
From the 1Department of Clinical Neuroscience, Rehabilitation Medicine, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, 2Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, 3Departement of Health and Rehabilitation, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, 4RISE Acreo, Gothenburg, Sweden
Objective: To determine whether there are differences in arm, leg and trunk activity measured by acceleration between weekdays and weekends in people undergoing rehabilitation in the subacute stage after stroke.
Design: Cross-sectional study.
Patients: Twenty-eight individuals with stroke (mean age 55.4 years; severe to mild impairment) and 10 healthy controls.
Methods: A set of 5 3-axial accelerometers were used on the trunk, wrists and ankles during 2 48-h sessions at weekdays and over a weekend. Day-time acceleration raw data were expressed as the signal magnitude area. Asymmetry between the affected and less-affected limb was calculated as a ratio.
Results: Participants with stroke used their both arms and legs less at weekends than on weekdays (p < 0.05, effect size 0.32–0.57). Asymmetry between the affected and less-affected arm was greater at weekends (p < 0.05, effect size 0.32). All activity measures, apart from the less-affected arm on weekdays, were lower in stroke compared with controls (p < 0.05, effect size 0.4–0.8). No statistically significant differences were detected between weekday and weekend activity for the control group. One-third of participants perceived the trunk sensor as inconvenient to wear.
Conclusion: Increased focus needs to be applied on activities carried out during weekends at rehabilitation wards.
Key words: stroke; physical activity; accelerometry; rehabilitation; weekday weekend differences; ambulatory monitoring; wearable technology; patient preference.
Accepted Mar 22, 2019; Epub ahead of print Apr 2, 2019
J Rehabil Med 2019; 51: 426–433
Correspondence address: Margit Alt Murphy, Rehabilitation Medicine, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Per Dubbsgatan 14, SE413 45 Gothenburg, Sweden. E-mail: margit.alt-murphy@neuro.gu.se
Individuals with stroke have difficulty achieving the recommended levels of physical activity. The physical environment and support provided can also influence activity levels. This study aimed to determine whether there are differences between weekdays and weekends in arm, leg and trunk activity measured by acceleration in people undergoing rehabilitation in the subacute stage after stroke. The results showed that people with hemiparesis in the inpatient rehabilitation setting use not only their more-affected, but also their less-affected arm and leg less at weekends than on weekdays. Thus, the challenge during inpatient rehabilitation is to identify patients who might need extra support to be able to maintain their physical activities at weekends, facilitate activity on all days of the week, and take full advantage of the recovery process.
Individuals with stroke have difficulty achieving the recommended levels of physical activity, despite that the physical activity is a key component of primary and secondary prevention of stroke (1). Behavioural mapping studies show that individuals with stroke spend approximately 70–80% of waking hours in lying or sitting, both in subacute and chronic stages (2–6). In hospital settings, during a typical day of rehabilitation, patients were physically active for approximate 23 min and spent only 1 min in vigorous activity (7). Studies using accelerometers show that community-dwelling stroke survivors took approximately half the number of steps per day compared with healthy controls (8), and that individuals with stroke remain sedentary at least 1 year after stroke (9). Similarly, the paretic arm was used for a mean of 3 h per day and the non-paretic arm for 6 h per day early after stroke compared with 8.5 h in non-disabled controls (10).
Wearable devices, such as accelerometers, are increasingly used to objectively measure activity levels in stroke. The majority of studies in stroke report step or activity counts or duration of activity/inactivity (e.g. time spent in walking, sitting or lying) measured with a single or a set of 2–3 activity sensors on the lower body (11). Similarly, duration of arm activity, measured as activity counts and a ratio of paretic to non-paretic arm, are frequently reported (12). Commonly, proprietary algorithms are used to generate step or activity counts, which makes comparison between devices and studies difficult (13). Thus, reporting accelerometer metrics in terms of acceleration (m/s2) is advocated in order to allow data comparison across devices, studies and populations (13, 14). The feasibility of using activity sensors that allow raw data handling in clinical settings needs to be evaluated further.
The physical environment and support provided are factors that influence activity levels early after stroke (15, 16). In many rehabilitation wards scheduled therapy sessions with physiotherapists and occupational therapists are provided only on weekdays (2). Even when the patients have the opportunity to carry out self-training exercises with or without assistance and are encouraged to be active at weekends, the activity levels might be lower at weekends. In addition, weekends can be perceived by patients and staff as days of rest, which may influence the activity levels (12). A recent study in chronic stroke found differences between weekday and weekend data for walking time and step count, with more activity occurring on weekdays, whereas time in sitting, standing and in light or moderate PA did not differ (17). Real-world activity and how this activity is distributed over a week during stroke rehabilitation are still not well described (12).
The primary aim of this study was to quantify arm, leg and trunk activity in people with hemiparesis after stroke during inpatient rehabilitation, and to determine whether there were differences in activity levels between weekdays and weekends. The hypothesis was that the activity levels are lower at weekends when scheduled activities are limited. It was also expected that the activity levels would be lower in stroke compared with healthy controls. The feasibility of the sensor measurement in terms of comfort, acceptance and management in the clinical setting was also explored.
Participants were recruited consecutively from an inpatient rehabilitation ward at Sahlgrenska University Hospital for an 8-month period during 2015 and 2017. Preliminary power analysis was not possible, since no data on the accelerometer measure used in the current study have been published earlier. Confirmatory power analysis was performed based on the accelerometer data (m/s2) from the arm and leg sensors after data from 11 individuals was collected (18). To detect differences between weekday and weekend sessions with 80% power and alpha level equal to 0.05 and accounting for 10% missing data, 28 participants with stroke were required.
In total, 28 individuals with stroke were included in this cross-sectional study. The inclusion criteria were: first-ever ischaemic or haemorrhagic stroke, age 18 years or older, having the ability to walk with or without assistance, and not receiving a full score on the Fugl-Meyer Assessment of the affected arm or leg. Individuals with another condition affecting arm or leg function, or having severe multi-impairment prior to stroke or malignancy, and those unable to understand verbal instructions in Swedish or English were excluded. All participants with stroke followed an individual rehabilitation plan in accordance with the National Swedish Stroke Guidelines. Each patient had an individual time schedule that included at least one 45-min session with a physiotherapist and 1 with an occupational therapist per day, 5 days per week, together with group activities (walking, gaming) and individual therapy with other rehabilitation team members (e.g. speech therapist). In the ward, an equipped therapy room, gaming room and common room for meals, as well as a therapy garden and walking paths outside the hospital building, were available for day-time use. Patients were also encouraged to perform self-training with or without assistance from the nursing staff or next of kin at weekends.
A convenience sample of 10 healthy individuals with varying occupation, age and sex was included as a healthy control group to allow better interpretation of the activity levels in individuals with stroke. Healthy participants were included if they did not report any medical, neurological or musculoskeletal disorders affecting their motor function or everyday physical activity and were able to communicate in Swedish or English.
Ethical approval for the study was provided by the Regional Ethical Review Board in Gothenburg, Sweden (507-15). Written and verbal informed consent was received from all participants prior to participation in the study.
Accelerometer data were collected using a set of 5 3-axial accelerometers (Shimmer 3, Shimmer, Dublin, Ireland) during 2 separate 48-h sessions on weekdays and over a weekend, respectively. The sensors were calibrated according to the procedure from the supplier before use. The weekday measurement was performed during any 2 consecutive days between Monday and Friday. The sampling rate was set to 51.2 Hz, with an accelerometer range of ± 8 g. Accelerometers (51 × 34 × 14 mm, weight 24 g) were fastened with customized Velcro straps on the trunk, wrists and ankles. Participants were instructed to wear the sensors during the entire session, including the night, but the sensors could be removed at any time when necessary. Since the sensors were not waterproof they had to be removed for showering or swimming activities.
Participants were asked to record their main daily activities using an activity log. For each hour between 08.00 h and 20.00 h participants recorded their main activities (e.g. eating, taking a walk, training, preparing a meal, transport in a car, working in the garden) and whether the activity was mostly sitting, standing/walking, or lying/resting. Participants who were unable to complete the log were interviewed during and after the measurement period. The weekday schedule data, including training sessions, were collected for the participants with stroke. The logs were used to describe the participants’ main daily activities.
Data acquired from the sensors were extracted to Matlab software (MathWorks Inc.) for custom-made analysis. Only the day-time activity between 08.00 h and 20.00 h were extracted. All data were visually inspected to identify segments in which the sensor data contained no motion information or were missing. Primarily, this occurred when the participant had removed one or more sensors from their body, e.g. for taking a shower. Such segments were documented and removed from the measurement data. Corrupt measurement data time-stamps, possibly caused by sensor synchronization malfunction, were reconstructed using uniform resampling of the accelerometer data.
The length of the available data for each participant was then calculated and needed to be at least 20 h out of a possible 24 h to be included in the analysis. This criterion was applied to the individual sensors for weekdays and weekends separately. For calculation of ratios, data needed to be available for both limbs. The extracted measurement data were filtered using a Butterworth bandpass filter (0.2–10 Hz passband). The activity level was expressed as the Signal Magnitude Area (SMA), which is computed from the 1-norm of the acceleration vector averaged over a fixed epoch length (T = 120s) and, thus, resulting in 1 value each epoch
Furthermore, the SMA ratio (more affected/less affected in stroke or non-dominant/dominant in controls) was computed for arms and legs as a measure of asymmetry. The logarithm of the SMA ratios was used to obtain a measure that was symmetrical with respect to both limbs. The value zero indicates perfect symmetry between limbs, while a negative value indicates that the SMA is lower in the affected limb or non-dominant limb. The SMA for trunk, both arms and legs along with ratios were averaged over subsequent days of measurement to produce a single value for each weekday and weekend session.
Clinical assessments
In stroke, the upper and lower extremity sensorimotor function was assessed using Fugl-Meyer Assessment (FMA) (19–21). The maximum score of 66 and 34 for the upper and lower extremity, respectively, indicates normal function. The FMA sensation, passive range of motion and pain were also assessed. The muscle tone in elbow, wrist and ankle joint was assessed using the Modified Ashworth Scale (22). Walking ability was dichotomized to independent (scores 4–5) and dependent (scores 0–3) according to Functional Ambulation Categories (FAC, 0–5 pts) (23, 24). The stroke type was gathered from medical charts and hand dominance by participants’ own reporting.
Feasibility evaluation
At the end of each measurement session, participants were asked to rate whether the sensors were comfortable to wear on a 5-point scale (strongly agree, agree, agree partly, do not agree, strongly disagree) and describe their experience and perception of the measurement. When the participants with stroke had difficulties expressing themselves their next of kin or staff at the rehabilitation ward that had assisted the participant was interviewed. Comments regarding the practical management of sensors were also collected. This data were summarized descriptively.
Statistical analysis
Statistical analyses were conducted using IBM Statistical Package for Social Sciences™ (SPSS) version 24. The alpha value was set to 0.05 (2-tailed). The activity logs were analysed descriptively. Since some accelerometer measures showed non-normal distribution and the sample size was not very large, non-parametric statistics were used.
To verify whether there was a difference in activity levels between weekdays and weekends, Wilcoxon signed-rank test was used. Wilcoxon signed-rank test was used to determine differences between the more-affected and less-affected limb in stroke and between the dominant and non-dominant limb in controls. The Mann–Whitney U test was used to test whether the activity levels in individuals with stroke were different from controls. Possible interaction effect of dominant/non-dominant affected hand on arm activity and independence/dependence in walking on leg activity were verified by using between-within subjects analysis of variance.
The relative magnitude of the differences between groups was calculated using effect size estimates for non-parametric data (r = z/√N) and Cohen’s guidelines were followed while interpreting the effect sizes, where 0.1, 0.3 and 0.5 indicate small, medium and large effect sizes, respectively (25).
The measurement protocol was followed in all 28 participants with stroke and 10 healthy controls. Among individuals with stroke, no data were recorded in oneparticipant due to battery malfunction and in another due to non-adherence related to cognitive impairment. These measurements were fully missing (all 5 sensors, both sessions) and therefore excluded from the data analysis (Table I). For the remaining measurements from 26 participants with stroke and 10 controls (36 measurements from 5 sensors in 2 sessions = 360 measurements), 11.9% had less than 20 h data and were signified as incomplete (Table I). Data from all 5 sensors during a weekend measurement session (1.4% of total 360 measurements) was missing since the patient forgot to apply the sensors (human factor). All other data loss was due to technical failure and random (10.5%). Thus, in all collected data including measurements from the 2 excluded participants (380 measurements) human error accounted for 3.9% and technical failure for 12.6% of missing/incomplete data. Common technical failures were malfunction of battery or memory card, failure of wireless synchronization between the sensors or failure occurring during data transfer.
Table I. The summary of data availability showing missing and incomplete data
The demographic and clinical characteristics of the individuals with stroke are shown in Table II. The control group included 10 individuals (4 men, 6 women) between 32 and 64 years (mean 50.6 years, SD 11.8). All healthy controls were right-hand dominant. The FMA scores of upper and lower extremities ranged between 7–65 and 8–33, respectively, which indicates that persons with both low and high sensorimotor function were included.
Table II. Demographic data and clinical characteristics of individuals with stroke (n = 26).
The activity logs showed that participants with stroke spent approximately 70% of the daytime in sitting (Fig. 1). The time in sitting activities was comparable between weekdays and weekends, but slightly more time was spent in standing/walking on weekdays (19%) and slightly more time in lying/resting at weekends (20%). Among healthy controls, 63% was spent in sitting, 36% in standing/walking activities, and almost nothing in lying or resting on weekdays (workdays). At weekends, however, 12% was spent in lying/resting and 44% of time was equally spent in sitting or standing/walking activities.
Fig. 1. Percentage of time spent in sitting, standing/walking or lying/resting activities during the daytime between 08.00 h and 20.00 h, based on the reported activity logs.
The main reported activities in stroke were eating, watching TV, rest, walking or training, transport by car, light household activities and shopping, computer gaming, social activities such as meeting and talking with others, playing with children. Among the healthy controls, 5 were working in an office environment and 5 had clinical work in hospital setting. The main activities on weekdays reported by the controls were: working with the computer, clinical work with patients, meetings, shopping, making food, driving, using public transport, cycling, and occasional training (biking, gym, yoga). On weekends the activities reported were: shopping, driving, household activities, cultural activities, such as going to a museum, concert, and coffee shop, reading, studying, watching TV, walking, working in the garden and ice-skating.
Differences in activity levels on weekdays and weekends
Participants with stroke showed lower arm and leg activity at weekends compared with weekdays (Table III, Fig. 2A and 2B). The largest difference between weekdays and weekend was observed for the affected arm (z = 3.67, p < 0.001, r = 0.57) followed by the less-affected leg (r = 0.41), less-affected arm (r=0.37) and affected leg activity (r = 0.32). As expected, participants with stroke used their more-affected arm less compared with the less-affected arm at both sessions (z = 3.95/3.82, p < 001, r = 0.59/0.62). This difference was also reflected in the arm ratio measure (Table III, Fig. 2C), which showed larger asymmetry at weekends (z = 2.07, p < 0.05, r = 0.32). This indicates that the participants with stroke relied even more on their less-affected arm during normal daily activities at weekends. There was no interaction effect between arm activity and hand dominance of the affected arm (p > 0.37).
The more affected leg was also less active compared with the less-affected leg at both sessions (z = 3.88/3.18, p < 0.001, r = 0.58/0.48), but the asymmetry between the legs remained the same between weekdays and weekends. The trunk activity showed no difference between weekdays in participants with stroke (z = 1.67, p = 0.098, Fig. 2D). No statistically significant differences could be observed in healthy controls between weekdays and weekends (Table III). There was no interaction effect between leg activity and independence in walking (p > 0.55).
Table III. Acceleration data in individuals with stroke and healthy controls for weekday and weekend measurement sessions
Fig. 2. Activity levels of (A) upper extremities, (B) lower extremities, (C) arm and leg ratios (more-affected side/less-affected side), and (D) trunk in stroke and controls. Statistically significant differences between weekdays and weekends are indicated accordingly: p < 0.05*, p < 0.01**, p < 0.01***. Outliers are shown as black dots. (C) SMA ratio (log) equal to 0 indicates symmetry between the limbs, shown as a dotted line. SMA: signal magnitude area; IQR: interquartile range.
Activity levels in stroke compared with healthy controls
Participants with stroke showed lower activity (z > 3.28, p < 0.05, r > 0.61) in both limbs compared with controls, except for the less-affected arm at weekdays (z = 1.61, p = 0.11). The median value of the arm activity in healthy controls was twice as large and leg activity 3 times as large compared with the affected limbs in stroke. Also the asymmetry between limbs (SMA ratio) in stroke was larger between arms (z > 2.22, p < 0.05, r>0.40) and legs (z > 2.73, p < 0.01, r > 0.51) than in controls.
Feasibility evaluation
Wearing sensors for 2 sessions of 48 h including the night was perceived as acceptable by most of the participants. Approximately half of the participants described that they forgot that they were wearing the sensors at some point. The trunk sensor was, how-ever, perceived uncomfortable or even disturbing by one-third and 8 reported problems with Velcro straps (too loose or tight, skin irritation) and/or that the sensors were in the way while getting dressed. Five expressed that it was relieving to take the sensors off after a measurement period. Two worried whether the sensors were always correctly placed, e.g. when donned after showering. A few found the measurement stimulating and were interested to get feedback of the results. One participant described a feeling of being watched over, and one preferred to wear the sensors under the clothes, not visible to others. The sensors were well tolerated overnight, but 5 individuals found the blinking from light-emitting diode (LED) lights on the sensors, especially in the darkness, disturbing. Two control participants working at hospital needed to remove sensors on the arms occasionally due to the hygiene rules. In rating their perception whether the sensors were comfortable to wear, one agreed strongly (3%), 11 agreed (30%), 19 agreed partly (53%), and 5 did not agree (14%). No adverse effects were reported. The management of multiple sensors and the need for customized application for increased convenience was perceived as a barrier for clinical feasibility by the researcher collecting the data.
After stroke, people with hemiparesis in the inpatient rehabilitation setting use not only their more-affected, but also their less-affected, arm and leg less at weekends than on weekdays. Asymmetry in arm use, indicated by a ratio of paretic to non-paretic arm, was increased at weekends in people with stroke. Healthy controls did not show differences between weekday and weekend measurements in any of the activity metrics. The findings of the current study, showing differences in arm and leg activity levels between weekdays and weekends, are novel. The results also imply that the acceleration metrics used in this study were sensitive enough to capture differences in activity levels dependent on whether the measurement was performed on a weekday or weekend.
There may be many factors that influence the activity levels among people with hemiparesis after stroke in the inpatient settings. The impairment level can vary from very severe to mild, meaning that the need for assistance in different activities varies. The hospital environment itself, the number of staff available, and decisions on rehabilitation routines might be a contributing factor influencing activity levels (26–28). Differences in activity at weekdays and weekends can also be influenced by cultural, religious or social norms, e.g. perceiving Sundays as a day of rest (29).
The current study did not reveal any differences in trunk and limb activity between weekdays among healthy controls. Similar results have been found for working age and older community-dwelling adult populations, revealing no difference in time spent in sitting/standing/walking or number of steps taken between weekdays and weekends (30, 31). Others have shown that older adults took fewer steps and spent less time in moderate PA on Sundays compared with weekdays (29). In chronic stroke, the findings are divergent regarding differences in PA between weekdays. A study, using activity sensors on the non-paretic leg, waist and upper arm, found differences for stepping time and step counts, but not for time spent in sitting, standing, or in light/moderate intensity PA (17). Another study using an accelerometer worn on the hip showed no difference in daily activity counts between weekdays and weekends (32). In an inpatient rehabilitation unit the time spent in task practice and exercise was observed to be 14% and 2% on weekdays, and only 7% and 1% at weekends, respectively (27). In the current study, both the more-affected and less-affected limbs were used less at weekends compared with weekdays. This difference in activity cannot be accounted for by changes in arm function, since the weekday and weekend measurement sessions were conducted within the same week, the weekday session prior to the weekend session. The asymmetry between arms was also greater at weekends, which may have been caused by a combination of a generally lower activity at weekends and that the less-affected arm was used more at weekends to compensate for the limited ability of the affected arm. Since neither physiotherapists nor occupational therapists were present at weekends, it can be expected that less focus was possibly paid to affected arm use at weekends.
In the current study the use of less-affected arm at weekdays was the only metric that reached comparable activity levels to healthy controls. This corroborates findings from previous studies, showing that the activity levels are, in general, low after stroke. The added knowledge from the current study is that the arm activity was lower and asymmetry increased at weekends irrespective of the hand dominance of the affected side; and that the leg activity remained low regardless of whether the person was independent in walking or using a wheelchair. It has been proven that it is difficult for patients to bridge the gap between supervised and unsupervised practice and maintain the activity levels when alone (5, 33). Many promising attempts to promote increased activity among stroke survivors have been made, including elements from enriched environment, group exercise and use of technology, but challenges still remain (16, 34, 35).
The strength of the current study is that acceleration data were provided as acceleration rather than activity counts (14). The data were collected as raw signal and common non-proprietary post-processing methods were employed. Since direct comparisons between different accelerometer metrics is difficult, we also included a healthy control group. Activity levels from healthy controls can be used as goal estimates representing activity levels in people without disabilities. Another strength was that the activity logs were gathered, which provided a possibility to verify accelerometer data when needed. Use of activity logs, however, require extra effort and time and will be a limitation in clinical settings (12). A set of 5 sensors was used, which allowed a more comprehensive and differentiated analysis of activity levels. In our data-set no difference was found between weekdays and weekends in trunk activity. The placement of the trunk sensor was also perceived as most inconvenient for the participants. Thus, information from arms and legs may be enough to capture most of the activities of daily living, e.g. walking, transfers using either arms or legs, and manual activities.
A limitation of the study is the missing data. In total, out of all collected data from 5 sensors in 38 participants in 2 sessions (380 measurements), missing or incomplete data due to technical errors accounted for 12.6%. Reporting of missing data due to technical errors is not extensive, but similar levels ranging from 14% to 23% have been reported previously (36–38). To be fully clinically feasible, the missing data from accelerometers need to be minimal. In addition, use of accelerometers that allowed raw data handling was an advantage in the current study, but it also enclosed a disadvantage, since it required manual time-consuming post-processing. Accelerometers used were not waterproof and individual adjustments were needed for sensor placement. These disadvantages were reflected in the feasibility evaluation, where the participants commented that the sensors were in the way when getting dressed and that the straps, and particularly for the trunk sensor, were uncomfortable. Thus, these elements also need to be more convenient for the user before they can be used in clinical practice. Participants were aware of measurements, which may have motivated them to be more active. However, this bias might be negligible, since the current evidence indicates that the use of commercial activity monitors does not have an effect on daily step counts in people with stroke (39).
In conclusion, people with stroke in inpatient rehabilitation settings use not only their more-affected, but also their less-affected, upper and lower limbs less at weekends than on weekdays. To our knowledge this is the first study to report acceleration data (m/s2) from all extremities and the trunk in people with stroke in the inpatient rehabilitation setting. Wearing sensors for a total of 4 days was acceptable for the majority of subjects, although the trunk sensor was perceived as the most uncomfortable. A need for customized application of sensors on the body and manual data-processing were the main barriers to clinical feasibility. There is strong evidence that neural repair and functional recovery, to a large extent, take place during the subacute stage after stroke, which means that the therapeutic interventions at this stage may have the strongest impact on patients’ recovery. Thus, the challenge during inpatient rehabilitation is to identify patients who might need extra support to be able to maintain their physical activities at weekends, facilitate activity on all days of the week, and take full advantage of the recovery process.
The authors thank all participants in this study.
The study was funded by the Swedish Foundation for Strategic Research (SBE13-0086), the Swedish state under the agreement between the Swedish government and the country councils, the ALF-agreement (ALFGBG-775561), Swedish National Stroke Association, Rune and Ulla Amlöv Foundation for Neurology Research, JB Wenneström Foundation, Promobilia Foundation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize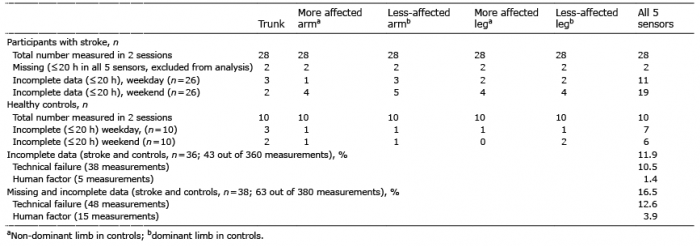 Click to show fullsize
Click to show fullsize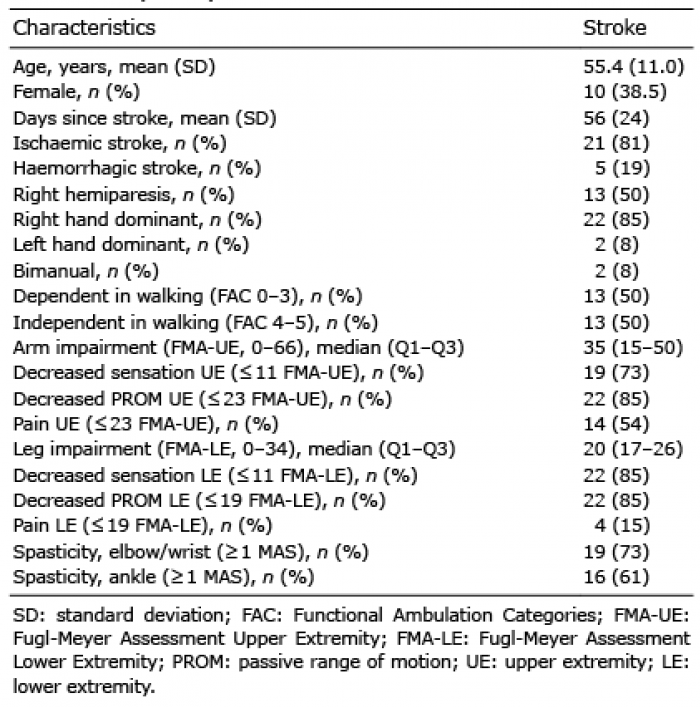 Click to show fullsize
Click to show fullsize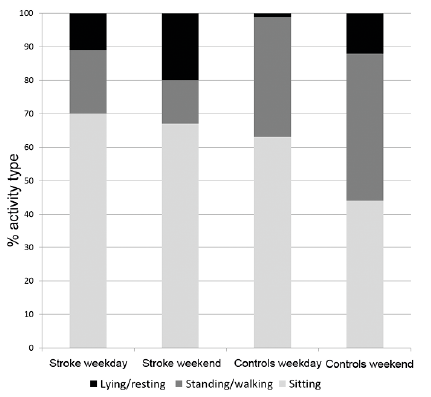 Click to show fullsize
Click to show fullsize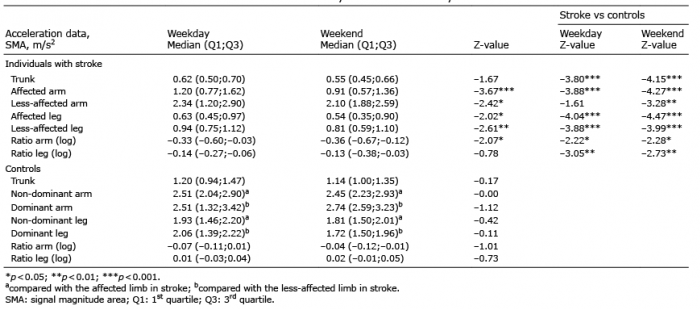 Click to show fullsize
Click to show fullsize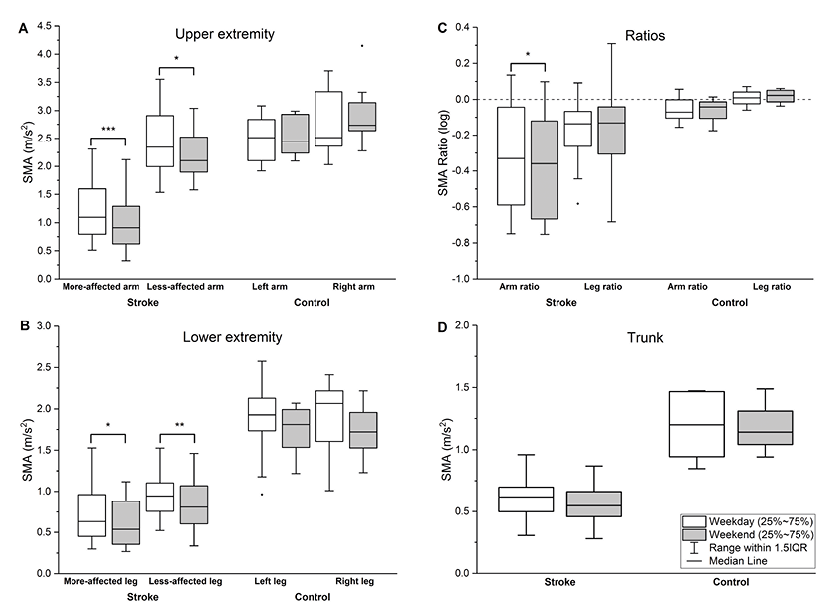 Click to show fullsize
Click to show fullsize