
From the 1College of Nursing and Health Sciences, Flinders University, South Australia, 2Physiotherapy, Faculty of Medicine and Health Sciences, Stellenbosch University and 3Australian Health Services Alliance, Melbourne, Victoria, Australia
Objectives: To systematically identify literature reporting on assessment instruments relevant for incipient hospital-acquired deconditioning during acute hospital admissions; evaluate their psychometric properties; and identify individual assessment items to form the basis of a comprehensive acute hospital test battery for hospital-acquired deconditioning.
Design and data sources: Systematic evidence scan of MEDLINE, CINAHL, PubMed and Google Scholar from database inception to January 2018.
Study selection: Papers reporting psychometric properties of assessment instruments to detect change in body function and structure, relevant to hospital-acquired deconditioning were selected. Included instruments should assess one or more elements of hospital-acquired deconditioning, reflect the short time-frame constraints of acute hospital admissions, and be able to be applied by any healthcare provider.
Quality evaluation: Evidence of psychometric properties and utility were assessed using a validated instrument.
Data extraction: Hospital-acquired deconditioning assessment items.
Results: Eight potentially-relevant instruments were identified, with moderate-to-good validity and utility, but limited evidence of reliability. These instruments reported a total of 53 hospital-acquired deconditioning assessment items. Seventeen items with measurement periods greater than 3 days were excluded. The remaining items measured anthropometrics, gait, balance, mobility, activities of daily living, and skin integrity.
Conclusion: These assessment items provide the basis of a multifaceted evidence-based test battery to comprehensively and repeatedly assess acute hospital inpatient function for incipient hospital-acquired deconditioning.
Key words: hospital-acquired deconditioning; HAD; assessment; inter-professional practice; quality care; discharge planning; functional decline; frailty; systematic evidence scan; psychometric properties; utility; older people; acute hospital admission.
Accepted Feb 26, 2019; Epub ahead of print Mar 15, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Sue Gordon, Chair of Restorative Care in Ageing, A partnership position funded by ACH group and Flinders University, College of Nursing & Health Sciences, Clinical Teaching and Education Centre at ViTA, 17 Rockville Avenue, Daw Park, South Australia 5041, Australia. E-mail: sue.gordon@flinders.edu.au
Hospital-acquired deconditioning can occur insidiously and rapidly as a result of enforced bed rest, immobilization or sedentary behaviours. While hospital-acquired deconditioning can occur in people of any age, it is particularly problematic in elderly people, as it can lead to irreversible functional decline. Hospital-acquired deconditioning is preventable with proactive, comprehensive regular assessment to detect changes in the performance of body systems. The time-period of assessment must be short, so that repeated assessments can be made during an acute hospital admission. At present there is no comprehensive, time-sensitive assessment instrument for hospital-acquired deconditioning. Based on a systematic scan of the literature, this paper proposes a core set of items that could be developed into a comprehensive, standardized assessment instrument for regular application by any healthcare provider during an acute inpatient stay, to identify incipient hospital-acquired deconditioning. The assessment items measured anthropometrics, gait, balance, mobility, activities of daily living, and skin integrity.
Deconditioning is “a complex process of physiological change following a period of inactivity, bedrest or sedentary lifestyle” (1, p. 16). Older people are particularly at risk (1–5), as deconditioning in this age group can quickly progress to irreversible functional deterioration and frailty (3, 4, 6, 7), decreased life expectancy and quality of life.
Hospital-acquired deconditioning (HAD) can occur within days for adults of any age, during acute hospital admissions involving enforced bed rest, immobilization and/or sedentary behaviours (2–4, 7). There is no standard definition of HAD, and no agreement on common HAD elements, or assessment practices (1–4, 8–10). HAD changes can be insidious, and if undetected, can delay safe discharge from hospital and/or require additional recuperative care (5–7, 9). It is counterintuitive that HAD should occur in healthcare settings, where it could be reasonably expected that health should improve, not decline (2, 4, 12). How-ever, HAD is a reality in many countries (2, 4, 12). It is coded as M62.81 (generalized muscle weakness) in the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), a system used by healthcare providers to code diagnoses, symptoms and procedures related to hospital care (8).
Most HAD research has focused on older people (1–4). Falvey et al. described HAD as “declines in muscle strength, muscle mass, cognitive function, muscle protein synthesis and physical function” (2, p. 1307), while van Vliet & Deeg describe it in terms of loss of mobility (stairs, footpaths) and inability to undertake activities of daily living (such as sit-to-stand, moving around, and cutting toenails) (4). Creditor described 8 hazards of hospitalization (including bed rest or enforced immobilization) as: decline in muscle strength and aerobic capacity; vasomotor instability; reduced bone density; reduced pulmonary ventilation; altered sensory “continence”, appetite and thirst; and urinary incontinence (12). Compared with other authors in the field, Creditor reports the broadest range of HAD attributes, and these were used to benchmark the assessment items identified in this evidence scan (12).
HAD elements overlap those described for frailty. Like HAD, frailty is also variably described in the literature by characteristics such as decreased muscle strength; fatigue; compromised ambulation, continence, nutrition, sleep patterns and/or energy levels; heightened anxiety and/or depression; unexplained persistent pain; and/or decreased confidence in safely undertaking usual daily activities (1–7, 12). The main difference between HAD and frailty appears to be the time-frame within which change is detected. HAD can manifest within hours of hospitalization requiring bed rest or immobility (1, 2, 4, 6), whilst frailty is generally more insidious, taking longer for subtle age- or disease-related changes to functioning to manifest (1, 5). Thus, the challenge of identifying HAD is ensuring the repeated, judicious application of measures that can efficiently demonstrate change within days of hospitalization.
The term “body systems performance” is used in this paper as an overarching term for a range of factors addressed in the International Classification of Functioning, Disability and Health (ICF), including body functions and structures (such as weight, nutritional status, cardiopulmonary condition, muscle strength, skin integrity) and functional capacities (such as balance, transfers, walking ability, self-care) (13).
There are increasing pressures on acute hospital beds worldwide, particularly given increases in the prevalence of chronic disease and the proportion of people living for longer (2, 8–10). Safe, efficient and effective discharge from hospital to home makes economic and social sense (1, 2, 10, 12, 14, 15). Preventing HAD is essential for safe, efficient discharge, and to prevent readmission (1, 2, 6, 7, 8, 14). Therefore, being alert to, and assessing for, incipient HAD should be within the remit of any health professional (14, 16). However, there is no comprehensive agreed assessment for HAD that can be applied repeatedly during an acute hospital admission (1–3, 5, 7, 8, 11–15). To be relevant to an acute hospital admission, HAD assessment items need to be measured at point-in-time (P-i-T) (or over very short time-frames), so that incipient HAD can be identified within days of admission.
To date, inpatient assessments of body system performance are often inconsistently conducted by different healthcare professionals, using different assessment instruments, which assess different aspects of body system performance over different time-periods (2, 4, 12, 14–16). Moreover, findings are variably recorded and shared, which constrains proactivity in preventing HAD (11, 14–16). This largely reflects the primary focus of acute hospitals, which is to resolve the reason(s) for admission, rather than to prevent unsuspected and adjunctive issues, such as HAD (14–16). As a result, HAD may not be recognized until it has become a risk to successful discharge. Hospital quality standards and bed flow would be significantly enhanced if regular application of core standard assessment items for HAD occurred throughout the acute hospital stay (1–3, 8–10, 14, 15). This paper describes research to fill a current gap in clinical assessment practices for HAD in acute hospital settings.
To systematically identify literature reporting on assessment instruments relevant for incipient HAD during acute hospital admissions; evaluate their psychometric properties; and identify individual assessment items to form the basis of a comprehensive, acute hospital test battery for HAD.
There is no standard, comprehensive instrument currently available to assess acute hospital inpatients for all elements of incipient HAD.
Identification of items from one or more psychometrically-sound assessment instruments, to form the basis for comprehensive testing of body systems performance to detect incipient HAD during an acute hospital admission.
Papers that described psychometric properties of assessment instruments for any element of HAD were systematically identified. The psychometric properties and clinical utility of these instruments were then critiqued using a validated checklist (17); and assessment items relevant to a comprehensive test battery for incipient HAD identified. The items must be able to be repeatedly and efficiently applied and recorded by any healthcare provider in acute hospital settings.
A systematic evidence scan was undertaken, guided by relevant methods and reporting frameworks (16, 18, 19).
Whilst the literature search targeted assessment instruments designed for, or tested on, older people (considered to be most at risk of HAD), instruments relevant to any acute hospital inpatient 18 years or older were also considered (2, 4, 12, 15). Literature was included if:
A Population (P) – Intervention (I) – Time (T) framework was applied: P = any acute hospital inpatient but in particular, older people; I = assessment instruments relevant to detecting any element of incipient HAD; and T = time-period of acute hospital admissions (i.e. instruments with items appropriate for repeated short-term application). The expanded search terms and syntax for each database are reported in Table SI1. Library databases (MEDLINE, CINAHL, PubMed, PsychInfo and Google Scholar) were searched from database inception until January 2018.
Literature was excluded if it:
reported on condition- or disease-specific assessments of body systems performance (e.g. cancer, trauma, stroke and other neurological conditions, chronic respiratory conditions or cardiac conditions). These conditions have predictable management pathways, specific diagnostic codes, condition-specific assessment items and time-frames of measurement, and predictable functional changes;
Potentially-relevant articles were considered collaboratively by author-pairs (using title and abstract). They then collaboratively assessed full texts of potentially-relevant papers against inclusion and exclusion criteria. If more than one paper described psychometric testing of an assessment instrument, the earliest paper was included, and the number of subsequent psychometric testing papers was recorded. Disagreements were arbitrated by a third author.
Study design was assigned using the Australian National Health and Medical Research Council hierarchy (22).
Items with measurement time-periods longer than 2–3 days were excluded, because they were not feasible for repeated administration during an acute inpatient stay. To evaluate psychometric properties and clinical utility, the validated iCAHE Ready Reckoner was applied by author-pairs (17). The iCAHE Ready Reckoner seeks evidence from the developmental literature that an assessment instrument demonstrates quality elements, but does not record the statistics:
The iCAHE Ready Reckoner does not apply a specific threshold to detect instrument quality. Higher total scores indicate better quality instruments.
All items in the included assessment instruments were extracted, the measurement purpose was identified, items were cross-matched with the Creditor HAD elements (12) as well as with items with similar intent in the other included instruments, and time-frames of reporting were described. Items that were readily applicable by any healthcare provider, and which could form the basis of a comprehensive assessment for HAD were identified by discussion between the authors.
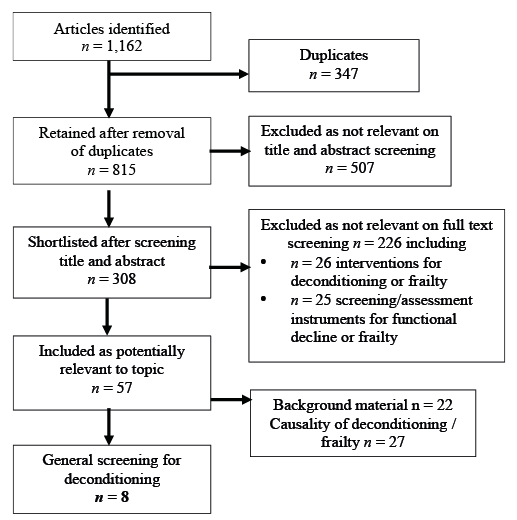
Of 1,162 potentially-relevant papers, 8 were retained, each reporting on the development of a relevant HAD-assessment instrument (25–32). The inclusion flowchart is shown in Fig. 1.
Fig. 1. Literature inclusion flow chart.
As hypothesized, no single instrument reported items that comprehensively assessed all HAD elements (as described by Creditor (12)). The 8 identified instruments assessed different elements of HAD, often using different methods for the same element. The included instruments are described below.
Timed Up and Go Test (TUG) (25). This point-in-time assessment reports the time (in s) taken to complete an integrated task set (rising from a chair, walking 3 m, turning, walking back, and sitting down again). The TUG has been used to assess performance in older people for 30+ years. It offers a simple way of assessing complex constructs (transferring between positions, static and dynamic balance, gait, falls likelihood, and ability to safely complete turning movements).
Physical Performance Test (PPT) (26). This point-in-time assessment includes 8 activities of daily living (writing a sentence; simulated eating; turning 360°; putting on and removing a jacket; lifting a book and putting it on a shelf; picking up a coin from the floor; walking 50 feet; and climbing stairs (optional)). The PPT has been widely used in aged care settings.
Dartmouth COOP (Cooperative) Function Charts (27). This instrument is over 30 years old. It is published in association with the World Organization of Colleges, Academies and Academic Associations of General Practitioners/Family Physicians (WONCA)). It measures 6 aspects of function over the previous 4 weeks (physical fitness, feelings, daily activities, social activities, change in health, and overall health). A pain measure is optional, and a sleep measure is being developed. Each chart uses a simple drawing and 5-point ordinal response scales (“no limitation at all” to “severely limited”). The instrument has been translated into 17 languages, and is widely used in research and clinical practice. It requires registration prior to use.
Nutrition Screening Initiative Checklist (NSIC) (28). This consensus-based instrument assesses nutritional risk in older people, using a “recent” reflection period (undefined). It can be delivered via telephone interview, or face-to-face. Higher scores identify increased nutritional risk. It measures dietary intake and recent dietary changes, dental and oral health, swallowing, social isolation, expenditure on food, polypharmacy, recent weight loss or gain, and compromised functional capacity in shopping or cooking.
Short Physical Performance Battery (SPPB) (29). This point-in-time instrument captures ability to overcome daily movement challenges including standing and sitting 5 times from a chair, balance and walking a set distance.
Mini Nutritional Assessment (MNA) (30). This multidimensional instrument evaluates nutritional state and risk in elderly people. It includes point-in-time anthropometric measures (weight, height, arm and calf circumferences, weight loss), and current medications. It also includes questions with a longer (3-month) reflective period on lifestyle, mobility, diet and subjective self-assessed health and nutritional state. The point-in-time questions are relevant to repeated delivery during an acute hospital stay. Respondents are classified on a total score as “normal and well nourished”, or “at risk for malnutrition”, or “malnourished”.
De Morton Mobility Index (DEMMI) (31). This is a point-in-time measure of mobility using increasingly difficult physical challenges. DEMMI has been tested in different clinical settings and older populations. It has 15 items measuring mobility in bed, in a chair, during static and dynamic balance with no gait aid, and walking. Items are scored on a 3-point scale (“unable”, “able” and “independent”). Scores are scaled to 100, with higher scores indicating better mobility levels.
Activity Measure for Post-Acute Care (AM-PAC) “6 Clicks” instrument (32). This was developed specifically for hospitalized elderly people. All questions are measured point-in-time. Three questions are about perceived difficulty “turning in bed”, “sitting down and standing up from a chair”, and “moving from lying to sitting on the side of the bed”. The questions ask about help required from others to “move from bed to chair”, “walk in the hospital room” and “climb 3–5 steps with a railing”. Four level responses (scored 1–4) are applied to each item (“unable”, “a lot”, “a little” and “none”), with higher scores indicating fewer problems.
All included papers described diagnostic studies (National Health and Medical Reserach Council (NHMRC) Level II) (22).
Measurement period. The COOP/WONCA instrument requires a 4-week reflection period, and thus was excluded from further consideration (27). The MNA items with 3-month reflection periods (30) were also excluded. In addition, the reflective interview questions, and some objective measures in the NSIC (28) and SPPB (29) were excluded because they, like the COOP/WONCA and reflective MNA questions, were more appropriate for comprehensive screening, at hospital admission, of general health status, or current frailty state, rather than detection throughout the hospital stay of altered performance of body systems, which could indicate incipient HAD (1–4). The excluded MNA items comprised usual food intake, recent weight loss and psychological stress or acute disease within the past 3 months, and the excluded NSIC and SPPB items comprised usual dietary habits; usual alcohol intake; tooth or mouth problems; isolation; literacy; polypharmacy; body mass index (BMI); finances; and self-perceived health status. BMI lacks sensitivity to detect meaningful change over short time-periods, such as an acute hospital admission (33, 34).
Psychometric and utility properties. Table I reports the psychometric and utility properties of the included assessment instruments. Despite excluding items from MNA, NSIC and SPPB, the psychometric properties of these instruments were reported, because some items remained relevant to the purpose of this research. All included instruments demonstrated moderate to good evidence of validity and clinical utility, but only 2 scored well for reliability testing (TUG (25), DEMMI (31)). Four of the instruments reported population norms (25, 28–30). Of the possible total score of 19, the highest scoring instrument was TUG (25) (84%), followed by SPPB (26) and DEMMI (31) (79%), then NSIC (28) and PPT (26) (68%), then MNA (30) (63%) and, finally, AM-PAC “6-Clicks” (31) (58%).
Table I. Ready reckoner
Table SII1 reports the 53 items related to any aspect of body systems’ performance that was assessed in at least 1 of the included instruments, compared with the Creditor list (12). This table highlights that no instrument assessed urinary incontinence or osteoporosis. Considering the measurement time-periods, any change in osteoporosis state will take longer to occur than during an acute hospital admission, and therefore it is rejected on time-frame. Urinary incontinence should, however, be considered for inclusion in a composite HAD instrument, as change can occur in this element within days (35).
Compilation of items. Table II reports instruments, item measurement time-frames, the body systems performance measured by each assessment item, and the assessment items. Muscle strength was the most commonly-measured HAD element (5 instruments); followed by mobility, balance, fitness, activities of daily living and walking distance (4 instruments), then gait speed (3 instruments) and appetite (2 instruments). No HAD element was measured in the same way across instruments.
Table III reports a compilation of specific assessment items extracted from included instruments, which relate to the body systems performance measures outlined in Table II. For all but incontinence, the included screening instruments provide at least 1 way of measuring each element (see shading in the table). The HAD assessment items include standing and functional balance, functional mobility (in bed, and ambulatory), anthropometrics, skin integrity, a range of practical activities of daily living across instruments, circumferential limb measurements (arm and/or calf), appetite and incontinence.
Table II. Relevant hospital-acquired deconditioning (HAD) assessment items, and the body systems they address, from included instruments
Table III. Collated assessment measures of items relevant to incipient hospital-acquired deconditioning (HAD)
As hypothesized, this study of the evidence found no single instrument that contained a comprehensive list of assessment items to detect incipient HAD during an acute hospital admission. The 7 relevant assessment instruments provided a variety of ways in which P-i-T, or assessments in the past few days, of the performance of different body systems could be undertaken. Whilst the application of all instruments identified in this review might provide a comprehensive assessment of incipient HAD, this would be inefficient, and unnecessary. Not only would there be significant repetition of measurement, and duplication of effort, but there would be interpretation challenges related to correlating the different assessment approaches taken for the same HAD element in different instruments (see Table SII1). Our research suggests that the current clinical assessment gap could be filled by a new comprehensive assessment instrument, based on the items identified from this search.
Any new assessment instrument for HAD requires psychometric and utility testing. Even though the suggested assessment items come from instruments with moderate-good validity and utility, a new assessment battery needs to re-establish validity (particularly construct and content validity, item redundancy and sensitivity). A scoring rubric is essential so that overall performance can be readily quantified, and expected population norms should also be developed. Any new HAD assessment instrument also requires extensive reliability testing. This was a critical omission in 5 of the included instruments. Information on expected variability in performance of body systems is urgently required over a typical inpatient hospital stay, for different sex-age groups, so that abnormal deterioration of body systems can be readily identified (2, 4, 5, 7).
The development of a new comprehensive HAD assessment instrument could be integrated with quality care and discharge planning standards, and hospital accreditation requirements (2–4, 14). It is counterintuitive, and makes no economic, social or functional sense to allow people to decondition whilst in hospital, and to leave hospital in poorer health than when they were admitted (1, 3–5). Regular application of a composite test battery will identify incipient HAD before it becomes an issue, and promote healthy ageing in, and out of, hospital. It could also underpin integrated inter-professional practice (14, 16). A comprehensive assessment instrument should be able to be delivered by any healthcare provider from any discipline (e.g. doctor, nurse, physiotherapist, occupational therapist, healthcare assistant). Because it uses a standard approach, the findings could then be readily understood and discussed at inter-professional discharge planning meetings for HAD risk identification and mitigation strategies (6, 7, 9, 14).
Not all the Creditor HAD items were addressed in the included assessment instruments (e.g. demineralization (markers for osteoporosis), nutritional status/usual food intake, sensory “continence”, urinary continence and polypharmacy) (12). Whilst items such as balance, function, mobility, skin integrity could readily be assessed and re-assessed over short time-periods, measures such as demineralization, nutrition, appetite, perceived health status, sensory deprivation (hearing, vision, touch, taste, smell, etc.), osteoporosis and polypharmacy are more appropriate to longer-term reflective measurement periods (2, 4, 10). These measures lend themselves to comprehensive assessment on hospital admission, to detect already declining function and frailty (5). Moreover, proxy measures of demineralization could be inferred from anthropometric measures, mobility, balance and muscle strength, and sensory “continence” is integral to successful completion of all physical tests (2, 4, 5). However, urinary (and faecal) continence can change over short time-periods, and thus its assessment should be included in any new HAD instrument (34).
This systematic evidence scan identified that at least 12 tests of performance in different body systems are required for comprehensive assessment for incipient HAD (see Tables II and III). Whilst condition-specific assessments were deliberately excluded in order to find general HAD assessments, the included assessment items could also be applied to people with known
chronic conditions to ensure that they do not decondition
whilst receiving care requiring bed rest.
The comprehensiveness of the search was potentially limited by the lack of agreed characteristics of HAD, against which assessment items from the identified instruments could be aligned. Moreover, the breadth of the evidence scan was potentially limited by inconsistencies in nomenclature describing deconditioning, functional decline and frailty. The search may thus have failed to identify all relevant HAD assessment literature. The focus on general HAD assessment items (non-condition-specific) may have limited identification of relevant items that had been developed for chronic conditions or disease, but were, in fact, transferable to global HAD assessment.
No single assessment instrument currently assesses HAD comprehensively. HAD should largely be identifiable with regular targeted, comprehensive assessment of performance of multiple body systems, in order to detect early changes. This would support preventative interventions during the hospital stay and restorative interventions on discharge.


 Click to show fullsize
Click to show fullsize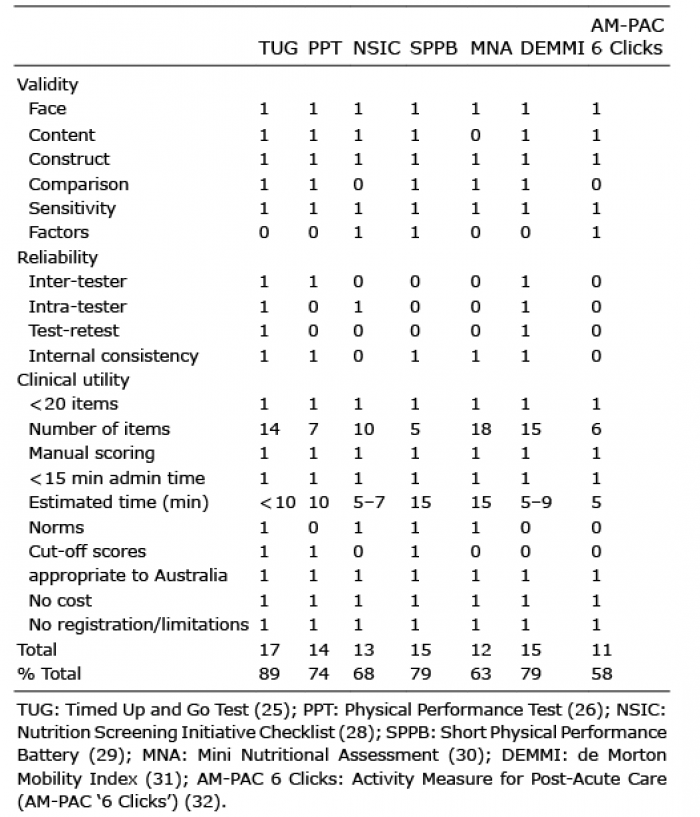 Click to show fullsize
Click to show fullsize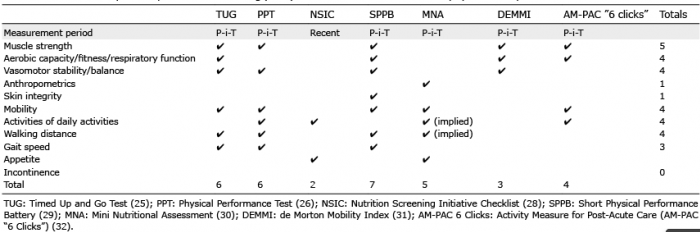 Click to show fullsize
Click to show fullsize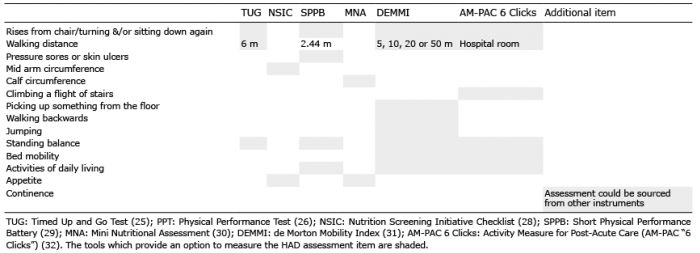 Click to show fullsize
Click to show fullsize