
From the ¹Glasgow Royal Infirmary, and ²University of Glasgow, School of Medicine, Glasgow Royal Infirmary, Glasgow, UK
Background: Intensive care unit survivors experience significant physical and psychological problems, including chronic pain following discharge. The aim of this study was to observe the incidence, anatomical sites, intensity, and interference of chronic pain in intensive care unit survivors over a 1-year period. In addition, potential predictors of chronic pain were analysed.
Methods: Data were collected during an intensive care unit follow-up programme as part of a quality improvement initiative. Data from the Brief Pain Inventory and from musculoskeletal assessment were examined, alongside demographic data from the patient. Data were collected from patients at baseline and at a 1-year follow-up appointment.
Results: Data from 47 intensive care unit survivors were included in this study. In 66% (n = 31) of the patients a “new” chronic pain that did not exist before their stay in the intensive care, was reported. Pain intensity in this patient group was “moderate”’ and did not improve significantly over the 1-year period. Although pain interference with life decreased over the study period, it was still the most common cause of reduced enjoyment of life and reduced employment at 1-year follow-up.
Conclusion: Chronic pain is associated with morbidity in intensive care unit survivors. Pain interference, but not pain intensity, improved significantly in the first year after discharge. Further multi-centre research is required to elucidate the chronic pain experience.
Key words: intensive care; chronic pain; post-intensive care syndrome; rehabilitation.
Accepted Apr 17, 2019; Epub ahead of print Apr 29, 2019
J Rehabil Med 2019; 51: 451–455
Correspondence address: Pamela MacTavish, Critical Care Department, Glasgow Royal Infirmary, Castle Street, Glasgow, G4 OSF, UK. E-mail: Pamela.mactavish@ggc.scot.nhs.uk
The sickest patients in a hospital often need treatment in an intensive care unit. When these patients eventually go home they often experience continuing psychological and physical problems, including pain. The aim of this study was to look at how often pain occurred in this group of patients, where the pain occurred, and if the pain was interfering with patient’s lives. We studied 47 patients after discharge from hospital and found that two-thirds of them had pain that they did not have before their stay in the intensive care unit. We followed up these patients over a 1-year period and found that the level of pain they experienced did not change over time. However, it did not interfere with their lives as much. Further studies are needed to find out why pain is such a major problem for intensive care unit survivors.
The number of patients surviving a critical illness is increasing worldwide (1). With this increasing survivorship, there is now a focus on understanding the recovery trajectory of patients (2). Evidence has shown that almost two-thirds of intensive care unit (ICU) survivors will experience significant physical, psychological, cognitive and social problems in the months and years following discharge from critical care (3–5). This group of signs and symptoms are now commonly referred to as “post intensive care syndrome” (PICS) (6).
An under-reported feature of PICS is chronic pain (7), defined as a “continuous, long-term pain of more than 12 weeks or after the time that healing would have been thought to have occurred in pain after trauma or surgery” (8). In the limited research published to date, almost three-quarters of ICU patients (73%) reported moderate or severe pain 12 months post-discharge (3). A further retrospective analysis of ICU patients estimated that the incidence of chronic pain in ICU survivors was as high as 44%, with the shoulder being the most commonly affected joint (9). A variety of risk factors for the development of chronic pain have been studied, including increasing patient age and severe sepsis (9). However, there is limited evidence about the intensity of pain and how this affects activities of daily living (ADL). Furthermore, there is a lack of evidence regarding how pain is treated pharmacologically.
The aims of this study were to assess the incidence, intensity and location of chronic pain; to explore the level of its interference in daily life; and examine the drugs required for its treatment. In addition, the study explored predictors for developing chronic pain in the ICU survivor population, and the changing nature of such pain over time.
Participants
Patients who attended the pilot phase of an ICU recovery programme were included in this evaluation. Intensive Care Syndrome: Promoting Independence and Return to Employment (InS:PIRE) is a 5-week, post-ICU, multi-disciplinary, peer-supported, rehabilitation programme. Patients who had been mechanically ventilated for more than 72 h or in high-dependency care for more than 2 weeks were invited to participate in InS:PIRE 6–20 weeks post hospital discharge. People who were further along the recovery trajectory, who self-referred into InS:PIRE, were also included. Exclusion criteria for the programme included: age less than 18 years; patients with significant brain injuries; in-patient psychiatric patients; and terminally ill patients. Patients were followed up at 12 months post programme attendance. All eligible patients admitted to the ICU were invited to join the programme. Data were collected between September 2014 and June 2015. Complementary data from the InS:PIRE programme has been published elsewhere (10–12).
Setting
InS:PIRE was undertaken at Glasgow Royal Infirmary (GRI), a large tertiary referral teaching hospital in Scotland. It has a 20-bedded general intensive care/high-dependency unit providing tertiary care for pancreatic, burn, oesophageal and plastic surgery. The hospital serves a community of severe socio-economic deprivation in the West of Scotland (13).
Intervention and measures
A musculoskeletal assessment was conducted by the physio-therapist (HD) during the 5-week programme (i.e. once during the 5-week period). Patients were asked during the musculoskeletal assessment to comment on any “new” pains since their admission to ICU, which had been present for more than 12 weeks. In the present study this was utilized to indicate the incidence of pain. The location of the patient’s pain was then coded by body site.
To understand the impact of pain following discharge from critical care, the Brief Pain Inventory (BPI) outcome measure was used at initial assessment of patients during the InS:PIRE programme and at a 1-year follow-up review (14). This measure was initially developed for patients with pain related to cancer; however, it has since been used in a wide range of patient groups with chronic diseases and conditions, including fibromyalgia, neuromuscular pain and post-surgical pain (15–17). The consensus panel Initiative on Methods, Measurement and Pain Assessment in Clinical Trials (IMMPACT) recommended that the 2 domains of the BPI be used in all chronic pain clinical trials (18). It allows patients to report their pain severity and interference with daily life. The BPI has been found to be a valid and reliable measure of chronic pain (19).
On the BPI, patients record the severity of their pain over the previous 24 h, as worst, least, mean and current pain, on a 0–10-point numerical rating scale (where 0 = no pain and 10 = worst pain imaginable). Developers of the tool recommend that all 4 items be used in a mean score (14). The optimal cut-off points for pain severity using the BPI are as follows: 0 = no pain, 1–3 = mild pain, 4–6 = moderate pain, and 7–10 = severe pain (20–21). Pain interference is measured using 7 components to include: general activity, mood, walking ability, normal work, relations with other people, sleep and enjoyment of life. Interference has been recommended by the tool developers to be scored as a mean of the 7 items (14). At 12 months all items in this study were compared with baseline values.
Analgesics used by patients for pain prior to ICU admission and at initial clinic attendance were recorded by the pharmacist (PMcT) within the InS:PIRE programme. The analgesics prescribed were then assessed according to the World Health Organization (WHO) pain ladder, a 3-step scale used by clinicians in the management of pain, which was originally developed for cancer pain in adults (22). The WHO pain ladder outlines the oral administration of pain-relieving drugs if pain occurs. It consists of: step 1: non-opioids (aspirin and paracetamol); step 2: mild opioids (codeine and tramadol); step 3: strong opioids, such as morphine. If pain occurs drugs should be prescribed in a stepwise order until the patient is free of pain. Additional drugs, called “adjuvants”, can also be added.
A number of patient demographics regarding the patient’s stay in the ICU were collected from the ICU database. Also collected was information about the patient’s socio-economic status. The Scottish Index of Multiple Deprivation (SIMD) is the Scottish Government’s tool for identifying socio-economically deprived neighbourhoods (13). For the purpose of this evaluation, the SIMD was split into quintiles; quintile 5 represents the most affluent area and quintile 1 represents the most deprived area.
Data analysis
Patient demographics were analysed using descriptive statistics and presented as numbers and percentages for the categorical variables (and medians and interquartile ranges) for the continuous variables.
Inferential statistics were explored using Minitab 17.3.1 Statistical Software (2016) (23). Means, rather than medians, were used in the analysis of the BPI pain intensity and interference scale, as recommended by the tool developers (14). Therefore, paired t-tests were used to compare initial and 1-year pain intensity and interference. An unadjusted modelling strategy utilizing binary logistic regression was undertaken to assess the predictive capacity of a number of variables on the likelihood that participants had “new” chronic pain after an ICU stay. Percentages were used to represent all other results.
Ethical considerations
InS:PIRE was a service improvement project utilizing quality improvement methodology within the ICU. Ethics approval was sought and waived by our hospital research and development department.
Patients
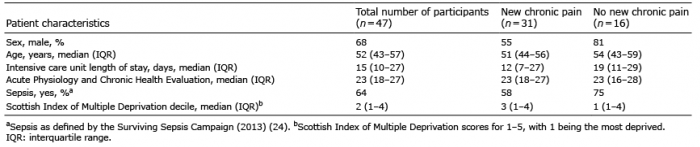
During this pilot study, 89 patients were invited to take part in InS:PIRE. Of these, 49 (55%) attended, and a final total of 47 patients received the physiotherapy assessment. Baseline demographics for the 47 patients are shown in Table I. The median age of participants was 52 years (interquartile range (IQR) 43–57 years), with a median Acute Physiologiy and Chronic Health Evaluation (APACHE II) of 23 (IQR 18–27). The largest group of patients came from a general medicine background (40%, n = 19), while 26% (n = 12) of patients came from general surgery and 11% (n = 5) from gastroenterology (Table II).
Table I. Patient demographics for the physiotherapy intervention group
Table II. Admitting speciality
Incidence and location of pain
At baseline assessment, two-thirds (66%, n = 31) of patients reported a “new” chronic pain since ICU admission at initial assessment (Table I). In these patients, lower limb pain was reported in over two-fifths of this group (42%, n = 13), but the shoulder joint was the most frequently affected joint (39%, n = 12), followed by the trunk/back (32%, n = 10), upper limb (6%, n = 2) and head (3%, n = 1) (Fig. 1). Thirty-nine percent of patients (n = 12) reporting a “new” chronic pain, had pain at more than one anatomical location/joint. Bilateral symptoms were reported in almost all of those who reported having lower limb pain (85%, n = 11), in contrast to only one-third of those with shoulder pain (33%, n = 4).
Fig. 1. Anatomical location of “new” chronic pain at baseline assessment.
Brief Pain Inventory intensity/severity
The mean BPI score for pain severity of those reporting a “new” chronic pain at initial assessment was 5.3 (standard deviation (SD) 2.4; range 0–10) and the mean score at 1 year was 4.6 (SD 2.7). The difference between reported pain severity at baseline and at 1-year was not significant (p = 0.66).
Brief Pain Inventory interference
The mean BPI score given by patients to describe the impact of pain on daily function or interference in those reporting chronic pain was 6.5 (SD 2.5). Pain interference decreased significantly between baseline assessment and follow-up at 1-year (mean 6.5 (SD 2.5) vs mean 4.5 (SD 2.7), respectively) (p = 0.04). Further investigation of pain interference on individual activities of daily living indicated that “enjoyment of life” (mean 7.1, SD 2.8) and sleep (mean 6.9, SD 3.3) were the most severely affected and “relations” the least affected by chronic pain (mean 5.7, SD 3.5) at baseline assessment. However, at 1 year “enjoyment of life” (mean 5.2, SD 3.2) and “normal work” (mean 5.2, SD 3.3) were the most affected.
Predictors
There was no significant difference in any of the variables, including ICU length of stay (LOS) , age, SIMD or sepsis, between those with and without chronic pain (Table III).
Brief Pain Inventory intensity/severity
The mean BPI score for pain severity of those reporting a “new” chronic pain at initial assessment was 5.3 (standard deviation (SD) 2.4; range 0–10) and the mean score at 1 year was 4.6 (SD 2.7). The difference between reported pain severity at baseline and at 1-year was not significant (p = 0.66).
Brief Pain Inventory interference
The mean BPI score given by patients to describe the impact of pain on daily function or interference in those reporting chronic pain was 6.5 (SD 2.5). Pain interference decreased significantly between baseline assessment and follow-up at 1-year (mean 6.5 (SD 2.5) vs mean 4.5 (SD 2.7), respectively) (p = 0.04). Further investigation of pain interference on individual activities of daily living indicated that “enjoyment of life” (mean 7.1, SD 2.8) and sleep (mean 6.9, SD 3.3) were the most severely affected and “relations” the least affected by chronic pain (mean 5.7, SD 3.5) at baseline assessment. However, at 1 year “enjoyment of life” (mean 5.2, SD 3.2) and “normal work” (mean 5.2, SD 3.3) were the most affected.
Predictors
There was no significant difference in any of the variables, including ICU length of stay (LOS) , age, SIMD or sepsis, between those with and without chronic pain (Table III).
Table III. Risk factors for the incidence of chronic pain: results of binary logistic regression analysis
Analgesics
The number of patients taking analgesics (steps 1–3 pain medications, as defined by the WHO pain ladder) prior to admission was 43% (n = 20). This figure had increased to 81% (n = 38) at the time of the patients’ baseline clinic visit. The intensity of analgesics prescribed also increased, with the number of patients prescribed strong opioids (step 3 of the WHO pain ladder) increasing from 2% (n = 1) to 11% (n = 5). Even with the increase in the number and potency of pain medications prescribed, two-thirds of patients still reported a “new” chronic pain (Table IV).
Table IV. World Health Organization (WHO) pain ladder analgesic use on intensive care unit (ICU) admission and at initial assessment
Healthcare support
This study found that over a quarter of patients (26%, n = 8) were already accessing physiotherapy treatment prior to their initial InS:PIRE attendance and a further 29% (n = 9) required referral after assessment to a specialist physiotherapist in areas such as the shoulder or back. A number of patients required referral to local gym schemes (19%, n = 6) to increase fitness and body strength, or onward referral to other services, such as their primary care physician (19%, n = 6).
This is one of the first studies internationally to explore pain intensity and interference in ICU survivors. Two-thirds of patients in this study reported a “new” chronic pain when attending an ICU follow-up programme. This chronic pain was of “moderate” intensity and was reported to be directly related to the ICU admission. The shoulder was the single most affected joint in this study, with almost two-fifths of patients reporting this problem. No significant predictors for chronic pain were found. Chronic pain resulted in a high level of interference in patients’ daily activities after discharge from the ICU, with “enjoyment of life” and “sleep” being the most severely affected at initial programme attendance. It was also found that patients who have had an ICU admission frequently needed pain medication for a “new” chronic pain after discharge from the ICU. Furthermore, there appeared to be a need for more potent analgesics following discharge from the ICU. Pain interference, but not pain severity, improved over the 1-year period, with “enjoyment of life” and “work” now being the most affected.
The incidence of chronic pain in this study is consistent with a previous study in ICU survivors, which highlighted that up to 73% of patients reported chronic pain at 12 months post-ICU discharge (3). Similarly, another study reported that 56% of patients had chronic pain at 2 years post-discharge (25). This incidence of chronic pain is higher than the European population norm, which suggests that that 20% of people live with chronic pain (26). The incidence of shoulder pain in this study is almost double that of findings in another study which found that over 20% of patients had shoulder pain post-ICU (9). The shoulder is a vulnerable joint; the strategies employed to move patients in the ICU often depend on pressure being placed on this joint. This may be a cause of this new pain; however, more information and research in this area is required.
The literature suggests that the causes of chronic pain post-ICU are multifactorial. The severity of patient’s illness in the ICU necessitates certain procedures, which often cause pain/discomfort and prolonged periods of immobilization, in addition to the critical illness process (7). No significant predictors for chronic pain were found in this population. However, ensuring early mobility and appropriate physical therapy within the hospital setting may help prevent some of the issues seen in this cohort of patients. At present the literature has focussed on functional capacity as an outcome measure for interventional rehabilitation research in this area. Future research must also understand the potential impact of these interventions for pain development in this group.
In relation to the requirement for analgesics, there is a dearth of literature on the pharmacological management of chronic pain in ICU survivors after hospital discharge and the associated cost. This is probably due to the lack of involvement of pharmacists in post-ICU follow-up clinics (27). It is important that future studies address this issue to ensure that patients are receiving safe, effective care.
Strengths of this evaluation include its systematic approach to assessing pain in critically ill patients attending an ICU recovery programme. Furthermore, this is one of the first studies to apply a standardized tool to help understand analgesic requirements in this population. However, this study has several limitations. Pain interference, but not pain severity, improved over time; this may be due to improved psychological status and the development of coping strategies to manage pain over time. It is unclear whether this improvement is correlated with self-efficacy and the amelioration of psychological problems, such as anxiety and depression. These data were not available for analysis in the present evaluation, but future research should explore psychological profiles with chronic pain. The definition of chronic pain utilized in this study, was pain which persisted for more 12 weeks. There are a number of different definitions of chronic pain in the literature and this may limited the scope of the findings of this study. Furthermore, this study took place in a single centre with a small population. ICU survivors are at a high risk of developing chronic pain. This study did not have a pre-defined sample size and was a sample of convenience, thus may not have detected relationships between variables.
In conclusion, the findings of this small-scale quality improvement project suggest that post-ICU follow-up programmes should provide the appropriate support to manage chronic pain issues. Future large-scale, multi-site research related to post-ICU chronic pain is required to understand this problem further and to help design appropriate, effective interventions for patients.
This work was supported by a Health Foundation Shine Award (2014). The Health Foundation is a charitable organization.
Joanne McPeake was supported by a Chief Nursing Officer (Scotland) Fellowship for the duration of this study. Joanne McPeake and Tara Quasim are supported by grants from the Society of Critical Care Medicine.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize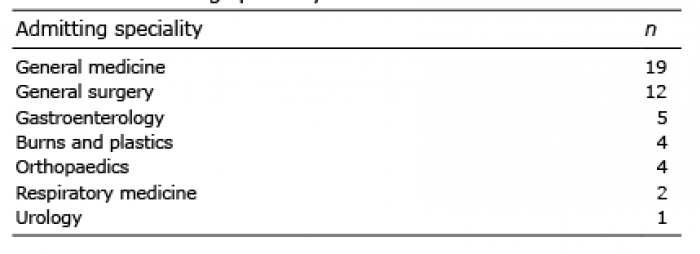 Click to show fullsize
Click to show fullsize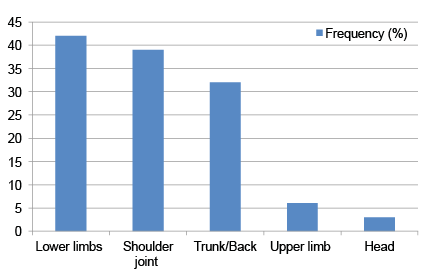 Click to show fullsize
Click to show fullsize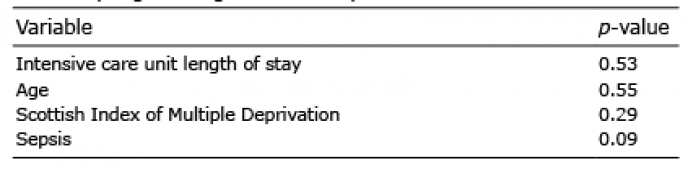 Click to show fullsize
Click to show fullsize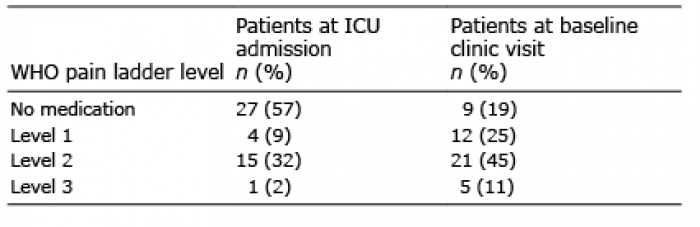 Click to show fullsize
Click to show fullsize