
From the 1Lund University, Department of Health Sciences, Research Group Rehabilitation Medicine, Lund, 2Skane University Hospital, Department of Pain Rehabilitation, Lund, 3Umeå University, Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå, 4Karolinska Institutet, Department of Clinical Sciences, Division of Rehabilitation Medicine, Danderyd Hospital, 5Danderyd University Hospital, Department of Rehabilitation Medicine and 6Karolinska Institute, Department of Neurobiology, Care Sciences and Society, Stockholm, Sweden
Objectives: To investigate: (i) changes in sick-leave benefits from 1 year prior to multimodal rehabilitation to 1 and 2 years after rehabilitation; (ii) sex differences in sick leave; and (iii) the impact of policy changes on sick leave.
Methods: All patients undergoing multimodal rehabilitation registered in a national pain database for 2007–11 (n = 7,297) were linked to the Swedish Social Insurance Agency database. Sick leave was analysed in 3-month periods: T0: 1 year before rehabilitation; T1: before start; T2: 1 year after; and T3: 2 years after rehabilitation. Four sick-leave benefit categories were constructed: no sick leave, part-time sick leave, full-time sick leave, and full-time permanent sick leave. The individual change in sick-leave category at each time-period was analysed.
Results: Sick-leave benefits increased from T0 to T1 (p <0.001) and decreased from T1 to T3 (p < 0.001). Reductions were significant for both men and women from T1 to T3, but men had less sick-leave benefits at T2 and T3. Positive changes in sick-leave benefits at T2 and T3 were found both prior to and after policy changes, with less sick-leave benefits after policy changes at all time-points.
Conclusion: Multimodal rehabilitation may positively influence sick-leave benefits for patients with chronic pain, regardless of their sick-leave situation, sex or policy changes.
Key words: chronic pain; rehabilitation; registries; return to work; sick leave.
Accepted Feb 26, 2019; Epub ahead of print Mar 8, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Marcelo Rivano Fischer, Lasarettsgatan 13, 221 85 Lund, Sweden. E-mail: marcelo.rivano@med.lu.se
This study investigated changes in sick-leave benefits from 1 year before multimodal rehabilitation to 1 and 2 years after rehabiliation. The study also examined differences in sick leave between men and women, and whether sick-leave policy changes influence patterns of sick leave. All patients receiving pain rehabilitation in 2007–11, who were registered in both the national pain database and the Swedish Social Insurance Agency database, were included in the study. Sick leave was analysed 1 year before rehabilitation, before the start, 1 year after, and 2 years after rehabilitation. It was shown that sick-leave benefits increased during the year before rehabilitation and decreased after rehabilitation. These reductions in benefits were significant for both men and women. Positive changes in sick-leave benefits at follow-up were found both before and after policy changes, with less sick-leave benefits after policy changes at all time-points. In conclusion, multimodal rehabilitation has a positive impact on sick-leave patterns for patients with chronic pain, regardless of their sick-leave situation, sex, or policy changes.
Chronic pain, a major health and socioeconomic problem, often causes long-term work absenteeism. In a European survey 19% of the population reported chronic pain. Of those, 34% reported severe pain, 21% were diagnosed with depression due to pain, 61% were unable to work outside home, and 20% lost their work due to pain (1). In Sweden, it has been reported that people with musculoskeletal chronic pain have a mean of 46 days’ sick leave per year (2). In Europe, large differences in return to work (RTW) after sick leave due to back pain are associated with differences in the countries’ regulations on work interventions and sick-leave benefits (3). Major policy changes were effected in Sweden in July 2008, aimed at speeding up rehabilitation processes, reducing benefit levels, and establishing an upper time-limit for sick leave. The changes were fully implemented in 2009.
Risk factors for disability pension were investigated in a population-based cohort study in Sweden. Higher age, low income, previous sick-leave history and not being born in Sweden increased the risk of disability pension. For women, the highest risk factor was musculoskeletal pain (4).
Multimodal rehabilitation (MMR) is the gold standard for managing the consequences of chronic pain (5); studies indicate better outcomes on RTW than unimodal interventions. A Swedish study (6) showed the strongest effects of MMR on RTW in female participants, with substantial impact on costs for production losses, while no improvements were observed for men on health-status or costs. One meta-analysis on low back pain rehabilitation in Europe (7) showed limited effects on RTW, but the effect was larger if restricted only to Scandinavian settings. In addition, positive effects of MMR on RTW were reported to persist 3, 6 and 10 years after intervention (6, 8, 9), economic benefits being estimated as €3,799–€7,515 per treated patient and year (9).
However, the positive effect of MMR on RTW is questioned (10, 11), and there is no consensus on how to assess changes in sick-leave benefits due to MMR. Different methods to track RTW and work ability are used, from self-reports to information from social insurance agencies (6, 7, 12).
Since previous studies exploring patterns of sick leave have usually focussed on changes observed in the years following MMR, there is a need for studies that include a time-period prior to admission in order to increase knowledge about the sick-leave process for patients included in MMR and to further investigate the influence of MMR on RTW.
This study aimed to investigate: (i) changes in patterns of sick leave from 1 year prior to MMR to admission to MMR; (ii) changes in patterns of sick leave from admission to 1 and 2 years after MMR; (iii) sex differences in patterns of sick leave; (iv) the impact of policy changes in the sick-leave benefit system on patterns of sick leave.
This is a multicentre, register study with a retrospective design. Data were collected from the 31 rehabilitation units at specialist care level reporting to the Swedish Quality Registry for Pain (SQRP) during 2007–11.
The SQRP aims to monitor health status prior to and after MMR for patients with chronic pain, to allow for comparisons between units and to enable audits for single units as well as outcome studies in Sweden (13). All units offered an MMR programme with at least 3 professionals working with a cognitive behavioural therapy (CBT)-based approach. Physicians, physical therapists, psychologists, occupational therapists, socials workers and nurses usually staffed the rehabilitation teams. Medical secretaries were available to all teams.
The registry was established in 1998 and became web-based in 2009. Ninety percent of the operationally active tertiary units at that time in Sweden (31 in June 2015), reported patient data during the data collection period.
The questionnaires used in the SQRP cover variables recommended by national and international guidelines for the description of health-related domains of patients with chronic pain and for the follow-up of outcomes of pain rehabilitation (14, 15). Furthermore, the health-related categories (physical and psychological functioning, activity and participation) in the International Classification of Functioning, Disability and Health (ICF) are included, as well as socio-economic and socio-demographic variables (16).
The patients participating in MMR complete questionnaires before, after and at a 1-year follow-up after MMR. The units collect data following SQPR’s written instructions (22). The questionnaires are either posted to patients prior to a first visit or administered on site. After MMR the questionnaires are mostly administered on site. The 1-year follow-up is usually sent by post, including one reminder.
The SQRP questionnaire includes socio-demographic factors (sex, age, educational level and referral sources), pain duration, intensity and location, as described by Nyberg et al. (13). The Hospital Anxiety and Depression Scale (HADS) and the Multidimensional Pain Inventory (MPI), also included in the SQPR, were used here.
The HADS aims to detect symptoms of anxiety and depression in non-psychiatric medical settings (17). It includes 14 items, ranging from 0 to 3. A total score is calculated both for anxiety (7 items) and for depression (7 items). Cut-off levels for no, mild and severe symptoms are 0–7, 8–10 and 11–21, respectively. Both the English original and the translated Swedish version have acceptable validity and reliability (17, 18).
The MPI (version 2) measures pain-related functioning (19), including 61 items and 13 subscales. All items ranges from 0 (never) to 6 (very often). Four subscales were used in this study: pain severity, life interference, life control, and affective distress. The original MPI with satisfactory psychometric properties (19, 20), is translated to Swedish and described by Nyberg et al. (21).
People in Sweden with a sick-leave period longer than 2 weeks are included in the Swedish Social Insurance Agency (SSIA) database. In Sweden sick-leave benefits are decided according to cut-off levels of 25%, 50%, 75% and 100%, based on the actual level of employment.
In this study, data were retrieved from the SSIA database and included all patients registered in the SQRP with discharge from a MMR programme at the pain rehabilitation units from 2007 to 2011. The extent of sick leave reported in the SSIA database for each patient 1 year prior to admission, before the first visit to the units, 1 year and 2 years after discharge was used for statistical analyses. The extent of sick leave before MMR was also analysed by comparing 3-month periods for 12 months prior to MMR.
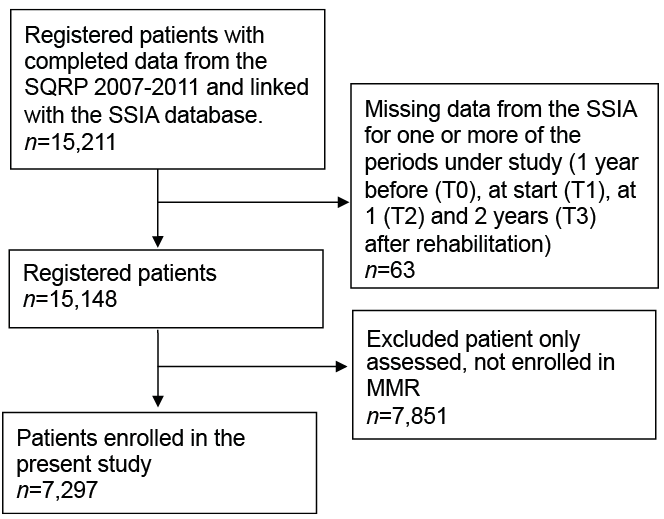
Patients who participated in MMR at specialist (tertiary) level in Sweden and who were registered in the SQRP and the SSIA between 2007 and 2011 were considered eligible. In total 7,297 patients undergoing MMR during the specified time-frame were included in the study (Fig. 1).
Fig. 1. Inclusion process of study participants from Swedish Quality Registry for Pain (SQRP) and Swedish Social Insurance Agency (SSIA).
Data from the SQRP were linked to the SSIA database to obtain information as to what extent patients were benefitting from sick leave prior to and after MMR. The linked data from the SQRP and the SSIA resulted in a database used for statistical analysis.
According to Swedish law, the first 14 days of sick leave are not registered by the SSIA, but paid for by the employer. Long-term sick leave was defined in this study as a period of 28 or more days of work absence due to sickness. This meant that patients with sick leave had at least 14 consecutive days of registration at the SSIA database during any given period defined by this study. Each patient was sequentially followed during a period of 3 years: from 1 year prior MMR to 2 years after discharge.
In order to analyse changes in patterns of sick leave the selected measurement points were defined as periods of time. To analyse changes occurring before MMR, the 12-month period prior to MMR was divided into trimesters. Two of these were included in the statistical analyses. The first ranged from 365 to 273 days before the start of MMR (T0). The second ranged from 90 to 0 days before the start (T1). The 1-year follow-up measuring point was defined as a period ranging from 320 to 410 days after discharge from MMR (T2), and the measurement point at 2 years follow-up was defined as a period ranging from 685 to 775 days after discharge from MMR (T3).
In this study, 4 categories of sick-leave benefits were constructed based on: (i) the extent of benefit (full-benefits, partial benefits and no benefits) and (ii) the length or duration of sick leave (temporary and/or permanent). The categories are described below:
Work ability should not be defined in terms of sick leave. This study assumes that the degree of sick leave registered in SSIA usually indicates the degree of absence from the workplace. The category full-time permanent sick leave includes persons assumed to be absent from work with permanent lack of working ability or absent from work for more than 2 years. The category full-time sick leave includes combinations of either only temporary or combinations of temporary and permanent sick leave. This category was created under the assumption that it included persons with less deteriorated work ability than the category full-time permanent sick leave. The category temporary sick leave includes persons assumed to be without work ability for up to a maximum of 2 years.
Descriptive data are presented as medians and 25th–75th percentiles for ordered categorical data. Differences in number of patients in the 4 categories of sick leave within the sample over time, at T1, T2 and T3, were analysed by Friedman’s analysis of variance (ANOVA) by ranks. Wilcoxon signed-rank test was used as post-hoc analysis and for analysis of difference between groups at the different time-points and Mann–Whitney U test within groups at different time-points.
SPSS for Windows version 24.0 was used for all statistical analyses. The level of significance was set at p < 0.05.
Men and women were analysed separately in order to explore and describe their patterns of sick leave.
Participants in MMR were separated into 2 groups; one group “before” policy changes, year 2007–08 (n = 16,02) and one group “after” policy changes, year 2009–11 (n = 5,695). The groups were analysed separately to examine whether policy changes in sick-leave benefits affected the levels of sick leave for patients registered in SQPR 2009–11 compared with 2007–08.
This study followed the principles of the Declaration of Helsinki, and the study was approved by the Regional Ethical Review Board in Lund, Sweden (Dr 2018-31). The data were collected as part of the ongoing quality control of clinical care activities in the participating clinics, and stored with the consent of the National Swedish Data Inspection Agency (permission number 1580-97). Informed consent was received and participation was entirely voluntary.
The patients’ characteristics are shown in Table I. Most patients (67%) were referred from primary care. One-third of patients reported several pain locations, and more than 50% reported mild or severe symptoms of anxiety or depression according to HADS. Patients also reported severe negative life interferences due to pain (MPI).
Table I. Description of background data on all patients in multimodal rehabilitation (MMR); n=7,297
There was a significant change in the distribution of sick-leave benefits among the participants during the year before rehabilitation (p < 0.001), with a larger percentage of full-time and partial sick leave and a smaller percentage of no sick leave at T0 compared with T1. Fig. 2 illustrates the percentage of patients in the different categories of sick leave at the different time-points.
Fig. 2. Level of sick leave at 4 3-month periods of time: 365–273 days (T0), 272–182 days, 181–91 days before multimodal rehabilitation (MMR), and 90–0 days (T1) before MMR; n = 7,297.
There was a significant change (p < 0.001) in the distribution of sick leave among the participants from T1 to T3, with the percentage in the no sick-leave category increasing from T1 to T3 and the percentage in the other categories decreasing from T1 to T3. Fig. 3 illustrates the percentage of patients in the different categories of sick leave at the 3 time-points. Post hoc analysis showed a significant reduction in the percentage of patients with sick leave between T1 and T2 (p < 0.001) and between T2 and T3 (p < 0.001).
Fig. 3. Level of sick leave at 90–0 days before (T1) multimodal rehabilitation (MMR), 320–410 days after (T2) MMR and 775–985 days after (T3) MMR; n = 7,297.
Changes in sick leave categories for each patient from T1 to T2 and T3 are illustrated in Table II. Of the patients belonging to the no sick leave category at T1, 77% remained at T2. The percentage remaining in the no sick leave category increased further to 85% at T3. Of the patients belonging to the partial sick leave (temporary and/or permanent) category at T1, 38% moved to the no sick leave category at T2. At T3 a total of 54% had moved from the partial sick leave to the no sick leave category. Of the patients in the full-time sick leave (temporary or mixed temporary and permanent) category at T1, 42% had moved to the no sick leave category at T2, and at T3 a total of 58% had moved from the full-time sick leave to the no sick leave category. Most patients in the full-time permanent sick leave category at T1 remained in the same category at T2 (64%), and 46% remained in the full-time permanent sick leave category at T3. Nevertheless, 21% of those in the full-time permanent sick leave category at T1 were in the no sick leave category at T2 and the share increased further, resulting in 30% moving to the no sick leave category at T3.
Table II. Description of individual changes in each category of sick leave from before multimodal rehabilitation (MMR) to 1 and 2 years after MMR; total n = 7,297
Changes in sick leave category from T0 to T1 (p < 0.001) and T1 to T3 (p < 0.001) were found in both men and women (Table III).
Table III. Percentage and number of men (n = 1,898) and women (n =5,399) on each category of sick leave at 1 year before multimodal rehabilitation (MMR) (T0), before MMR (T1), 1 year after (T2) and at 2 years after MMR (T3)
There were no differences between men and women in categories of sick leave at T0 and at T1 (p = 0.24 and p = 0.69, respectively), at T1 35% of the men and 30% of the women were on full-time sick leave. At T2 sick-leave benefits decreased more for men than for women (p < 0.001), e.g. the category full-time sick leave decreased 16% for men and 11% for women. At T3 the difference between men and women remained (p < 0.001) and the category full-time sick leave continued to decrease, from T2 to T3 (8% for men and 7% for women).
There were no significant differences between the patients admitted before policy changes (n = 1,602) and after policy changes (n = 5,695) with respect to sex, educational level, depression, pain severity, pain-related interference or affective distress. Patients admitted after policy changes were older (p < 0.001), had longer pain duration (p = 0.006), higher levels of anxiety (p = 0.004) and reported more life control (p < 0.001) (Table IV). Significant changes in sick-leave category were found in both groups (before and after policy changes, respectively) from T1 to T2 to T3 (before (p < 0.001), after (p < 0.001). The numbers and percentage of patients per sick-leave category in T1, T2 and T3 for the group before (2007–08) and the group after (2009–11) policy changes are described in Table V.
Table IV. Description of background data on patients in multimodal rehabilitation (MMR), before and after 2009, and p-values for statistical differences on background variables between the 2 time-points
Table V. Percentage and number of patients in the 4 categories of sick leave for the time period before 2009 (n = 1,602) and after 2009 (n = 5,695) 1 year before multimodal rehabilitation (MMR) at (T0), before MMR (T1), at 1 year after MMR (T2) and at 2 years after MMR (T3)
At all time-points the group after policy changes received less sick-leave benefits compared with the group before policy changes T0 (p < 0.001), T1 (p < 0.001), T2 (p < 0.001), T3 (p < 0.001). The percentage of patients on full-time sick leave was higher in the group before policy changes (37%) than in the group after policy changes (30%) and the percentage with no sick leave in the group before policy changes (26%) was lower than that of the group after policy changes (37%). At T3 the percentage with no sick leave increased, in the group before policy changes to 46% and in the group after policy changes to 68%.
The main finding of this study was an observed decrease in sick-leave benefits during 2 years after MMR. This is the first study to include all participants in the SQRP during 2007–11, including most participants in MMR at the tertiary level, and combining data from these patients with data from the SSIA database. To our knowledge, the SQRP is a unique national database for people with complex problems due to non-malignant chronic pain. This study also presents data on the escalating sick-leave benefits during the year prior to inclusion in MMR, providing valuable information about the sick-leave process in patients with complex chronic pain.
These results underline that time is an important factor to consider in evaluating the process of RTW after rehabilitation. Furthermore, the results of this study indicate that patterns of sick leave should be assessed during long periods of time, both before and after rehabilitation. The changes observed prior to MMR indicate that patients gradually increased their absence from work, suggesting a deterioration in their work-related activities prior to and leading up to MMR. The changes observed after rehabilitation indicate that MMR positively influences levels of sick-leave benefits. Busch et al., in 2011, showed a similar pattern in their 10-year follow-up; the total amount of sick-leave decreasing up to 2 or even 3 years after rehabilitation (22). The results, however, are inconclusive, and in a recent Norwegian study, Brendbekken et al. (23) reported that the level of improvement found after 1 year stabilized 2 years after rehabilitation. No previous study, however, has yet included patterns of sick leave prior to rehabilitation in the analyses; an area to which the current study contributes valuable information.
In addition, these results show a shift from full-time sick leave to no sick leave or partial sick leave categories when comparing patterns of sick leave from the year before to 2 years after MMR, which in agreement with other findings (22, 24–26).
The current results were achieved in a national population of patients with chronic pain with reported complex and negative pain-related consequences, involving psychological, social, and activity-related problems, as illustrated by the demographic and background data. Compared with the participants in studies by Busch et al. (22) and Jensen et al. (6), the participants in the current study had longer duration of pain and more complex emotional disturbances.
Analyses of aggregated sick-leave data at different time-points, without discerning how sick leave changes both in type and extent of benefit for each individual, may fail to apprehend important variations that, at the individual level, are crucial for patients regaining areas of autonomy and increased activity. For example, the proportion of patients in the full-time permanent sick leave category at T1, T2 and T3 appears to be stable over time, at 11–12%. It might then, erroneously, be argued that MMR has no RTW effect in this group. Our analyses showed that this is not the case. On the contrary, MMR seems to be associated mainly with positive changes in all sick-leave groups, including the full-time permanent sick leave category. Even though the share is stable, the patients in the category are not the same at the different time-points. Approximately 30% of patients in the full-time permanent sick leave category prior to MMR were in the no-sick leave category 2 years after MMR, indicating that almost one-third of the patients that started MMR in the full-time permanent sick leave category were no longer on sick leave at all. On the other hand, 10% of patients in the full-time sick leave (temporary or mixed temporary and permanent) category prior to MMR shifted to the full-time permanent sick leave category 2 years after MMR, suggesting that, as many clinicians would claim, MMR may be effective in stopping fruitless rehabilitation efforts for individuals who are not able to return to work. To our knowledge, there are no other studies reporting similar analyses.
In this study, the patterns of sick leave changed significantly for both women and men, but when analysing sex differences at different time-points, it was found that men changed to a more favourable category of sick leave and, hypothetically, gained more from MMR. Sex has earlier been found to significantly influence the risk of full-time permanent sick leave 10 years after rehabilitation; women having a relative higher risk than men of being on permanent disability pension (22). When studying the long-terms effects of rehabilitation on RTW for patients with back pain, women benefitted the most after 3 years (6), but after 10 years no differences were found between men and women. Our patients represent a wide range of diagnoses, from local to widespread pain, and this may have influenced the outcome.
The social insurance system in Sweden underwent major changes in 2008. According to Anema et al. (3), these changes probably influence patterns of RTW, and therefore some differences in patterns of sick leave due to policy changes were expected in this study. Thus, we controlled for the policy changes in the sickness benefit system, by analysing data in both periods separately, before and after implementation of the new regulations. The results indicate that the regulatory changes in the benefit system entailed a positive change in reducing levels of sick leave, corroborating findings from previous research on the impact of regulation and law changes in benefit levels in RTW (3, 27). Furthermore, the regulatory changes might have impacted on decisions about referral to MMR, as some differences were found between the groups regarding duration of pain, levels of anxiety and life control. Nevertheless, the positive changes in sick-leave benefits after rehabilitation were significant for both periods, before and after policy changes, indicating that MMR per se had an impact on the patients’ patterns of sick leave, in addition to policy changes.
This study analysed sick-leave benefits by linking information from SQRP to data from a national insurance agency database (SSIA). Data from the SSIA on sick-leave benefits is more valid than self-reported data (7) and probably more reliable. This study is, to our knowledge, the first attempt to publish sick-leave data on a national level from specialized pain rehabilitation units. The large number of patients included (n = 7,297) and the geographical spread make the data highly representative for this patient group over the whole country. Previous studies often have transformed patients’ different uses of sick-leave benefits into the total number of days of sick leave (22, 28, 29). We intended to analyse the extent and length of sick leave through an extended timeline in a large sample of patients undergoing MMR by selecting specific time periods prior to and after MMR. However, due to methodological differences between the current and previous studies, comparisons were not feasible. We would argue that the methods used elucidate different aspects of the sick-leave spectrum; ours focussing on processes, and others focussing on total amounts.
This is not a controlled design study, thereby generalization of the results is limited. The effect of rehabilitation on sick-leave benefit levels can therefore not be fully established. On the other hand, the sample size, the large period under observation, and the frequently repeated observations, following each person, allows for some conclusions to be drawn regarding the changes observed.
One way to make comparisons between time periods is to find appropriate control subjects or a reference group (not subjected to the studied intervention) (9). However, there are problems inherent in the identification of adequate controls, the main one being the assumption that patients referred to MMR or other treatments are alike. Referral sources, usually physicians, make judgements before deciding whether to send patients to pain rehabilitation, judgement weighting several aspects. Therefore, important variables that should be controlled for in any matching procedure, such as functioning, activity levels, and motivation for change, cannot be controlled for by matching the usual variables, diagnoses, age and sex. Furthermore, patients with pain who are not referred to a specific rehabilitation may seek healthcare in other places, which may often not have been controlled for. A study reported by Post Sennehed found ”limited feasibility in identifying 2 comparable groups for evaluation of the multimodal rehabilitation programme” (30). Our study, therefore, approached the problem by using a large sample and repeated measures over an extended period of time, in order to obtain answers as to whether MMR has an impact on sick-leave benefits.
Future research
The possibility of linking SQRP data to the SSIA database opens up several avenues for future research. One such area is that of identifying subgroups of patients participating in MMR in relation to changes in their patterns of sick leave. Other areas refer to possible associations between patterns of physical, psychological or activity-related limitations reported by patients and patterns of sick leave, the prediction value that patients’ self-descriptions might have on patterns of sick leave, and how work conditions interact with outcomes of MMR at long-term follow-up after interventions.
Conclusion
Since the extent of sick-leave benefits seems to increase during the year prior to participating in MMR and decrease during 2 years after rehabilitation, the results of this study highlight the importance of offering MMR to patients with chronic pain. The results, based on data from 2 large national databases, indicate that MMR has an impact on sick-leave benefits regardless of sex or policy changes in the sick-leave benefit system.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize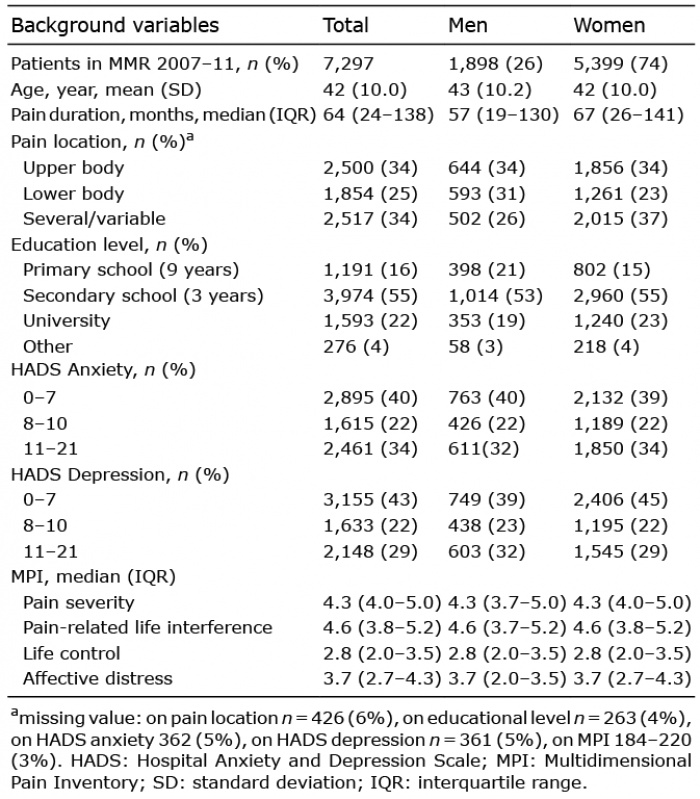 Click to show fullsize
Click to show fullsize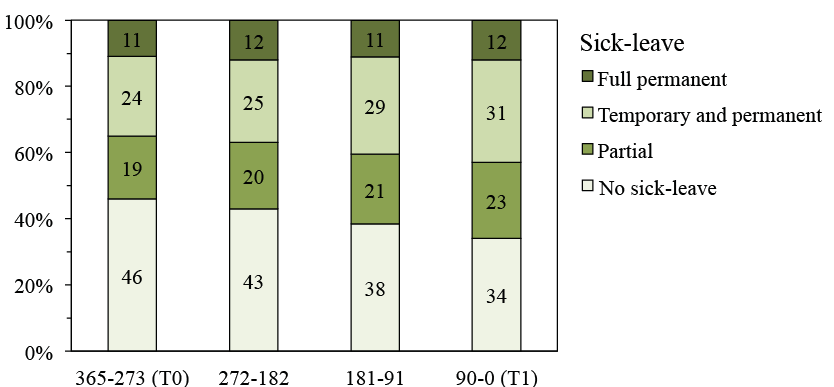 Click to show fullsize
Click to show fullsize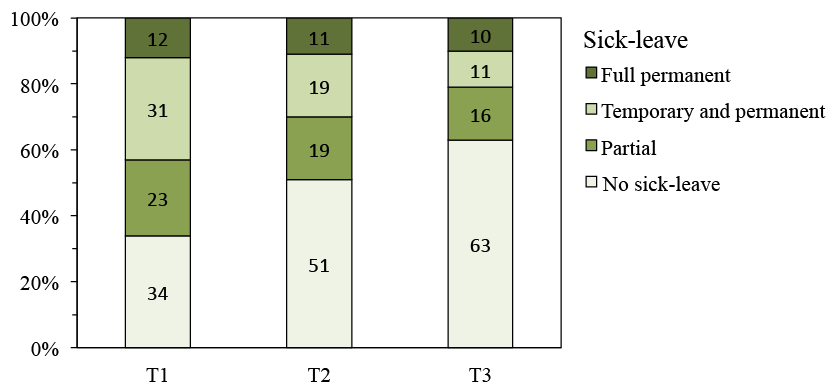 Click to show fullsize
Click to show fullsize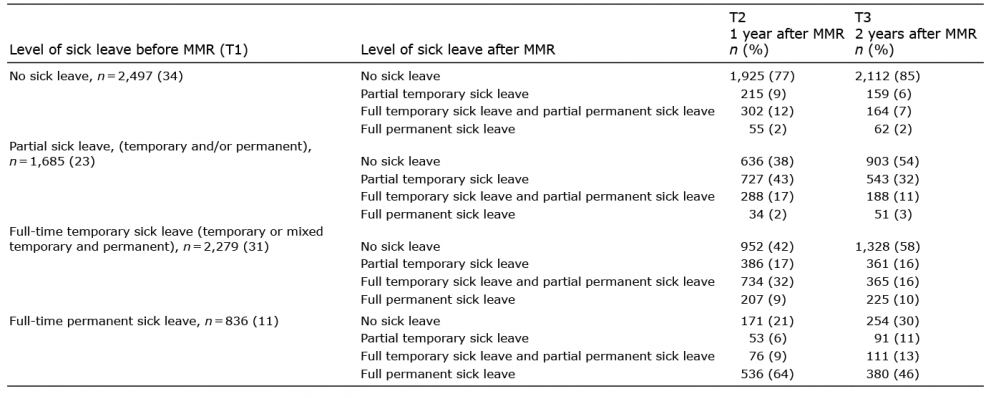 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize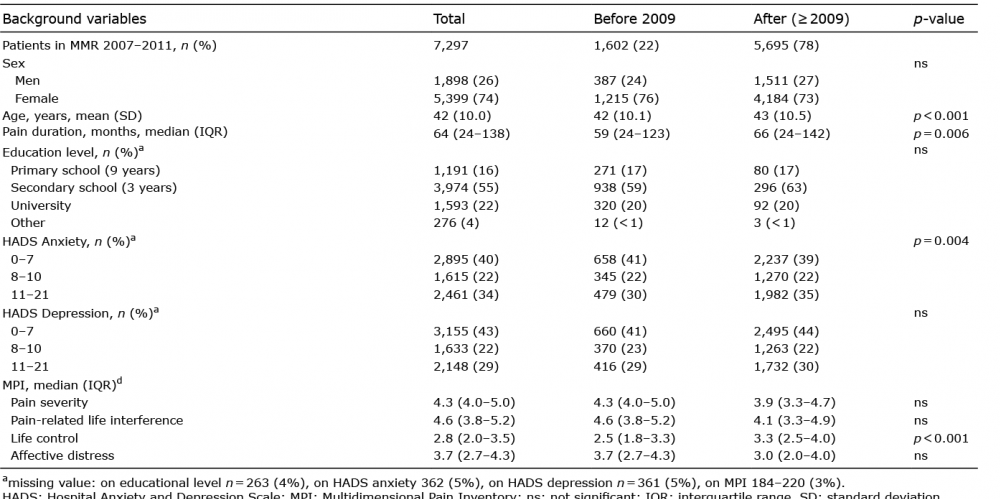 Click to show fullsize
Click to show fullsize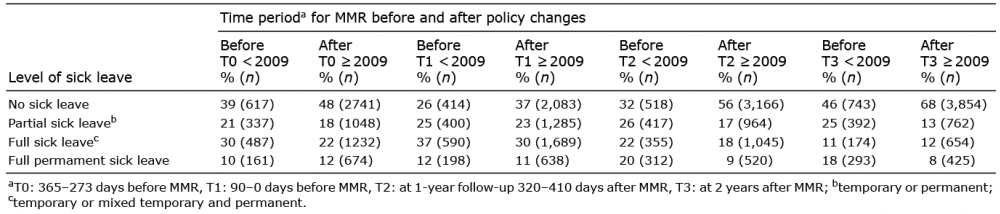 Click to show fullsize
Click to show fullsize