
Objective: An increase in numbers of cases of sick leave due to stress have been reported from several European countries during recent decades. Chronic stress-induced exhaustion disorder is associated with physiological and neurobiological perturbations that may contribute to cognitive problems and long-term exhaustion. Rehabilitation of patients with
chronic stress-induced exhaustion disorder is therefore challenging. This narrative review summarizes the evidence regarding the effectiveness of different interventions for the rehabilitation of patients with chronic stress-induced exhaustion disorder.
Methods: Both structured and unstructured searches of research studies and reports were performed in order to find knowledge sources. The structured search had 2 predefined inclusion criteria: (i) chronic
stress-induced exhaustion/clinical burnout/severe burnout/stress-induced exhaustion; and (ii) rehabil-itation with improvement of symptoms and/or
return to work as outcomes.
Results: Cognitive behavioural interventions and multimodal interventions seem to reduce symptoms. Workplace interventions, either work-focused cognitive behavioural or workplace dialogue, seem to improve return to work. Sleep is important for both symptom improvement and return to work, and interventions for improving sleep might therefore be important. For improvement of cognitive function, which is a main complaint among patients with chronic stress-induced exhaustion disorder, aerobic and cognitive training may have some effect.
Conclusion: In summary, the few studies of high-quality that examine interventions for rehabilitation of chronic stress-induced exhaustion disorder show only marginal effects. Thus, it is important to prevent the onset of chronic stress-induced exhaustion disorder.
Key words: stress; exhaustion; burnout; fatigue; intervention; return to work.
Accepted Feb 26, 2019; Epub ahead of print Mar 18, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Johanna Wallensten, Department of Clinical Sciences, Karolinska Institutet, Danderyd Hospital, 18371 Stockholm, Sweden. E-mail: Johanna.Wallensten@ki.se
There has been an increase in cases of sick leave due to stress in several European countries in recent decades. Chronic stress-induced exhaustion disorder is linked with physiological and neurobiological changes, which may add to cognitive problems and long-term exhaustion. This narrative review summarizes the published evidence about the effectiveness of different interventions for the rehabilitation of patients with chronic stress-induced exhaustion disorder. Cognitive behavioural interventions and multimodal interventions reduce symptoms. Workplace interventions often improve return to work. Better sleep is associated with improvement of symptoms and return to work. Interventions for improving sleep might therefore be important. For improving cognitive function, which is a main complaint among patients with chronic stress-induced exhaustion disorder, aerobic and cognitive training may have some effect. Most interventions for the rehabilitation of chronic stress-induced exhaustion disorder have only marginal effects. Therefore, it is important to prevent the onset of this disorder.
Increasing numbers of cases of sick leave due to stress have been reported from several European countries during recent decades (1). In Sweden, adjustment disorder and reaction to severe stress have been the most common reasons for more than 14 days of sick leave since 2014, and chronic stress-induced exhaustion disorder is associated with long periods of sick leave (2).
Medical and psychological nomenclature for exhaustion after a long period of severe stress differs between countries and disciplines. The term “burnout” is commonly used. Burnout is a psychological concept defined by emotional exhaustion, depersonalization, and lack of personal achievement as a response to chronic occupational stress (3, 4). In the International Classification of Diseases, tenth version (ICD-10), burnout is not regarded as an illness, but as a “factor which influences health status”, which is reflected in the Z-code used for the condition. The ICD code for burnout is Z73.0. Z73 includes “problems related to life management difficulty”.
Long-term chronic stress can, however, lead to a state of exhaustion that has the character of an illness, which is associated with changes in brain structure and function as well as biochemical aberrations (5–9). If such physical and mental exhaustion is induced by a long-lasting period of high levels of stress without sufficient recovery, the term chronic stress-induced exhaustion disorder or exhaustion disorder (SED) may be used. SED is classified as an illness in the Swedish version of ICD-10 since 2004. The term SED is used in this paper when referring to studies that have used diagnostic criteria for SED. The diagnostic criteria for SED are described in Table I.
Table I. Criteria for chronic stress-induced exhaustion disorder (SED) according to the Swedish National Board of Health and Welfarea
There are equivalents to SED in the international literature, such as chronic burnout (10), clinical burnout (9, 11), stress-related exhaustion (12), job stress-related depression (13, 14) and, possibly, neurasthenia (15). Clinically, the diagnosis SED is often subsumed under depression or adjustment disorder. However, the main symptom in SED is exhaustion, and not depressive mood. In SED symptoms of depression and anxiety can be present, but are rarely the major complaint. Typical of SED are markedly reduced mental energy, lack of endurance, and increased time needed for recovery after mental effort. Somatic symptoms are common. Many patients experience symptoms of the digestive tract, nausea, gas and indigestion, headaches, and dizziness. These symptoms often decline with time (16).
Cognitive impairment and structural differences in the brain. Imaging studies comparing patients with SED and controls have shown structural and functional differences in the brain (5, 17–20). Patients with SED demonstrate thinning of the prefrontal cortex (PFC), the anterior cingulate cortex (ACC), left superior temporal gyrus (STG), and reduced volumes of caudate and putamen in the basal ganglia. Thinning of the PFC and reduced volumes of caudate was correlated with perceived stress, implying a possible causal link (5). In addition, thickness of PFC as well as altered functional couplings in the emotion- and stress-processing limbic networks was correlated with an impaired ability to down-modulate response to emotional stress (17). Prolonged stress has been shown to cause morphological changes in the hippocampus, including suppressed production of new neurones in the dentate gyrus regions of the hippocampus (21). These changes correspond to deficits in spatial navigation and episodic memory (22, 23).
The brain areas with altered volumes in patients with SED are important for cognitive function, such as attention, executive functions and memory. Similar structural changes have been found in persons who have experienced early life traumas and among persons with PTSD (5).
Cognitive impairment may last for several months or even years, in patients with SED (24). In a prospective cohort study, patients with work-related stress performed worse than controls when assessing memory, mental speed and executive function in a neuropsychological test at follow-up 1 year after inclusion (25). Long-lasting cognitive impairment is also supported by a magnetic resonance imaging (MRI) study demonstrating that thinning of PFC among patients with SED normalized during a follow-up of 1–2 years (7).
Prolonged course and downregulation of the hypothalamic pituitary adrenal axis. During stress 2 main systems are activated; the sympathetic system, and the hypothalamus, pituitary and adrenal axis (HPA axis). When the HPA axis is activated cortisol is released from the adrenal gland. Patients with SED seem to have decreased ability to mount a stress response in the HPA axis. Testing the HPA axis by measuring cortisol response to corticotrophin-releasing hormone (CRH) after dexamethasone pre-treatment demonstrated blunted cortisol response in women with SED compared with controls, both at baseline and after 7 years’ follow-up (13, 14). This finding may support the observed prolonged course that the patients experience (13, 26). The finding is also in accordance with a meta-analysis by Miller et al., showing that stress gives an initial activation of the HPA axis, but, with time, the activity diminishes (27).
The aim of rehabilitation is to achieve and maintain optimum functioning in individuals who experience or are likely to experience disability (28). Patients with SED demonstrate physiological and neurobiological perturbations that may contribute to prolonged cognitive problems and exhaustion. Rehabilitation of patients with SED is therefore challenging. In addition, patients with SED need to evaluate stress factors in their everyday lives and often learn stress management skills in order to prevent relapse. Many different interventions for rehabilitation of these patients have been tried.
This narrative review aims to summarize the evidence for different interventions for SED, with symptoms and return to work (RTW) as primary outcomes. RTW is a particularly stringent test of a positive outcome, since the condition is often induced by work stress.
Both structured and unstructured searches of research studies and reports were used in order to find knowledge sources for this review. The structured search, performed in April 2017, had 2 predefined inclusion criteria: (i) chronic stress-induced exhaustion/clinical burnout/severe burnout/stress-induced exhaustion; and (ii) rehabilitation with improvement in symptoms and/or RTW as outcomes. The search was performed in PubMed, PsycINFO, Web of Science and Clinical Trials, searching for “clinical burnout” or “severe burnout” or “stress induced” and “exhaustion”. A total of 441 articles were found. After excluding studies that did not test interventions, studies that were not in human beings, studies without a control group, and studies that were duplicates, only 3 studies met the 2 predefined inclusion criteria. These studies are shown in Table II.
Table II. Studies from the structured search fulfilling the inclusion and exclusion criteria
The unstructured search was based on the authors’ knowledge as active researchers and clinicians in the field. Some meta-analyses, RCTs and cohort studies including populations other than SED are discussed in this narrative review if a general effect of an intervention was of interest, or if persons with SED were likely to be included in the population, but categorized in another way. These studies contribute to the overall knowledge of rehabilitation of SED, but do not fulfil the predefined inclusion criteria of the structured search. The studies from the structured and unstructured searches are presented both in the text and Tables, divided into 2 main groups: (i) psychological and stress-reducing interventions; and (ii) workplace-oriented interventions. However, the order of the studies within these groups is presented slightly differently, since the Tables show chronological order, which was not always feasible in the text. Table III shows only those studies in which the outcome RTW was included.
Table III. Studies on populations with stress-related exhaustion and outcome return to work (RTW) from the unstructured search divided into psychological and/or stress-reducing interventions, psychological and/or stress-reducing interventions + workplace-oriented interventions and workplace-oriented interventions.
Cognitive behavioural interventions (CBI) and multimodal interventions (MMI) seem to be the most effective stress management interventions, at least for symptom reduction (29, 30). CBI work by changing attitudes and behaviour by focusing on thoughts, images, beliefs and attitudes. CBI can be used, individually or in a group setting, as one of several treatment modalities in multimodal rehabilitation (MMR) of SED.
A meta-analysis by van der Klink et al. in 2001 (30) included 48 studies designed to prevent or reduce psychological complaints related to occupational stress in a working population with imminent or manifest stress-related psychological problems. The meta-analysis found a moderate effect for CBI and MMI, and a small effect for relaxation techniques, in reducing psychological complaints. Only 4 studies measured absenteeism, in which no effect was seen for interventions with a cognitive approach or relaxation techniques. Interestingly, CBI showed an inverse correlation between the number of sessions and effect size, indicating that shorter programmes might be more effective (30).
A systematic review by Richardson & Rothstein in 2008 (29), aimed to update the meta-analysis by van der Klink by including an additional decade of studies, both published and unpublished sources, but including only those interventions evaluated by a true experimental design including randomization of participants and control groups. The systematic review included 36 studies representing 55 interventions coded into multimodal, CBI, relaxation, organizational, or alternative interventions. The mean length of the interventions was 7.4 weeks. The populations included were working populations not diagnosed with a major psychiatric disorder or a stress-related somatic disorder. CBI was the intervention that produced the largest effect on psychological outcome variables, such as stress, anxiety and mental health. No intervention had an effect on absenteeism (29).
In an RCT from Denmark, 163 patients referred to the regional department of occupational medicine were randomized into 3 groups: (i) an intervention group receiving individual cognitive behavioural therapy (CBT) and an offer of a minor workplace intervention; (ii) a control group receiving a clinical examination; or (iii) a control group receiving no treatment at the department. The patients had a diagnosis of adjustment disorder, reaction to severe stress or mild depressive episode, and were on sick leave due to work-related stress complaints. In all groups psychological complaints improved, but there were no treatment effects on the outcomes perceived stress, general mental health, sleep quality and cognitive failures. At follow-up at 16 weeks there was no significant difference in RTW, but at 44 weeks the intervention group had significantly faster lasting RTW compared with the control group receiving clinical examination (31, 32).
Even though traditional CBT and other forms of psychotherapy can be effective on symptom reduction in stress-related conditions they do not seem to influence RTW or sickness absence (33, 34). A Cochrane review from 2012 evaluated interventions facilitating RTW in patients with adjustment disorders (33). Patients with SED may be sorted under the diagnosis adjustment disorder, which makes this review interesting. Interventions were RCT including pharmacological, psychological, such as CBT and problem-solving therapy (PST), relaxation, physical and employee assistance or combinations. The interventions were effective on symptom reduction, but no intervention achieved a statistically significant reduced time to full-time RTW. The only treatment that significantly shortened time to partial RTW at 1 year follow-up was PST, according to a study of patients from primary healthcare with emotional symptoms, not necessarily reflecting SED (35).
Few studies report long-term follow-up. In a study by Stenlund et al. (55) the long-term effects of 2 different rehabilitation programmes were evaluated in patients with burnout (n = 107). The group receiving a cognitively oriented behavioural rehabilitation in combination with qigong showed positive effects 3 years after the end of intervention compared with controls receiving qigong alone. Patients reported significantly reduced symptoms of burnout, larger recovery and used significantly more tools learned from the intervention. This may indicate that, for patients with SED, establi
shing new behaviours may take time.
A more recently published systematic review from 2018 investigated the effect of psychological interventions in individuals on sick leave due to common mental disorders. The effect size was small, but psychological interventions were found to be more effective than treatment as usual (TAU) for reducing sick leave and symptoms. There was no significant difference between work-focused interventions, PST or CBT (36).
In summary, psychological interventions, CBI and MMI seem to reduce symptoms in individuals on sick leave due to common mental disorders. There seem to be small effect size for CBI and PST on RTW. The interpretation of MMI studies is complicated by the fact that MMI is not a uniform concept. Different clinics include different treatment modalities and furthermore, the selection of treatment modalities used for an individual patient is often based on local traditions and patients’ preferences.
In order to recover from SED and to prevent relapse many patients use different stress-reducing techniques. The most commonly used stress-reducing techniques are discussed below.
Physical activity. Physical exercise can be seen as a buffer against stress through its physiological impact. In healthy people there seems to be almost a dose response effect between leisure-time physical activity and psychosocial well-being, including stress-level and life dissatisfaction (37). Physical activity also appears to lower the risk of burnout (38) and improve cognitive function (39).
Eskilsson et al. (40) published, in 2017, an RCT exploring the effect of aerobic training in patients with SED. Patients participating in a 24-week multimodal rehabilitation (MMR) programme including group-based CBT, vocational measures and individual physical activity on prescription, were randomized to either a 12-week aerobic training intervention (n = 24) or no additional training (n = 32). Primary outcome was cognitive function. The patients in the aerobic training group (51% completed intervention) significantly improved their episodic memory performance after the aerobic training intervention compared with the control group (78% completed intervention). However, there were no significant differences in the cognitive functions executive function, working memory, perceptual speed or reasoning ability and no significant differences on self-rated symptoms of burnout, depression and anxiety (40). This finding in patients with SED is opposite to the general positive effect of physical activity on reducing depressive symptoms and anxiety that has been documented in several meta-analyses (41–43). In a study by Lindegard et al. (44), patients with SED were recommended physical activity as a complement to MMR. Both compliers and non-compliers improved regarding burnout, depression and anxiety, but there was no difference between the groups until at the 18 months’ follow-up when compliers reported significantly lower levels of depression and burnout. No significant differences were found between the groups concerning anxiety (44).
In summary, several meta-analyses demonstrate that physical activity generally reduces depressive symptoms and anxiety. CBT seems to reduce symptoms until the end of the rehabilitation, but regular aerobic training may be important to reduce symptoms in the long-term. Aerobic training at a moderate-vigorous intensity may be important to facilitate cognitive function.
Mindfulness and meditation. Mindfulness is a meditation technique based on being aware of what is happening right now, without valuing or judging (45). It is a popular technique when trying to achieve stress relief.
Mindfulness seems to be positively associated with psychological health, subjective well-being and reduced psychological symptoms (46). According to a review by Creswell (47) mindfulness interventions improve attention-related cognitive outcomes, such as sustained attention and working memory performance, among healthy young adults. Combining mindfulness meditation, body awareness and yoga seems to facilitate relaxation of the body and calming of the mind, and thereby reduce stress and anxiety (48).
A systematic review and meta-analysis from 2014 evaluated the effects of meditation in RCTs. The participants were patients with a clinical psychiatric or physical condition, but also stressed populations without a medical or psychiatric diagnosis. The review concluded that mindfulness meditation programmes have a moderate evidence of decreased anxiety and depression and low evidence of decreased stress and increased mental health-quality of life. Compared with other treatments, such as drugs, physical exercise and behavioural therapies, there was no evidence that mindfulness meditation programmes were better (49).
An RCT from 2013 evaluated the efficacy of a multidisciplinary intervention in patients on full- or part-time sick leave because of significant symptoms of work-related stress for months. The intervention included workplace-focused psychotherapy, a workplace dialogue if the patient agreed and a mindfulness-based stress-reduction (MBSR) course (2 h a week over 8 weeks). The intervention group (n = 69) was compared with 2 control groups, TAU including individual sessions with a psychologist (n = 71) and a waitlist control group (n = 58). Significantly more patients in the intervention group (67%) returned to work compared with patients in the control groups (36% and 26%) after the treatment. Both the intervention group and the controls that received TAU reduced their symptoms significantly compared with the waitlist control group (50).
In summary, mindfulness interventions can improve attention-related cognitive outcomes among healthy young adults, and reduce symptoms of anxiety, depression and stress in a diverse population. According to one RCT mindfulness in combination with workplace interventions could improve RTW in patients with work-related stress compared with TAU. However, the effect of mindfulness alone on RTW is unknown.
Yoga. There are many different schools of yoga, but the key elements for all of them are meditation, breathing exercises and postures. A systematic review summarized 17 articles of mindfulness stress- reduction, yoga combined with mindfulness meditation, from 2009 until 2014 in healthy people, and found that most of the articles showed positive changes in outcomes related to anxiety and/or stress (51).
However, yoga is not only practiced in wellness care, but is also used as therapy in healthcare (52). We found one RCT with an intervention of yoga in patients with stress-related symptoms. Patients in primary healthcare (n = 37) with stress-related diagnosis and self-reported symptoms of stress were treated with standard treatment comprised of individual physical activity, pharmacological treatment, if needed, and individual consultation with a psychologist, physiotherapist, nurse or a counsellor. The patients were randomized to yoga twice a week during 12 weeks, or no yoga. Stress was measured by the Perceived Stress Scale (PSS) and symptoms of anxiety and depression by Hospital Anxiety and Depression Scale (HADS), before and after 12 weeks. The results showed a significant decrease in levels of stress and anxiety (53). The level of depressive symptoms did not decrease.
In summary, the only RCT found on yoga was an intervention for patients with stress-related symptoms, and it showed a significant decrease in levels of stress and anxiety.
Qigong. Qigong is a mind-body exercise that can be practiced at any time and in any place, which may improve physical health and decrease anxiety and perceived stress in healthy adults (54). We found 2 RCTs that evaluate qigong in patients with SED. In one study qigong was performed twice a week during 12 weeks in combination with TAU (n = 82). The control group received TAU. The outcome was psychological variables and physical measurements. Both groups improved significantly, but there was no difference between the groups (55). In the other RCT, patients with burnout were randomized to qigong only or in combination with cognitively oriented behavioural rehabilitation (CBR) (n = 136). Both groups significantly improved in terms of psychological variables and sick leave rates at the 12-month follow-up. There was no difference between the groups (56). At a 3-year follow-up there was still no difference between the groups in terms of rates of sick leave; however, the patients who undertook the CBR seemed to have implemented cognitive tools learned from the CBR and also reported lower levels of burnout (57).
In summary, research does not support that qigong improve psychological variables and rates of sick leave compared with TAU.
Garden/nature. Forest environments seem to reduce stress and can be viewed as therapeutic landscapes in healthy people (58, 59). A review by Keniger et al. summarizes that there is evidence that natural settings have many beneficial effects, including physical health, psychological well-being and cognitive benefits, at least in healthy people (60).
A Swedish study examined in an RCT the qualitative experiences of a forest-based rehabilitation programme in patients (n = 19) on long-term sick leave because of SED. The intervention was offered during 3 months before a cognitively oriented behavioural rehabilitation. Mental peace and conditions for starting the recovery process were the main positive effects reported. The effect was transient and, according to the authors, visiting a forest is a complementary treatment and should probably be combined with CBT to improve recovery by increasing reflection and facilitating the coping process (61). When a forest rehabilitation group (n = 35) was compared with a waiting list group (n = 43) in an RCT, the recovery from SED and psychological measures did not differ between the groups, either after the 3-month forest rehabilitation or after the subsequent 1-year of MMR including CBI for all participants in both groups (62).
A retrospective cohort study of the effect of a nature-assisted rehabilitation programme in a sick-listed group of patients with reactions to severe stress and/or mild to moderate depression found reduced healthcare consumption, but no effect on RTW compared with a matched reference group from the general population (63). In a longitudinal study from Pálsdóttir et al. (64) with a mixed-method approach, symptoms of severe stress and RTW were examined in 21 patients with stress-related mental illness after a 12-week nature-based rehabilitation programme. RTW was measured after 1 year and symptoms of stress after the intervention. The results showed significant changes in symptoms of stress and self-reported RTW (64). However, since the study did not include a control group, it is unclear whether the results were due to time or to the intervention.
In summary, in the few studies retrieved, nature-based rehabilitation may reduce symptoms of stress, but there is only self-reported or no evidence for reduced RTW.
One RCT on SED and cognitive training was found. Patients with SED (n = 27) treated in an MMR programme with additional process-based cognitive training were compared with patients treated with MMR without additional process-based cognitive training. The outcome was an extensive cognitive test battery. The patients in the group with additional process-based cognitive training reported significantly improved cognitive function and lower levels of burnout (65).
In summary, one RCT supports that cognitive training improves cognitive function and decreases symptoms of burnout in patients with SED.
Patients with SED experience mental and physical exhaustion. One reason for these symptoms might be the sleep disruptions that many patients with chronic stress-induced exhaustion experience. Sleep disruptions predict SED, contribute to the onset of SED and may maintain the state (9, 66). Stress might also contribute to cognitive dysfunction by affecting sleep-related neuronal plasticity processes (67). A systematic review from Kärkkäinen et al. (68) exploring factors associated with RTW in patients with burnout found a positive association between unimpaired sleep and RTW.
Typical sleep disruptions that patients with SED experience are arousals, sleep fragmentation, more wake time and lower sleep efficiency (69). In a study investigating the role of sleep physiology, patients (n = 23) with a burnout-related diagnosis and on more than 3 months’ sick leave were subjected to polysomnographic recordings at baseline and after 6−12 months of MMR. Patients improved significantly, with fewer arousals, less sleep fragmentation, less sleep latency and increased sleep efficiency; however, they never reached the levels of healthy controls (n = 16). The best predictor of RTW was recovery from fatigue, and the degree of fatigue was related to a reduction in the number of arousals per hour measured by polysomnography (11). This is in line with a study from Sonnenschein et al. (70), showing that quality of sleep plays an important role both in symptom improvement and in RTW among employees on extended sick leave due to clinical burnout.
A review summarizing meta-analytic and double-blind RCTs on treatments for insomnia found that behavioural interventions are as effective as medication in short-term follow-up studies, but more effective in long-term follow-up studies (71). Other ways to decrease symptoms of insomnia seem to be reducing working time. One study among full-time working employees in the public sector, comparing a 25% reduction in work together with retained salary with controls, showed increased quality of sleep as well as less sleepiness and perceived stress (72). Another study found improved sleep quality with 6-h working days compared with 8-h working days (73).
In summary, quality of sleep plays an important role both in symptom improvement and RTW among persons with SED. In general, behavioural interventions for insomnia are more effective than medication for long-term effect. There is a lack of evidence regarding interventions for improving quality of sleep in patients with SED.
Patients with SED often have symptoms of depression and anxiety at the start of rehabilitation (26). Depressive symptoms may be a reaction to decreased function and exhaustion, but exhaustion might also cause a transient depressive state (74). A study from a stress clinic in Sweden showed that one-third of patients with SED scored high symptoms for depression, and two-thirds scored high symptoms for anxiety when referred to the clinic. After 3 months of rehabilitation there was a significant decrease in patients scoring high symptoms for both depression and anxiety, although high scores for burnout were still present. Antidepressant medication did not predict the course of burnout symptoms but, according to clinical observation, patients on antidepressant medication reported fewer symptoms of depression and anxiety (26).
In summary, there is an absence of evidence regarding the effects of pharmacological treatment in patients with SED.
Workplace interventions (WI) aim to reduce barriers to RTW and to prevent disability. WI focus on RTW instead of symptom reduction. The interventions are closely linked to the workplace and might include work adaptations or involvement of stakeholders at work (75).
Focus on RTW early in the rehabilitation process seems to speed up RTW. In a study with quasi-experimental design by Lagerveld et al. (76) the effectiveness of CBT and work-focused CBT that integrated work aspects early into the treatment, was compared. Patients (n = 168) were employees on sick leave due to common mental disorders, including adjustment disorder, and 12-month follow-up 12 data was collected. Both partial and full RTW occurred significantly earlier in the group that received work-focused CBT (12 days earlier and 65 days earlier), without an increase in psychological complaints (76). According to a review by Vargas-Prada et al. there is limited evidence for very early (delivered < 15 days of sickness absence) workplace interventions compared with usual care in patients with mental health problems (77).
Karlson et al. (78) explored the effect of a workplace-oriented intervention for patients on long-term sick leave due to SED (n = 74). The controls were matched patients who were not interested in participating in the intervention (n = 74), which probably introduced a selection bias in the study. The core intervention was a convergence dialogue meeting between the patient and the supervisor at the workplace, with the aim of finding solutions to facilitate RTW. At follow-up after 1.5 years RTW was increased in the intervention group compared with controls (78). However, in a follow-up after 2.5 years the difference in RTW remained only in subjects younger than 46 years (79). In an RCT by Willert et al. (80) patients with stress-related disease (n = 102) were randomized to a stress management intervention or waitlist. The goal of the intervention was to cope with stressful situations at work and, despite their difficulties, to be active at work. At follow-up after 16 weeks, patients in the intervention group self-reported lower absenteeism compared with controls. However, no significant evidence was found for RTW (80). In a controlled designed study by Lander et al. (81) stress-management intervention did not improve RTW in patients sick-listed for emotional distress. Nor did a Minimal Intervention for Stress-related mental disorders with Sick leave (MISS) improve RTW in a cluster randomized controlled educational trial in patients on less than 3 months of sick leave due to stress-related mental disorder. Primary healthcare practitioners were randomized to short training sessions, including, for instance, how to encourage patients’ recovery and active RTW (82).
An RCT by Finnes et al. (83) compared acceptance and commitment therapy (ACT) and a workplace dialogue intervention (WDI), standalone and in combination and TAU among persons on sick leave due to depression, anxiety and stress-related disorders. In all treatment groups sickness absence decreased and work ability increased after 9 months, there was no difference between the interventions groups. However, when diagnostic group was included as a moderator, participants with stress-related disorders had fewer sick leave days in the WDI group compared with TAU. In addition, self-reported symptoms of depression, anxiety and exhaustion decreased, but with no significant difference between the groups (83). In another RCT by Blonk et al. (84) the effect of 2 different CBT-based interventions and a control group were compared in patients on sick leave due to work-related psychological complaints (i.e. adjustment disorders, such as burnout and job stress). Significant effects were found in the group of patients that received a combined intervention including workplace and individual-focused techniques delivered by a labour expert. The patients in the combined intervention group returned to full work almost 7 months before the other groups. There was no difference in RTW between the CBT group and the control group. In addition, partial RTW was found significant in favour of the combined intervention. However, the dropout level was high (84 out of 122 subjects fulfilled the study) (84). Interestingly, like the RCT by Finnes et al., psychological complaints generally diminished over time, with no differences between the groups (83, 84). Increased RTW, but no significant difference in perceived stress, was also found in a comparative study by Eklund et al. (85) in women rehabilitated in a 16-week group-based Redesigning Daily Occupations programme (ReDO) (n = 42) compared with women who received TAU. However, in an RCT by Salomonsson et al. (86), patients with common metal disorders (n = 211) were randomized into 3 groups; CBT (n = 64), an RTW intervention (n = 67) or a combination (n = 80). There was no significant difference between the groups regarding sick leave and all groups effectively reduced symptoms, although CBI a little faster than the others, at least until the 1-year follow-up (86).
Instead of focusing on symptom recovery, the main aim of WI is to prevent disability and promote management to enable RTW. According to a Cochrane review (87) of 14 RCTs there is moderate-quality evidence that WI help workers with musculoskeletal disorders to RTW. However, there was only low-quality evidence on the effectiveness for WI in patients with mental health problems, including stress-related disorders (87). In a systematic review and meta-analysis, from 2016, of interventions for enhancing RTW in individuals with common mental disorders, the available interventions did not improve the percentage of employees who returned to work; however, they seemed to reduce the number of days of sick leave (88). A review from Kärkkäinen et al. (68) exploring work-related factors associated with RTW found that enhanced communication had a positive association and low control at work a negative association with RTW. Another recent systematic review and meta-analysis from Perski et al. (89) found that interventions focusing on treatment and facilitation of RTW, including advice from labour experts and enablement of a workplace dialogue, may be effective in facilitating RTW. However, no significant effect was found on full RTW or psychological symptoms (89).
The result of an RCT for sick-listed employees with distress, by van Oostrom et al., pinpointed that the intention to RTW at baseline is important for the result. The WI included a stepwise process involving the patient and their supervisor, aiming to reduce obstacles for RTW, significantly reduced time until lasting RTW only for employees who at baseline intended to RTW, despite symptoms (90).
In summary, WI, either by work-focused CBT or workplace dialogue intervention, seem to improve RTW.
Patients with SED have experienced high levels of stress without sufficient recovery for a long time, in SED by definition for more than 6 months. Patients are initially often markedly mentally and physically exhausted and in need of full- or part-time sick leave. Several studies show decreasing symptoms over time in both intervention and control groups, and early rehabilitation does not necessarily shorten the period of sick leave (91). However, although patients with SED initially need to rest, long-term sickness in itself could be a risk factor for reduced probability of RTW (68). This, in turn, means economic and social deprivation (92). Graded RTW seems to be effective for successful work participation in patients with chronic mental disorders (93). In order to avoid relapses the workplace often needs to take necessary measures, and good cooperation with the employer might facilitate this.
Patients with SED referred to a stress clinic still describe symptoms of exhaustion after 18 months (26), indicating that RTW often has to start, even though the patient still experiences some symptoms. In a study by Glise et al. (26) the only predictor of recovery from symptoms of burnout after 18 months was the duration of symptoms before the patient sought healthcare. This underlines the importance of finding these patients at an early stage, but also of not waiting for an asymptomatic state before starting rehabilitation and RTW. Long-term sick leave before rehabilitation is significantly related to future sick leave for patients with burnout (34). Rehabilitation of severe SED takes time, and it is important not only to provide good healing conditions, but also to work with prevention, in order to minimize the risk of relapse. No articles were found exploring interventions for prevention of relapse.
There are few high-quality studies examining the effects of interventions on SED. Among patients with stress-related conditions and adjustment disorder, CBI and MMI appear to reduce symptoms, at least until the end of the intervention. For SED, only WI, either with work-focused CBT or workplace dialogue intervention, seem to improve RTW. CBI and nature-based rehabilitation do not appear to improve RTW. Sleep appears to be important for both symptom improvement and RTW, and interventions for improving sleep might therefore be important. Cognitive impairment is a main complaint among patients with SED, and probably contributes to the long-term sick leave. For improvement of cognitive function aerobic and cognitive training may have some effect. Research on interventions for rehabilitation of SED show only marginal effects. Thus, it is important to prevent the onset of SED.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize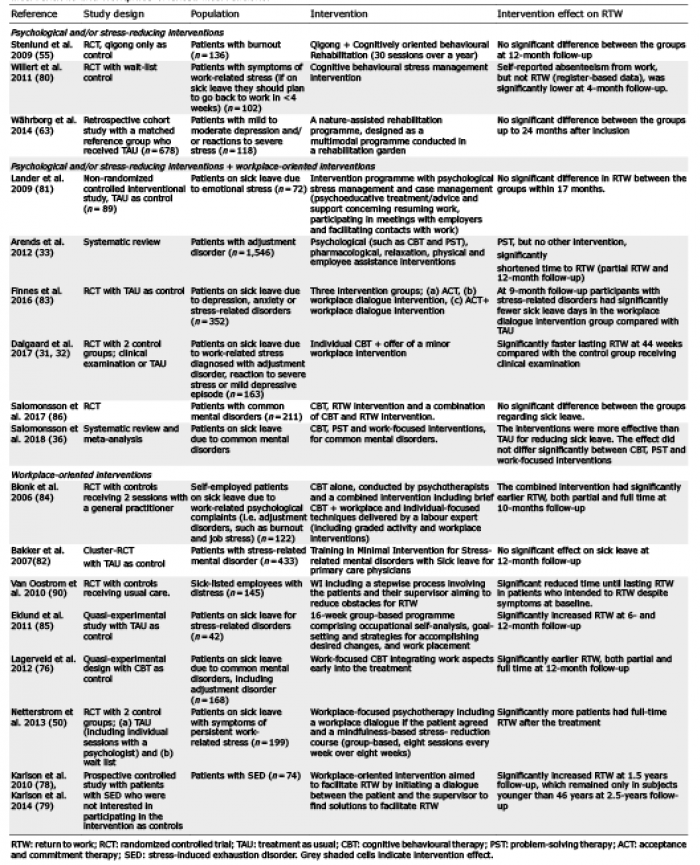 Click to show fullsize
Click to show fullsize