
From the 1Department of Physiotherapy and Occupational Therapy, Aarhus University Hospital, Aarhus C, 2The Research Initiative of Activity Studies and Occupational Therapy, Research Unit of General Practice, Department of Public Health, University of Southern Denmark, Odense, 3Danish Rheumatism Association, Gentofte, 4Section of Social Medicine and Rehabilitation, Department of Public Health, Aarhus University, Aarhus C and 5Research Department, Spine Centre of Southern Denmark, Lillebaelt Hospital, Institute of Regional Health Services Research, University of Southern Denmark, Middelfart, Denmark
Objective: To evaluate the effect of adding a lay-tutor to the educational sessions of a back school programme for patients with subacute low back pain.
Methods: Patients with subacute low back pain were randomized to a 10-week programme comprising 10 h
education and 20 h physical exercise led by a former patient as lay-tutor, or a programme led by a physiotherapist. In the intervention group, former patients served as lay-tutors in the educational sessions, teaching in conjunction with physiotherapists. In the control group, 2 physiotherapists led the entire educational programme. Disability, back pain, leg pain and health status were evaluated blindly at 3 and 24 months.
Results: Eighty-seven patients with subacute low back pain referred for treatment at 6 selected physiotherapy clinics were allocated to either an intervention group (n = 42) or a control group (n = 45). No statistically significant difference was found between the 2 groups. Both groups of patients showed a statistically significant improvement in health and pain measurements from the start of the study to the 3- and 24-month follow-up.
Conclusion: No short- or long-term effect was found of adding a lay-tutor to the educational sessions of a back school programme for patients with subacute low back pain with regards to functional activity, back pain, leg pain or general health. The main limitations are that the potential effect of including lay-tutors in the educational part of a back school programme as an intervention in itself has to be tested, and the programme has to be tested as a complete protocol. Also, no specific testing has been performed to confirm the ideal number of sessions in the programme.
Key words: subacute low back pain; lay-tutor; patient education; self-care; self-management.
Accepted Jul 5, 2019; Epub ahead of print Aug 14, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Berit Schiøttz-Christensen, Research Department, Spine Centre of Southern Denmark, Lillebaelt Hospital, Institute of Regional Health Services Research, University of Southern Denmark, DK-5500 Middelfart, Denmark. E-mail: Berit.Schiottz-Christensen@rsyd.dk
National and international guidelines recommend group exercise programmes for patients with specific or non-specific low back pain. This includes advice and information tailored to the patients’ needs and capabilities in order to help them self-manage their back pain. Eighty-seven patients with subacute low back pain were allocated to a 10-week programme comprising 10 h of education and 20 h of physical exercise. In the intervention group (42 patients), the educational part was led by a lay-tutor. In the control group (45 patients), the educational part was led by physiotherapists. Compared with patients in the educational sessions led by physiotherapists, patients in those led by lay-tutors did not show more improved health and pain measurements at 3 and 24 months follow-up after the start of the study. In conclusion, adding a lay-tutor to the educational sessions of a back school programme for subacute low back pain patients did not change the outcome at short- and long-term follow-up.
National and international guidelines recommend group exercise programmes for patients with specific or non-specific low back pain (1, 2). This includes the provision of advice and information tailored to the patients’ needs and capabilities in order to help them self-manage their back pain (3).
In Denmark, back school programmes (BSP) are typically offered within the primary healthcare sector. The programmes include a combination of physical exercises and education and are usually led by healthcare professionals. Education, aiming to equip the patients with adequate knowledge and skills to better manage their health-related problems, is included in the most recent programmes (4). By increasing the patients’ knowledge and skills, the educational part of the back school aims to support a patient’s motivation to change their health-related behaviour and to strengthen their ability to self-manage their back pain (5). It has been proposed that the inclusion of a lay-person as a facilitator might increase short- and long-term self-efficacy and self-management among patients with chronic conditions (5).
Lorig et al. has explored the use of patients, who had experienced effective pain relief through self-management of their own condition, as role models (6, 7). These studies showed that role models invited to educational programmes as active partners might encourage and motivate participants in BSPs. Other lay-led programmes, such as the Arthritis Self-Management Programme (ASMP) for patients with chronic disease (8), support this observation. Therefore, we designed a programme that included lay-persons as tutors for patients with low back pain. To our knowledge, no studies have evaluated the long-term effects of using lay-tutors as active partners in a BSP, comparing them with similar programmes led by healthcare professionals (5).
The aim of the present randomized controlled clinical trial (RCT) was to evaluate the effect of adding a lay-tutor to the educational sessions of a BSP for patients with subacute low back pain (SLBPP). It was hypothesized that patients whose education was facilitated by lay-tutors would be more motivated to stay active despite pain and to perform activities of daily living, thereby showing better improvement in functional capacity, pain and health-related outcomes than patients taught solely by healthcare professionals.
Design
This RCT was conducted in collaboration with the rehabilitation unit “SANO”, local physiotherapy clinics, the Section of Social Medicine and Rehabilitation and the university rheumatology clinic, in order to determine effective educational and exercise programmes. Fig. 1 shows the patient flow through recruitment, intervention and follow-up.
Back school programme
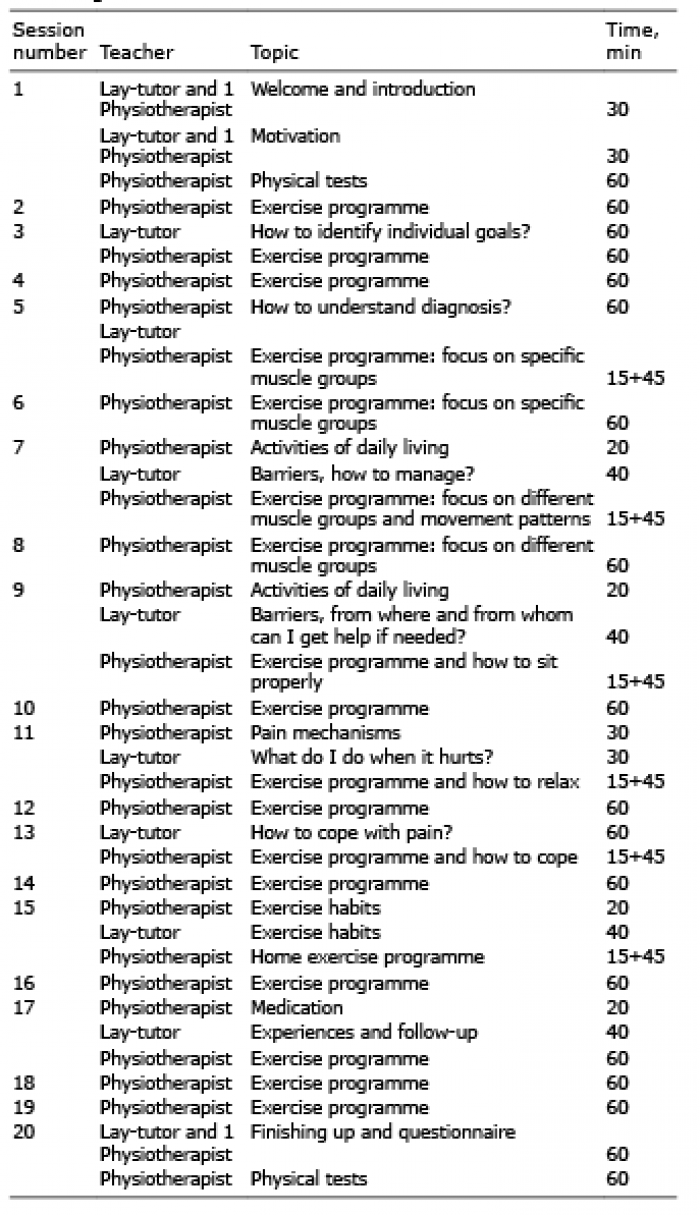
Experimental set-up. The BSP was based on self-management strategies, with the goal of motivating the participants to stay active and to change their health-related behaviour. The programme consisted of 2 sessions each week for a 10-week period, a total of 20 sessions (Table I). Once a week, the patients participated in a 2-h session with 1 h of education and 1 h of physical exercises. The other weekly session included only 1 h of physical exercises.
Table I. Procedures during a 10-week intervention programme including 10 sessions of education and 20 sessions of exercise
Educational part of the programme. This part consisted of providing information related to the condition of the patients. It included disease-specific information on anatomy, pain physiology and ergonomics. General information included how to cope with back pain in everyday life and provided examples of how to change bad habits and develop pain-coping strategies. The patients were encouraged to set personal goals as an important component in promoting self-management.
In the intervention group, the lay-tutor was responsible for general information (40 min) and the physiotherapist for disease-specific information (20 min). In the control group, 2 physiotherapists covered the entire lesson.
Physical exercise part of the programme. Each exercise session included aerobic training and exercise, focusing on strength, stability, coordination, balance, flexibility and relaxation. The sessions were group-based, but were adjusted to accommodate the individual patient. During each session, the participants were encouraged to take responsibility for their own progression through the programme, while the physiotherapists gave exercise instruction, feedback, and acted as motivators. At the end of the programme, all patients had an individualized physical exercise plan to follow.
Prior to the study, a detailed manual was developed for both the educational and the physical exercise components in order to standardize the BSP. All lay-tutors and physiotherapists participated in a 2-day introductory course led by clinical experts in the field of low back rehabilitation. In addition, the physiotherapists attended a 1-day course focused on the exercise lessons. A Danish version of the manual is available on request from the corresponding author.
Intervention. The intervention represented the participation of the lay-tutor in the educational part of the BSP. The lay-tutors were former back pain patients who shared their own experiences and focused on how they coped with their episodes of low back pain. Such interventions were expected to encourage patients to overcome pain-related problems in daily activities, and allow them to cope with their pain, as measured by improvement in general health. Since patients might be motivated by and relate more to the lay-person than to the physiotherapist, we expected the intervention group to improve functional capacity, pain and health outcomes compared with the control group.
Lay-tutors, physiotherapists and setting
Lay-tutors. The 6 lay-tutors were recruited among former patients at the participating physiotherapy clinics or at the outpatient clinic at the university hospital. Selection criteria for lay-tutors were: previous back pain patient, no prior back surgery, employed, age range 30–60 years, positive attitude to life, and ability to stay active despite back pain.
Physiotherapists. Participating physiotherapists were willing to teach with the lay-tutors, and they had a minimum of 2 years of documented experience in the rehabilitation of patients with back problems. Furthermore, they were committed to the back school concept as presented in the introduction course. No lay-tutor or physiotherapist was replaced during the study.
Setting. Six physiotherapy clinics in one of the largest cities in Denmark hosted 12 groups in total (2 groups each), with 6–8 participants in each group (October 2004–April 2005).
Physiotherapy clinics in Denmark are privately operated, but publicly funded. Selection criteria for inclusion of the physiotherapy clinics were: accessibility to facilities for education and physical exercise. Requisite equipment included bikes, steppers, trampolines, pulldown equipment, a backbench, dumbbells (1–8 kg), exercise balls, and facilities for educational sessions.
Patients
Inclusion criteria. Non-specific low back pain with a current duration of 4–12 weeks at time of referral, age range 30–60 years, employed or available for work, and able to participate in the educational sessions and answer the questionnaires at inclusion and during follow-up.
Exclusion criteria. Surgery referral, previous back surgery, pronounced osteoporosis, systemic chronic disease, pregnancy and inability to speak and understand Danish. The criteria were chosen in order to recruit a relatively homogenous group of patients.
Patients were invited to participate in the study by general practitioners and specialists and they received both oral and written information about the study. All participants accepted for participation in the study signed a written consent form and were allocated by computer-based randomization (1:1) to either the intervention group or the control group.
Outcome measures
The primary outcome measure was data from the Roland Morris Questionnaire (RMQ), measuring function in daily activities (9). The RMQ was chosen because it was developed to be used to evaluate functioning in patients with low back pain in the primary care setting and has shown to be valid in a setting like the one presented. The questionnaire is easy to answer, but is limited in the domains covered (9). The secondary outcome was the Short Form 36 Health Survey (SF-36) measuring general health using composite scores, the mental component score and the physical component score (10). In addition, 2 sub-scores were used: the physical function score and general health score. Finally, the patients were asked to describe their back pain and leg pain, as current pain and the worst pain during the past 2 weeks on a 0–10 numerical rating scale (NRS). The questionnaires were given to participants together with a pre-paid postage envelope at the beginning of the study (during the first session) and at 6 weeks, 3 months and 2 years after finishing the BSP.
Randomization
In order to ensure comparability between the groups with and without lay-tutors, the patients were randomly distributed. The allocation was handled by a secretary from a pre-ordered (third party) numbered list. Subsequently, the secretary contacted the clinic associated with the chosen programme and provided them with the patient’s name and telephone number. The clinic then informed the patient about the randomization result (control/intervention) and practical details related to the BSP.
The randomization protocol was drafted by a third party based on a computer program, and it was unavailable to the project manager.
Statistical analysis and power calculations
A power calculation was performed based on the RMQ. The standard deviation (SD) was set to 5.9 points. The minimal clinically important difference estimate was 4.5 RMQ points (11). With a power of 80% and a 2-sided significance level of 0.05, a total of 54 patients (27 in each group) was needed. In order to account for a 20% loss to follow-up, at least 65 patients needed to be included in the study. A total of 87 patients, referred by general practitioners (90%) and rheumatologists (10%), were included.
Data were entered twice into Epidata3.2 and any divergence was corrected by reference to the original material. STATA®14 software was used for statistical evaluation. The risk of a type 1 error was set to 5%. The data were analysed according to the intention-to-treat principle. To compare the 2 groups, we used a mixed model for repeated measurements with an unstructured covariance matrix to test the effect on RMQ, back pain, leg pain and SF-36 data. In order to do this, we used the Kenward-Rogers approximation to obtain the degrees of freedom for the tests in spite of missing values (12). Examining the residuals and fitted values did not give any cause to doubt the assumptions behind the model.
Ethical aspects
Patient information and letters of consent were set up in accordance with recommendations of the Central Denmark Region Committees on Health Research Ethics. The committee concluded that the project did not require review. The Danish Data Protection Agency approved the project (file number 1-16-02-588-15).
A total of 117 patients met the inclusion criteria and were invited to participate in the study; 30 patients declined the invitation (Fig. 1). In total, 87 patients gave their written informed consent to participate and were enrolled in the study. Eighty-two patients (94%) completed the questionnaire at the 3-month follow-up, and 73 patients (84%) responded at the 24-month follow-up (Fig. 1). Similar dropouts occurred for both study groups with regard to age and sex.
Fig. 1. Recruitment and participation in the study.
Table II presents the baseline characteristics of the participants. Overall, the 2 groups were comparable in terms of baseline characteristics, including demographic characteristics, employment status, duration of pain, number of back episodes and sick leave. The 2 groups were also comparable at baseline in terms of the different outcome measures, RMQ, back pain, leg pain and SF-36 (Table III).
Table II. Baseline characteristics of 87 patients included in the study
Table III. Data on disability measured by Roland Morris Questionnaire, back pain, leg pain and general health (measured by Short Form 36 Health Survey (SF-36)) for the intervention group and the control group at all measurement times. Data are described by mean and 95% confidence intervals (95% CI). The overall between-group effects are analysed based on the intention to treat principle in a mixed effect model for repeated measurements with group and time as systematic factors and patients as random effects
With regard to the primary outcome measure, the RMQ scores for functional activity, the mean score at baseline was 10 (95% confidence interval (95% CI) 8; 12) in the intervention group and 9 (95% CI 9; 11) in the control group, on a 0–24-point scale, where 0 represented no disability. No statistically significant between-group effect was found over time (Table III). As shown in Table III, small and statistically insignificant between-group differences were found over time when comparing the secondary outcome measures, back pain, leg pain and general health (SF-36).
Participants in the 2 groups showed similar attendance at the back school sessions. Out of the 20 back school sessions, the median number of sessions attended by participants was 17 (25th–75th percentile 15; 19) in the intervention group and 17 (25th–75th percentile 14; 19) in the control group.
This RCT aimed to evaluate the long-term effect of adding lay-tutors to the educational sessions of a BSP for SLBPP treated in a primary care setting. Participation of former back pain patients as lay-tutors in a BSP was expected to inspire SLBPP to change their health-related behaviour, thereby improving their physical function and health status. However, this turned out not to be the case; no differences were found regarding any of the outcomes between the 2 groups.
The current study was planned and conducted more than 10 years ago, but is still a highly relevant concept used in Denmark and other Western countries. At the time the study was initiated, the treatment of patients with low back pain changed to a more individualized concept. However, the back school concept has now been reintroduced in the Danish primary sector, focusing on education and individualized exercise. This study brings knowledge to the discussion about whether lay-tutors should be included in BSPs (1).
Poquet et al. (13) have stated that the back school concept is not efficient for patients with acute and subacute back pain, in contrast to Sahin et al., who, among patients with chronic low back pain, found an effect of adding the back school concept to exercise and physical treatment (14). This might be the case if the programme focused on group-based programmes, but differentiated programmes may be more effective. This study showed that patients had better outcomes in long-term follow-up; however, the introduction of lay-tutors to the educational part of the whole programme was ineffective.
Whether lay-tutor programmes, by themselves, might have the same effect as the combination of education and exercise in the same programme has to be tested in another setting.
The BSP was planned in collaboration with experienced physiotherapists and occupational therapists working in programmes including self-management strategies for patients with low back pain (Table I). These programmes were based on the theory of Bandura (15, 16), and are well described in a comprehensive manual. The protocol comprised a structured programme and theoretical information, as well as schedules for each exercise session. The manual was used in the training period by both physiotherapists and lay-tutors to ensure consistent knowledge and guidance. As we explored the effect of adding a lay-tutor to the BSP it was developed by clinicians for this specific project; therefore, we did not evaluate the effect of each of the learning sessions. This should be done if the protocol is used in future projects. The manual was written in Danish, due to the Danish setting of the study.
Previous studies, including lay-led programmes on coping and self-help strategies in handling chronic low back pain in everyday life, describe changes in coping strategies (5). The current study evaluated to what extent the participation of a lay-tutor affected long-term functional outcome and general health status, but did not evaluate the effect of the participation of a lay-tutor on individual competencies to handle daily activities despite back pain. This focus could be included as an outcome in future projects. In addition, including the lay-tutor in the educational programme and in the assessment of the patient’s ability to cope is also recommended (17).
Methodological considerations
The RMQ was used as the primary outcome. Mean RMQ was 10 out of 24, and the pain score was 4 out of 10, which was in accordance with other subacute low back pain populations treated in primary care (9), but compared with studies evaluating programmes including chronic back pain patients the score is relatively low (18). As minimal clinical important change in the RMQ score we used 4.2, which is higher than recommended by Roland (9). It is stated that a change of 1–2 points in a setting such as the one presented might be relevant. The relative change could have been used as an outcome, but it is seldom used in back pain studies and it was not chosen as an outcome in this study.
Strengths
To strengthen the generalizability of the study, patients were recruited from general practice and in an outpatient clinic at the university hospital. This strengthened the recruitment of patients and the external validity of the findings.
The patients fulfilled the inclusion criteria, representing a group of patients with subacute low back pain, of which two-thirds reported previous episodes of back pain. The mean age was 47 years, and they were employed, two-thirds as white collar or public servants. This group of patients were representative of the patients seen in a private physiotherapy clinic. They did not represent the group of patients with chronic low back who are usually the focus of the interventions described in this study. The eventual effect of including lay-tutors in the programme including chronic patients should be tested if it is planned for lay-tutors to be part of these programmes.
The high compliance with the interventions was considered another strength of the study, indicating that the patients were motivated and participated actively in most sessions.
Limitations
The main limitation of this study is that it did not explore the overall effect of BSPs including lay-tutors by including a control group not receiving the BSP. As the BSPs were part of usual practice at the time of the study, we aimed to explore the effect of adding lay-tutors to a BSP. Thus, the potential effect of including lay-tutors in the educational part of a BSP as an intervention in itself was not explored.
Another limitation was that 23 participants (26%) were lost to follow-up at 24 months. However, with the inclusion of 87 patients, a loss to follow-up of 26% is acceptable in accordance with the power calculation. In the analysis, a mixed model accounting for missing values was used. In the presence of missing data, the mixed model is considered an efficient use of the data at hand (12).
Previous studies on rheumatoid arthritis and on chronic pain conditions have shown an effect of inclusion of lay-persons in educational programmes (5). In the current study it was hypothesized that a similar response could be obtained in the current study population. However, the previous studies focused on patients with chronic pain and the patients in the current study were SLBPPs (17). As such, coping strategies with pain and their expectations towards functional ability in daily life might be different, and this might affect how they incorporate the information provided by lay-tutors. This may have been a reason for not finding the hypothesized effect of lay-tutors on our group of SLBPPs. A newly published study by Mehlsena et al. regarding lay-tutors also reported no effect of a lay-led group-based self-management programme for patients with chronic pain (19).
The inclusion of a lay-person in the team performing the intervention required that the lay-person had personal skills and the desire to act as a teacher. Furthermore, the lay-person needed to be able to understand the theory behind the programme and the teaching resources. Finding people who meet these requirements can be difficult, and requires ongoing supervision by trained healthcare providers. The cost of inviting a lay-person as a teacher is expected to be low, as it represents volunteer work. If lay-tutors need to be paid, there will be no financial benefit from such an effort. The specific skills of each of the lay-tutors have not been tested in this setting, which has to be done if the programme is conceptualized.
The schedule for the programme, including 1 h of teaching and 1 h of training every second time, was decided by the clinicians. Whether this is the strongest concept is not tested in this setting. If the dose response relation is an issue a dose response study will be needed.
Clinical implications and implications for future research
The aim of this study was to specifically evaluate the effect of adding lay-tutors to the educational sessions of a BSP for patients with low back pain. Therefore, an RCT design was used, which was considered to be optimal for comparing the effectiveness of 2 interventions. The programme included both educational and exercise sessions for all patients. All patients participated in an individually adjusted exercise programme in accordance with the protocol. The study focused on the potential effect of using a lay-person as 1 of 2 teachers in the educational sessions. It did not focus on the potential positive effect of the individualized guidance by the physiotherapist during the exercise programme. Optimally, an extra control group that did not receive any of the elements of the back school intervention could have been included; this was not considered as an option while information is known to be the foundation of guidance for back pain patients. Another option, which is recommended for further investigations, would be to focus on change in coping strategies.
Conclusion
No short- or long-term effects were found of adding a lay-tutor to the educational sessions of a BSP for patients with subacute low back pain, with regards to functional activity, back pain, leg pain or general health. The main limitations of this study are that: the potential effect of including lay-tutors in the educational part of a BSP as an intervention in itself has not been tested; the programme as a whole protocol should be tested; and no specific testing was done to secure the ideal number of sessions in the programme. These issues should be addressed in another setting.
The project was supported by the Danish Rheumatism Association in collaboration with the Association of Danish Physiotherapists and the Municipality of Aarhus, Denmark.
Funding. This work was financially supported by the Danish Ministry of Health and conducted as part of the Danish national health promotion programme: “Healthy Through Life” [2003-1432-5].


 Click to show fullsize
Click to show fullsize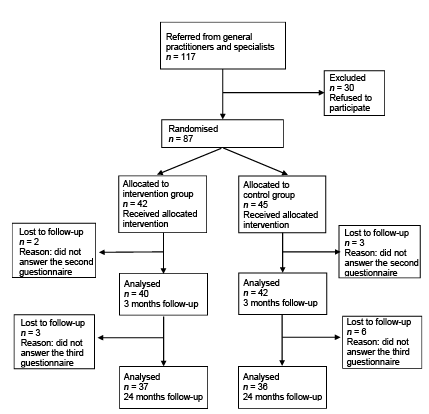 Click to show fullsize
Click to show fullsize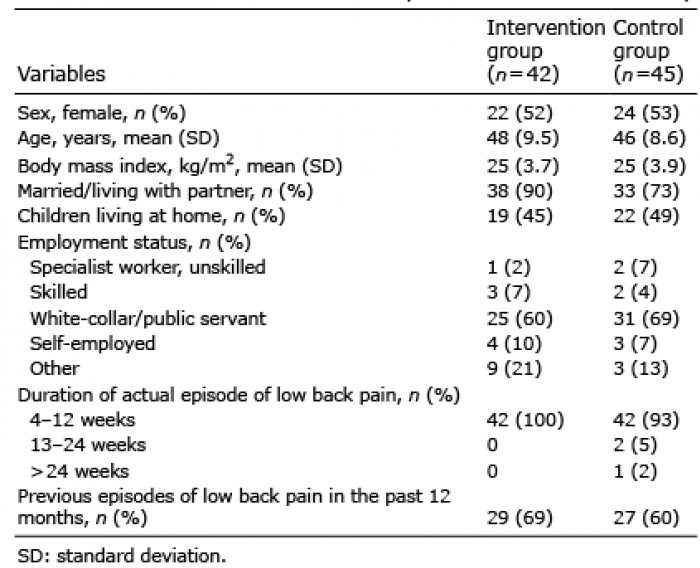 Click to show fullsize
Click to show fullsize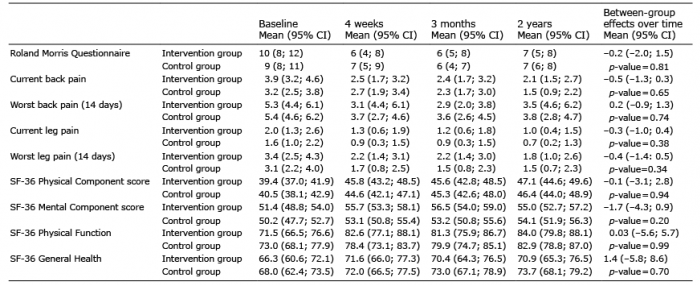 Click to show fullsize
Click to show fullsize