questions that matter most to the SCI population in Finland. Some questions were formulated by the FinSCI research group since the SCI and generic specific questions did not cover all 43 chosen ICF categories.
The data and results from FinSCI are also greatly needed at the national level, since Finland has an ongoing reform to establish a regional government for health and social services. The purpose of this reform is to harmonize the state regional administration with the county government administration and to rationalize the organization of public-sector administration at the state, regional and municipal levels. As the primary solution, the Government Programme envisages the centralization of functions into clear autonomous regions (counties) in terms of tasks and authority. The main reasons for the reform are that people in different municipalities are not on equal ground regarding social or healthcare services (37). The results of the present study can offer unique data for planning and organizing equal services. FinSCI results will be implemented into all organizations dealing with the SCI population. Concerning the rarity of SCI, the degree of treatment complexity or special requirements in the provision of care, centralization of care and rehabilitation is still needed. FinSCI aims to provide new knowledge for healthcare professionals, political decision-makers and for people with SCI themselves.
The FinSCI study has some limitations. Participant selection was based on appointment registrations from each university hospital, and the data were collected for an approximate 6-year period. AIS classification was 1 inclusion criteria and was found in most of the patients, but 162 patients were dismissed for lack of it. Furthermore, not all subjects with SCI need the services of the outpatient clinics, or they might have had a congenital SCI, a progressive new NTSCI or other exclusion criteria. Nevertheless, this containment was deemed necessary to minimize confounding factors. Unfortunately, FinSCI could not join the InSCI study started earlier to collect data from different countries. Moreover, FinSCI has consciously left out legacy health-related quality of life instruments, which are usually regarded as sufficient to assess well-being and quality of life. Items in these instruments most often assess health and functioning, but in very general ways. For this reason, no separate measure concerning quality of life, except PROMIS Global Health, was included in the study.
We can learn what matters to the SCI population by generating new evidence of the health, functioning and accessibility of subjects with SCI. We believe that this new knowledge will offer guidance for better lifelong SCI rehabilitation and follow-up. The study results will be utilized in the development of care and rehabilitation policies of patients with SCI and in the planning of training models and information provided to various parties involved. University hospitals may utilize the results to develop their patient register systems. The cohort study will yield information on measures that could be employed in patient register systems to systematically monitor the functioning of people with SCI. The National Institute for Health and Welfare can utilize the results to harmonize regional data collection in the planning of social welfare and healthcare management. The Finnish Association of People with Physical Disabilities and the Finnish Association of Spinal Cord Injured Akson can use the results to advocate for people with SCI.
We thank the MD, PhD Heikki Numminen at the Department of Neurology, Tampere University Hospital for his support and advice in the research. This study was supported by the Finnish Association of People with Physical Disabilities (2017-2019), Oulu University Hospital (grant VTR 2017), Department of Internal Medicine and Rehabilitation, Helsinki University Hospital (grants HUS/53/2017 §9, 9.6.2017 and HUS/76/2018 § 11, 18.4.2018), and Validia Rehabilitation (grant HUS-VTR 9.3.2017).


 Click to show fullsize
Click to show fullsize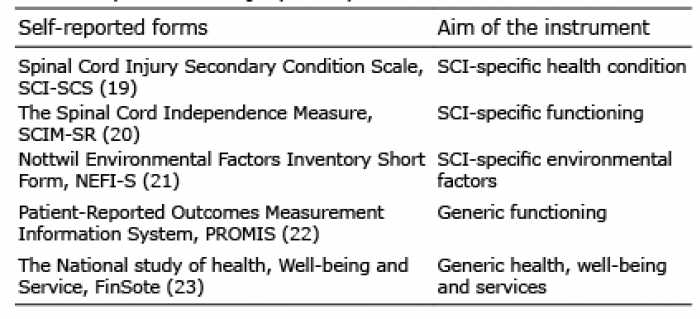 Click to show fullsize
Click to show fullsize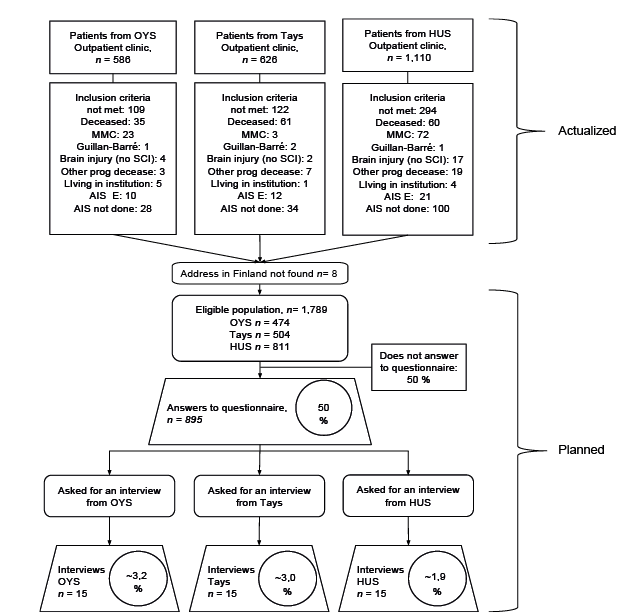 Click to show fullsize
Click to show fullsize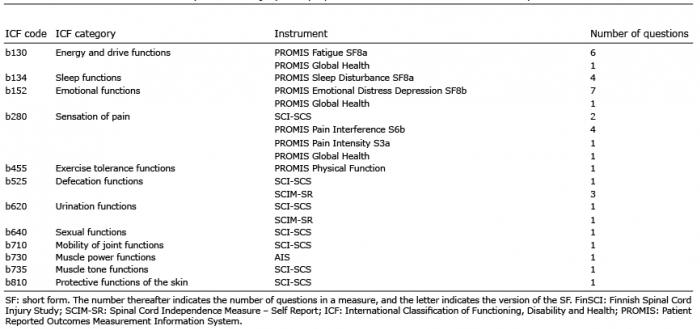 Click to show fullsize
Click to show fullsize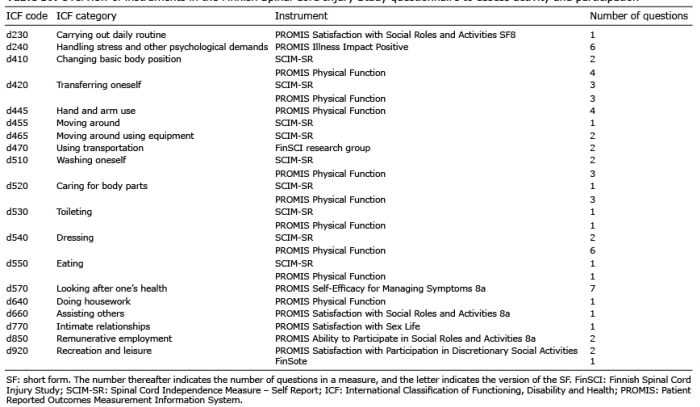 Click to show fullsize
Click to show fullsize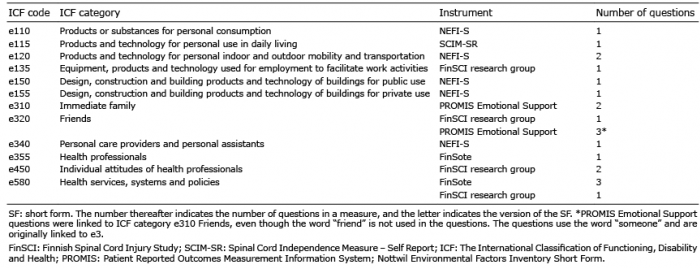 Click to show fullsize
Click to show fullsize