
From the 1Department of Cardiology, Aalborg University Hospital, 2Aalborg AF Study Group, Aalborg University Hospital, 3Department of Physiotherapy and Occupational Therapy, Aalborg University Hospital, 4Public Health and Epidemiology Group, Department of Health, Science and Technology, Aalborg University and 5Unit of Clinical Biostatistics, Aalborg University Hospital, Aalborg, Denmark
Objective: To examine the effect of a rehabilitation programme on quality of life and physical capacity in patients with atrial fibrillation.
Methods: Patients with paroxysmal or persistent atrial fibrillation were randomized to either a 12-week rehabilitation programme with education and physical training (intervention group) or standard care (control group). At baseline, after 3, 6 and 12 months participants completed 5 different quality of life questionnaires (Quality of Life in patients with Atrial Fibrillation (AF-QoL-18), Atrial Fibrillation Effect on QualiTy of Life (AFEQT), Patient Health Questionnaire (PHQ-9), Generalised Anxiety Disorder Assessment (GAD-7) and EuroQol 5D (EQ-5D)), and physical exercise tests. Differences in mean] scores between groups were analysed by repeated measures analysis of variance (ANOVA).
Results: Fifty-eight patients (age range 43–78 years, 31% female) were included. In the intervention group the AF-QoL-18 score increased from baseline (48.4 (standard deviation (SD) 22.8)) to 6 months (68.0 (SD 15.2)) compared with the control group (baseline 51.6 (SD 22.3), 6 months 59.2 (SD 27.3)). After 12 months, there was no difference. Similar patterns were found for the other questionnaires. Maximum exercise capacity improved in the intervention group from baseline (176 W (SD 48)) to 6 months (190 W (SD 55)). There was no change in the control group.
Conclusion: Education and physical training may have a short-term (but no long-term) beneficial effect on quality of life and physical exercise capacity in patients with atrial fibrillation.
Key words: atrial fibrillation; rehabilitation; quality of life; physical exercise; education.
Accepted Mar 22, 2019; Epub ahead of print Apr 1, 2019
J Rehab Med 2019: 51: 442–450
Correspondence address: Albert Marni Joensen, Department of Cardiology, Aalborg University Hospital, Søndre Skovvej 15, DK-9000 Aalborg, Denmark. E-mail: albert.marni.joensen@rn.dk
Atrial fibrillation is the most common cardiac arrhythmia and the number of atrial fibrillation patients is growing worldwide. In addition to an increase in risk of stroke and heart failure patients with atrial fibrillation also experience decrease in fitness and quality of life. In our study 58 atrial fibrillation patients draw lots to participate or not in a rehabilitation program with education and exercise training in addition to usual treatment. We measured fitness by a bicycle test at the beginning of the study and after 3 and 6 months, moreover participants filled out questionnaires on quality of life at the beginning of the study and after 3, 6 and 12 months. We found that our rehabilitation program may have a short term (but no long term) effect on quality of life and fitness in atrial fibrillation patients.
Cardiac rehabilitation takes a cross-functional approach to the aftercare of patients, including individually designed treatment plans, patient information and education plans, physical exercise, dietary guidance, psychosocial support, optimization of medical treatment, risk factor control, and individual maintenance of treatment goals.
There is strong evidence that rehabilitation has a beneficial effect on quality of life (QoL) in patients with coronary heart disease (CHD) (1). However, patients with atrial fibrillation (AF) are seldom and not systematically offered rehabilitation.
Previous studies have demonstrated that patients with AF lack knowledge regarding the natural history of AF, consequences, treatment and how to manage a change in QoL caused by AF (2).
In addition, the relationship between physical exercise and AF has been disputed. Among 64,561 patients, Qureshi et al. found an inverse relationship between cardiorespiratory fitness and incident AF, especially in obese subjects who underwent exercise treadmill testing (3). In 825 obese patients with AF, Pathak et al. demonstrated a lower burden of AF in patients who lost weight and improved their cardiorespiratory fitness (4, 5). Pathak et al. also demonstrated a beneficial effect of aggressive risk factor management on the long-term success of AF ablation (6). Randomized studies on patients with primarily permanent AF have demonstrated beneficial effects of physical exercise on physical capacity, AF symptoms and QoL (7–11).
The prevalence of AF is increasing (12), therefore, it is important to investigate whether a rehabilitation programme can improve QoL and physical exercise capacity in patients with AF and, potentially, prevent readmissions.
The aim of this study was to investigate whether a rehabilitation programme with group education, physical exercise, optimization of medical treatment and monitoring of lifestyle changes can improve QoL and physical exercise capacity in patients with AF.
Clinical randomized controlled trial. ClinicalTrials.gov (record N-20120002).
Patients with paroxysmal or persistent AF admitted to the Department of Cardiology, Aalborg University Hospital between 6 June 2012 and 4 April 2013 were consecutively invited to participate in the study. All patients received treatment according to the current guidelines. Patients who provided informed consent to participate were randomized to either specialized cardiac rehabilitation or standard follow-up. The rehabilitation programme consisted of groups of 10 patients.
At the primary admission, all patients underwent echocardiography and blood samples were taken.
Inclusion criteria. Patients ≥ 18 years of age, hospitalized at the Department of Cardiology, Aalborg University Hospital, with a diagnosis of paroxysmal or persistent AF documented by an electrocardiogram (ECG) or > 30 s of AF recorded by long-term monitoring. All participants received oral and written information prior to providing written informed consent.
Exclusion criteria. atients who qualified for cardiac rehabilitation due to other cardiac conditions (congestive heart failure or CHD) were excluded. If AF was caused by a reversible condition patients were also excluded.
Heart failure (New York Heart Association (NYHA) class III–IV or Left Ventricular Ejection Fraction (LVEF) < 40%) or valvular heart disease and patients admitted for radiofrequency ablation were also excluded. Patients considered too ill, physically or mentally, to participate in rehabilitation by the treating physicians were excluded.
Randomization was electronically, randomizing the participants into 2 groups of 20 participants at a time.
The rehabilitation programme included education, physical exercise, optimization of the medical treatment and discussion of implications on daily life.
The group sessions with a doctor, a nurse, a dietician or a psychologist was scheduled once a week for 1 h for the first 8 weeks. The education included information on pathophysiology, risk factors, treatment, diet and coping mechanisms for living with AF.
The exercise programme was conducted as 1-h sessions twice a week for 12 weeks and supervised by a cardiac rehabilitation physiotherapist. Each training session consisted of at least 30 min of aerobics ≥ 70% of maximum exercise capacity estimated from a maximum cycle ergometer test with ECG monitoring and graded on the Borg scale (score 14–16) and interval training with elements of strengthening exercises (13).
Patients were encouraged to be moderately physically active ≥ 30 min each day and, if they missed a group training session, to perform 30 min of high-intensity activities.
The medical treatment was optimized according to the current guidelines.
At inclusion and after 3, 6 and 12 months, all participants completed the following disease-specific QoL questionnaires: Health-related Quality of Life in patients with Atrial Fibrillation (AF-QoL-18) and Atrial Fibrillation Effect on QualiTy of Life (AFEQT) and the generic QoL questionnaires: Generalised Anxiety Disorder Assessment (GAD-7), Patient Health Questionnaire (PHQ-9) and EuroQol 5D (EQ-5D).
AF-QoL-18 includes 18 questions on 3 domains: psychological, physical and sexual activity. The answer score range from zero (worst) to 100 (best). AFEQT includes 20 questions on treatment, symptoms and daily activity during the last 4 weeks. The score range from 20 (best) to 140 (worst).
GAD-9 assesses anxiety and results range from zero (worst) to 21 (best). PHQ-9 focuses on depression symptoms during the latest 2 weeks ranging from zero (best) to 27 (worst). EQ-5D consists of 5 questions on mobility, self-care, usual activities, pain/discomfort, anxiety/depression and a visual analogue scale (EQVAS) assessing self-estimated health status.
At inclusion and after 3 and 6 months, all participants were tested by an ergometer cycle test, a 6-min walk (6MW) test and a 5-repetition-sit-to-stand (5RSS) test.
The ergometer cycle test was performed in accordance with the standard for exercise testing of the American Heart Association (14). The maximal physical capacity test was used as an indirect measure of the maximum exercise capacity. Participants started at 50 Watt (W), with a 25-W load increase for each 2 min until the participants could no longer maintain a speed of 60 rotations/min due to fatigue/dyspnoea.
The 6MW test is a simple, safe and inexpensive test to estimate submaximum exercise capacity. The test results correlate well with functional capacity and can be used prognostically (15).
The 5RSS test is also a simple, safe and inexpensive test evaluating the strength of the lower extremities by the patient standing up from a sitting position as quickly as possible 5 times in a row (16).
All tests were performed by one of 2 trained physiotherapists, who were blinded to whether the participant participated in rehabilitation.
Quality of life. From the study by Arribas et al. in 2010 (17), mean and standard deviation (SD) of AF-QoL-18 in a population of Spanish patients with AF were stated to be: mean 38.9 and (SD 21.5). With a level of significance of 0.05, a power of 0.8 and a difference between groups of 17 (corresponding to, for example, means 39 and 22), the necessary number of patients in each randomization arm is n = 26. No power calculation was made in relation to the other questionnaires.
Maximum exercise capacity. Hegbom et al., in 2006 (7), compared changes in maximum exercise capacity between 2 groups of patients with AF, of which only one group received active exercise therapy. From this paper, mean and SD of changes in measure of maximum exercise capacity (CW max) are stated as 0.3 and 0.26 (W × min), respectively. With a level of significance of 0.05, a power of 0.8 and a difference between groups of 0.3 (corresponding to, for example, means before/after of 1.3/1.6 for the active group and 1.3/1.3 for the passive group), the necessary number of patients in each randomization arm is n = 16.
The differences in time course in mean outcome values between the 2 randomization groups at baseline and at 3, 6 and 12 months were analysed by repeated measures ANOVA, taking into account the within-patient correlation. All hypotheses were specified a priori, thus, no corrections for multiple testing were made (18). Assumptions of normality and variance homogeneity were assessed by residual plots. Sensitivity analyses were performed using robust variance estimation to manage potential variance heterogeneity, using log-transformed data to accommodate right skewness and using bootstrap when assumptions in general were not met. Stata statistical software (version 13; StataCorp LP, College Station, TX, USA) was used for randomization and analyses. Two-tailed p-values <0.05 were considered statistically significant.
All patients received oral and written information, emphasizing that participating in the study was voluntary and withdrawing their informed consent at any time would not affect the present or future treatment. The project was approved by the local ethics committee (approval number N-20120002) and conducted in conformity with the Declaration of Helsinki.
Data were collected according to the principles of good clinical practice and the project was reported to the Danish Data Protection Agency (2008-58-0028).
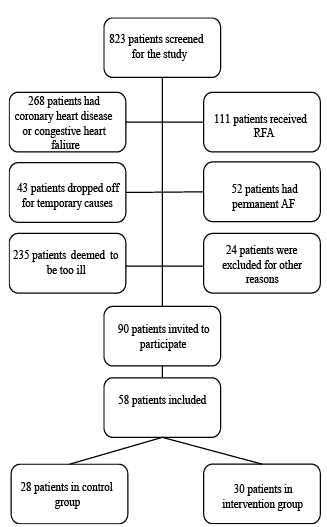
A total of 823 patients were screened. The majority of patients did not meet the inclusion criteria (Fig. 1). The low inclusion rate (7%) was explained mainly by exclusion of patients who were eligible for other rehabilitation programmes or experienced comorbidities. Consequently, 90 patients eligible for inclusion were invited to participate in the study, of whom 58 (64%) accepted the invitation. Barriers to participation were mostly time-consumption or not being able to participate due to the patients’ work.
Fig. 1. Fig. 1. Flowchart of participants. RFA: radio frequency ablation, AF: atrial fibrillation.
Two patients from the rehabilitation group and 4 from the control group did not return the questionnaires and were lost to follow-up. Over 80% of the intervention group participated in ≥ 75% of the rehabilitation programme.
Baseline characteristics of participants are listed in Table I.
Table I. Baseline characteristics of participants. All values are given as numbers unless otherwise stated in the table
For all QoL questionnaires, the trend was an increase in QoL from the baseline to 6 months questionnaire, which was higher in the intervention group than in the control group, although not all differences were statistically significant.
Using the AF-QoL-18 questionnaire, we found that the intervention group had a significantly higher increase in score during the first 6 months, but only a minor not statistically significant difference at 12 months (Table II and Fig. 2a). When separating the AF-QoL-18 into the 3 domains (physical, psychological and sexual activity), we found the same trend in all 3 sub-analyses, with the most pronounced effect in the physical domain (data not shown).
Results from the AFEQT questionnaire were similar (Table II and Fig. 2b).
Table II. Scores from quality of life (QoL) questionnaires at baseline and after 3, 6 and 12 months. The first column with p-values stems from the unpaired comparison between treatment groups at baseline. Subsequent p-values stem from unpaired comparisons of changes from baseline
Fig. 2a–e. Quality of life (QoL) scores (using 5 different QoL questionnaires) for patients with atrial fibrillation (AF) randomized to participate in a 12-week multifaceted rehabilitation programme vs usual care at 3, 6 and 12 months after inclusion in the study. Shown with 95% confidence intervals (95% CI). (a) Quality of Life in patients with Atrial Fibrillation (AF-QoL) (b) Atrial Fibrillation Effect on QualiTy of Life (AFEQT:) (c) Generalised Anxiety Disorder Assessment (GAD-7) (d) Patient Health Questionnaire (PHQ-9); (e) visual analogue scale (EQVAS).
The PHQ9 and GAD questionnaires showed that patients in both groups achieved a higher QoL after 6 months, but the increase was statistically significantly higher in the intervention group. From 6 to 12 months a lower QoL was found in both groups without statistical significance at the end of the study (Table II and Figs 2c and 2d).
A similar trend was found using the EQVAS, with an initial not statistically significant increase in QoL for the intervention group that decreased at the end of the study (Table II and Fig. 2e).
As shown in Fig. 3 and Table III, the participants in the intervention group had a lower maximum exercise capacity and oxygen (O2) uptake and an inferior performance in the 5RSS test at baseline than the control group despite the electronic randomization. The control group did not improve their exercise capacity and O2 uptake during the study, whereas in the intervention group, the maximum exercise capacity increased significantly from baseline to 3 months and remained steady until 6 months. The maximum O2 uptake increased from 29.0 ml O2/kg (SD 7.3) at baseline to 31.1 (SD 7.4) after 6 months.
In the 5RSS test, the rehabilitation group improved during the first 3 months and remained approximately the same for the next 3 months. The control group remained at the same level during the first 3 months but improved from 3 to 6 months. Thus, the difference between the 2 groups was the same at 6 months as at baseline (Fig. 3 and Table III).
Fig. 3a–d. Results from physical tests for patients with atrial fibrillation (AF) randomized to participate in a 12-week rehabilitation programme including physical exercise and education vs usual care at baseline and 3 and 6 months after inclusion in the study. Shown with 95% confidence intervals (95% CI). (a) Maximum exercise capacity; (b) maximum O2 uptake; (c) Five-repetition-sit-to-stand test; (d) 6-min walk test.
Table III. Results of physical score tests at baseline and after 3 and 6 months. The first column with p-values stems from the unpaired comparison between treatment groups at baseline. The subsequent p-values stem from unpaired comparisons of changes from baseline
In the 6MW test, the baseline mean distance was similar between groups. A small improvement was observed in both groups from baseline to 6 months, but no statistically significant difference between groups.
Nine patients had AF during one or more of the physical tests. Stratification for AF or sinus rhythm did not change the results of the physical tests significantly, but wider confidence intervals were observed.
Plots of residuals showed no violations of model assumptions. Sensitivity analyses confirmed our findings. Hence, the conclusions did not depend on a normal distribution of data or variance/covariance structure of data. Stratification by physical capacity at baseline, age, sex and type of AF did not differ from the main results.
No patients experienced adverse events during training.
During the study period, 38 patients had at least one readmission for cardiac reasons, mostly AF (rehabilitation group: 20 and control group: 18), 25 had at least one direct current cardioversion (rehabilitation group: 13 and control group: 12) and 11 had a radiofrequency ablation (rehabilitation group: 7 and control group: 4). There was no statistically significant difference between groups.
This study found that a full rehabilitation programme including group education and physical training for patients with paroxysmal or persistent AF was beneficial, with statistically significant improvement of QoL measured with both disease-specific (AF-QoL-18, AFEQT) and non-disease-specific (GAD-7, PHQ-9, EQ-5D) questionnaires during the first 6 months, after which the effect attenuated.
Five different questionnaires were used to assess different aspects of QoL. In all questionnaires, there was an increase in QoL for all participants from the start to the end of the study, which was consistent with results from other studies (19, 20). The intervention group experienced a higher increase in QoL during the first 6 months (although not statistically significant in all questionnaires) and a subsequent attenuation of the intervention effect compared with the control group. An earlier study regarding the AFEQT questionnaire suggested that a mean change of approximately 12 points was correlated with a small improvement and < 5.3 points was an unimportant improvement (21). Our study showed a difference of 7.6 points after 3 months, potentially suggesting a small clinical importance.
In addition, a positive effect was found on maximum O2 uptake, whereas no convincing improvement was found in the other physical tests.
At baseline, there was a statistically significant difference between the intervention and the control group in the performance of the physical tests despite randomization. However, this did not have any statistically significant effect on the results, as stratification by O2 uptake at baseline did not show a different effect of training in patients with a low O2 uptake compared with those with a high uptake.
Physical exercise has been shown to reduce the risk and magnitude of, for example, hypertension, diabetes mellitus and obesity, and has been shown to be beneficial for patients with CHD and congestive heart failure (22, 23). Thus, physical exercise may potentially lead to a reduction in the risk of developing AF. However, long duration of vigorous training may increase the risk of developing AF (8), although it seems that moderate physical exercise have a protective effect on patients with permanent AF (8, 24). Regarding physical exercise and non-permanent AF, Malmo et al. (25) found that aerobic interval training reduced the time in AF and improved QoL estimated from the Short Form-36 (SF-36) questionnaire. Furthermore, training also significantly improved AF symptoms, VO2 peak, left atrial and ventricular function.
Risom et al. (26) conducted a 12-week randomized trial on rehabilitation for patients with paroxysmal or persistent AF after catheter ablation. The authors found an improved physical capacity assessed by VO2 peak, which is in line with our results. The authors did not find a statistically significant improvement in the 6MW test in the training group compared with the control group, which was comparable with our results. They did not find an improvement of the mental health based on a non-disease specific questionnaire. As radiofrequency ablation was an exclusion criterion in our study the results cannot be directly compared.
Skielboe et al. included 76 patients with paroxysmal or persistent AF who were randomized to high- or low-intensity exercise for 12 weeks. Both groups improved their peak VO2 significantly (11). QoL was not measured. Recent studies have compared AF patients and non-AF patients who joined a cardiac rehabilitation programme for other cardiovascular diseases or cardiovascular risk factors. Younis et al. found that patients with AF initially had lower physical capacity than non-AF participants, but improvement in physical capacity diminished the risk of total mortality and cardiovascular hospitalization for both groups (27). In a case control study Reed et al. found that rehabilitation improved QoL in both groups, but to a greater extent in patients without AF (28).
Although patients with paroxysmal AF may be in sinus rhythm most of the time, they may be less likely to be physically active because of anxiety about initiating AF (29). Even when patients were in sinus rhythm, this study showed that QoL and physical capacity could be improved. We also found an improvement of the 6MW test in the control group, perhaps because participating in the study encouraged patients to be more physically active even though they were in the control group. The bicycle tests favoured the intervention group, probably because bicycle training was a central part of the physical exercise programme.
Establishing whether physical exercise in patients with AF would be beneficial to reduce the risk of comorbidities and the burden of AF will require larger studies with longer follow-up.
The rehabilitation programme seemed to have the highest impact on reducing anxiety and depression and increasing physical and psychological well-being (estimated by questionnaires with focus on these domains: AF-QoL-18, GAD-7 and PHQ-9) and alleviating patients’ symptoms (as assessed by AFEQT).
The strengths of this study include a complete rehabilitation programme, the use of disease-specific individualized training programmes and exercise tests performed by physiotherapists who were blinded to the 2 groups.
The study included patients with paroxysmal or persistent AF, whereas other studies have primarily included patients with permanent AF. Thus, in general, participants in our study seemed to have higher baseline scores compared with an unselected population of AF (17). Dudrik et al. have previously shown that progression from paroxysmal to persistent AF is associated with a decrease in health-related quality of life (30). We therefore performed stratified analyses on type of AF, but we did not find any differences in the effect of rehabilitation between the 2 groups.
This study examined the effect of a complete rehabilitation programme for patients with AF. Previous studies have shown beneficial effects of education about anticoagulation treatment on treatment compliance and found that physical training was beneficial regarding physical capacity and QoL (7, 9, 24, 28). In addition, non-randomized studies indicated a beneficial effect of physical exercise, weight loss, and aggressive risk factor management (5–7).
The primary limitation was the number of participants, although it was comparable with other studies in patients with AF (7–11). The physical training of the control group was not monitored. Due to logistics we could not include all relevant patients. Patients could not be included if they were admitted for a short period when no nurse or physicians leading the study were on duty, However, this is non-systematic selection and could therefore not influence the study results. Also, a precise registration of the AF burden would have been optimal, e.g. implanting a loop-recorder. However, the economy of the study was restricted. No information was collected regarding the degree of the patients’ physical activity during the follow-up period, which could affect the QoL scores.
Thus, this study has limitations. No long-term positive effect of patient education and physical training on QoL of the studied patients was found. Therefore, the cost-effectiveness of this rehabilitation programme for this patient group is questionable.
This study indicated that a multifaceted rehabilitation programme including education and physical training in patients with paroxysmal or persistent AF may have a beneficial short-term (but no long-term) effect on QoL and physical exercise capacity estimated with disease-specific and generic QoL questionnaires.
The authors would like to thank physiotherapists Rikke Niemann Hargaard, Kasper Juul Larsen, and Klaus Sletten Kristensen for their instruction in the physical exercise training and physiotherapists Camilla Zyrmylen and Thomas Wibaek Asp for performing the blinded physical tests. Thanks to clinical dietitian Lonneke Hjermitslev and clinical psychologist Lisbeth Hede Jørgensen for their assistance in the education. This study was supported by the Research Foundation of the Medical Association of North Jutland and the Aalborg AF Study Group.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize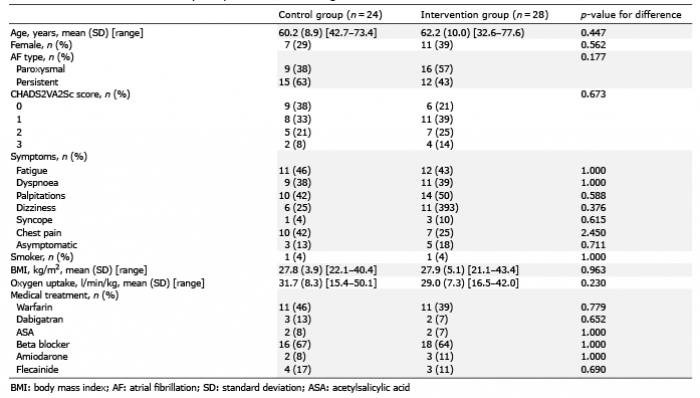 Click to show fullsize
Click to show fullsize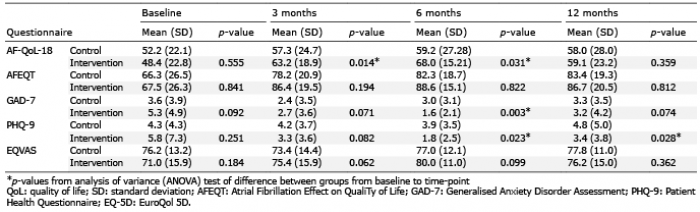 Click to show fullsize
Click to show fullsize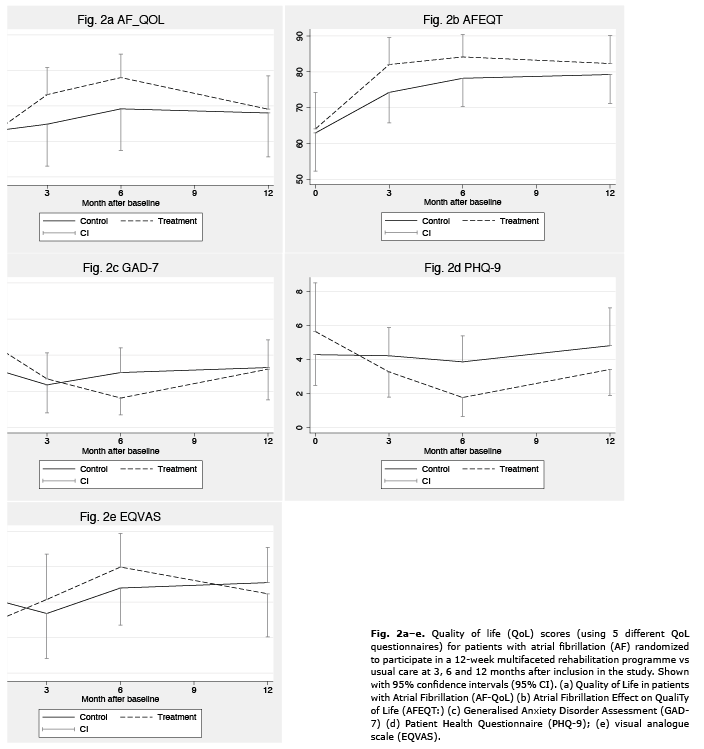 Click to show fullsize
Click to show fullsize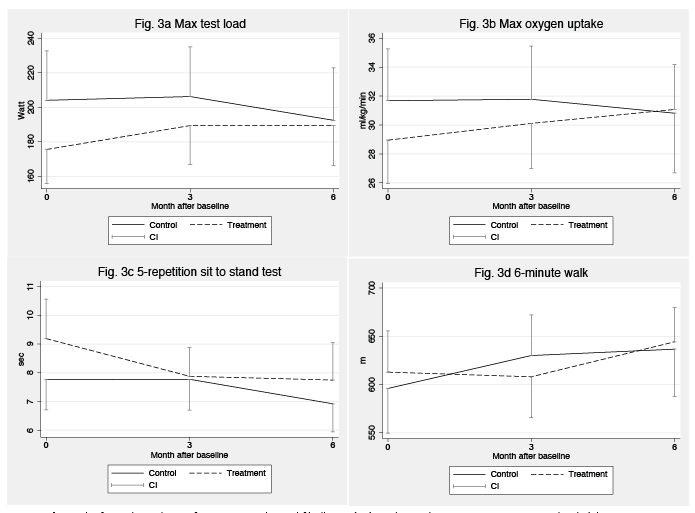 Click to show fullsize
Click to show fullsize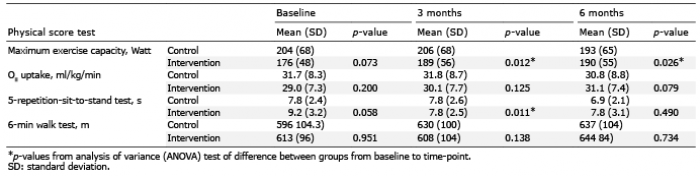 Click to show fullsize
Click to show fullsize