
From the 1Department of Nursing Science and Research Center for Habilitation and Rehabilitation Services and Models (CHARM), Faculty of Medicine, University of Oslo, 2Department of Geriatric Medicine, Oslo University Hospital, 3Oslo Centre for Biostatistics and Epidemiology, Department of Biostatistics, Faculty of Medicine, University of Oslo, 4Department of Nursing and Health Sciences, Faculty of Social and Health Sciences, Inland Norway University of Applied Sciences, 5Department of Health and Care Sciences, Faculty of Health Sciences, UIT, The Arctic University of Norway, 6Department of Geriatric Medicine, Oslo University Hospital, 7Department of Neurology, Akershus University Hospital and 8Department of Geriatric Medicine and Physical Medicine and Rehabilitation, Oslo University Hospital, Faculty of Health Sciences, Oslo Metropolitan University, Oslo, Norway
Objective: To evaluate the effect of a dialogue-based intervention on psychosocial well-being 6 months after stroke.
Design: Multicentre, prospective, randomized controlled trial.
Subjects: Adults (aged ≥ 18 years) who had their first or recurrent stroke within the last month, were medically stable, had sufficient cognitive functioning to participate and understood and spoke Norwegian.
Methods: A total of 322 participants were randomly assigned to the intervention (n = 166) or control (n = 156) group. Participants in the intervention group received up to 8 individual sessions aimed at supporting the coping and life skills of stroke survivors in addition to usual care. The primary outcome was the proportion of participants with normal mood measured by the General Health Questionnaire-28 (GHQ-28). The secondary outcomes included health-related quality of life (Stroke and Aphasia Quality of Life Scale; SAQOL-39g), depression (Yale-Brown single-item questionnaire; Yale) and sense of coherence (SOC-13).
Results: After controlling for the baseline values, no significant benefit was found in the intervention group over the control group (odds ratio (OR): 0.898: 95% confidence interval (95% CI): 0.54-1.50, p = 0.680) 6 months post-stroke.
Conclusion: Psychosocial well-being improved during
the first 6 months after stroke in both arms of the trial, but no statistically significant benefit of the dialogue-based intervention was found compared with usual care.
Key words: psychosocial rehabilitation; stroke; intervention study; mood; psychosocial factor.
Accepted Jul 8, 2019; Epub ahead of print Aug 14, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Ellen Gabrielsen Hjelle, Department of Nursing Science, Faculty of Medicine, University of Oslo, Pb 1130 Blindern, NO-0318 Oslo, Norway. E-mail: e.g.hjelle@medisin.uio.no
The aim of this study was to evaluate the effect of a dialogue-based intervention on psychosocial well-being 6 months after stroke. A total of 322 participants were assigned to an intervention (n = 166) or control (n = 156) group. Participants in the intervention group received up to 8 individual sessions aimed at supporting the coping and life skills of stroke survivors in addition to usual care. Psychosocial well-being improved during the first 6 months after the stroke in both arms of the trial. However, no benefit of the dialogue-based intervention was found compared with usual care.
Stroke is a major cause of death and disability globally and imposes social and economic burdens on individuals, families and communities (1). Every year, approximately 12,000 people suffer from stroke in Norway (2). Psychosocial challenges and emotional symptoms are frequent sequelae after stroke. Approximately one-third of patients report depressive symptoms (3) or anxiety (4) the first year post-stroke. Other common challenges include general psychological distress and social isolation (5). Psychosocial problems affect long-term functioning and health-related quality of life as well as motivation to participate in rehabilitation, but follow-up targeting psychosocial adjustment may improve psychosocial well-being, independent of functional impairment after stroke (6). To promote well-being, prevent additional negative consequences after stroke, and maximize the effect of rehabilitation, psychosocial well-being should be a focus during post-stroke care.
Systematic reviews have explored psychosocial interventions after stroke (3, 7–10). Although motivational interviewing is the only intervention with a documented effect (7), providing information (10), counselling (9) and liaisons with services (8) may contribute to psychosocial well-being. A study on motivational interviewing found a statistically significant benefit over usual stroke care. The results suggested that motivational interviewing led to improvements in the patients’ mood 3 months after stroke, and the benefit was confirmed at 12 months (11).
However, few dialogue-based psychosocial interventions to support stroke survivors’ coping and life skills have been conducted by primary healthcare professionals in the municipalities. In Norway, implementation of the Coordination Reform in 2012 (12) resulted in a shift in focus from primarily treating patients in hospitals to a focus on prevention, improving coordination between different care levels, integrating care in the community, and strengthening healthcare in the municipalities. The overriding aim of the reform was to direct more investment towards primary care in order to curb increasing hospital expenditure. As part of this shift, providing rehabilitation near patients’ homes in the municipalities was encouraged.
The dialogue-based intervention was developed and feasibility tested in accordance with the United Kingdom Medical Research Council (UK MRC) guidance on developing and evaluating complex interventions (13, 14). The intervention was found to be feasible to conduct in the municipalities, was tailored for stroke survivors and designed to be delivered in the early rehabilitation phase starting 4–6 weeks after stroke onset (15). A guiding topical outline and worksheets were developed to support the dialogues. The topics included emotions, social relationships, bodily changes, dynamic problem-solving, daily activities and identity (14, 15).
The theoretical perspectives underpinning the intervention included Antonovsky’s (16) theory on salutogenesis, sense of coherence (SOC), narrative theory (17) and ideas from guided self-determination (18).
Based on the theoretical foundation and feasibility work, we hypothesized that support during the early adjustment phase following a stroke could lead to improvements in mood, reduced depression, enhanced health-related quality of life and improved understanding, manageability and meaning in their lives after stroke (14, 15).
The present study evaluated the effect of a dialogue-based intervention in addition to usual care on psychosocial well-being 6 months after stroke.
Trial design and participants
This study was a multicentre, prospective, randomized controlled trial (RCT). Participants were recruited from 11 acute stroke or rehabilitation units in eastern Norway between November 2014 and November 2016.
Patients who met these criteria were invited to participate: aged >18 years and had had an acute stroke within the past month, were medically stable, had sufficient cognitive functioning to provide informed consent and participate, and understood and spoke Norwegian. Exclusion criteria were: severe dementia, other serious somatic or psychiatric diseases or severe aphasia. Recruiting personnel assessed the cognitive function and aphasia, which were discussed with the rehabilitation team at the recruiting institutions.
Interventions
All participants received usual care. Usual care included acute treatment at stroke units and rehabilitation centres or in the municipality. All participants were followed up by their physicians in accordance with the Norwegian clinical guidelines for treatment and rehabilitation after stroke (19) in addition to nursing and therapy input (e.g. through a multidisciplinary team) based on need and availability.
The dialogue-based intervention consisted of 8 individual sessions involving the participant and a registered nurse (RN) or occupational therapist (OT) recruited via the recruiting institutions, other stroke rehabilitation units or the community healthcare. All intervention personnel (IP) were required to complete a 3-day training programme. Group seminars led by members of the research team were arranged for the IP during the study. The seminars were an arena for guidance and supervision and allowed the research team to reinforce IP training and compliance to protocol in order to promote intervention fidelity.
The same RN/OT worked with the participant through all sessions. Interventions were delivered mainly in the participants’ homes. The first of the 8 sessions began shortly after randomization (4–8 weeks post-stroke), and the final session was completed within 6 months. The number of sessions was chosen to balance the ideal with the realistic (i.e. as few encounters as possible, but enough to provide adequate support).
The sessions` content addressed feelings, thoughts and reflections related to the patients’ experiences after stroke, and were based on topics highlighted as significant issues in the stroke literature and in the development and feasibility studies (14, 15).
Theoretically, experiences of chaos and a lack of control were perceived as potential threats to well-being following stroke. It was assumed that sense of coherence (SOC) could be promoted by experiencing diverse life events as comprehensible, manageable and meaningful. To promote SOC, the participants were encouraged to relate their experiences. Narrative theories em-phasize that human beings create meaning in their lives through telling stories. By guided self-determination, the intervention sought to empower the participants to make decisions on issues related to well-being based on their values and perspectives (14).
More details on the topics of the dialogue-based sessions are provided in the Table SI and Table SII1. Further details regarding the development and adjustments of the intervention were provided in previous research (15).
Outcomes
The stroke aetiology, side localization of the stroke symptoms, cognitive function, and language difficulties were recorded at baseline after obtaining informed consent. Neurological deficits were evaluated using the National Institutes of Health Stroke Scale (NIHSS) upon admittance to the hospitals (20). Information regarding cognitive function (Mini Mental Status Evaluation; MMSE) was collected from the participant’s medical record.
Participants were assessed prior to randomization using structured outcome measures 1 month post-stroke (T1). In addition, the data collector recorded the patient’s age, sex, living situation, education, work status, caring responsibilities, social support, previous illnesses and rehabilitation services. Data collectors with healthcare backgrounds (RN or OT) administered the instruments using a personal interview format. The assessors read the questions to the respondent and recorded the respondent’s answers in a web-based secure questionnaire using a tablet. At 6 months post-stroke (T2), a data collector who was blinded to the group allocation repeated the outcome measurements. Any changes in the patient’s living situation or health status since the first assessment were recorded.
The term psychosocial refers to the interrelation between social factors and individual thoughts and behaviours. Well-being generally refers to emotional reactions and subjective evaluations in response to events and includes a greater prevalence of positive than negative emotions and moods, satisfaction with life, sense of fulfilment, and positive relationships (21, 22). The primary outcome to evaluate psychosocial well-being was the General Health Questionnaire-28 (GHQ-28) (23). The GHQ-28 has been translated into Norwegian (24) and evaluated as an appropriate tool for research purposes in studies to capture emotional stress (25). The GHQ-28 consists of the following 4 subscales addressing aspects of psychosocial well-being: somatic symptoms, anxiety and insomnia, social dysfunction and severe depression (23). Higher score on the GHQ-28 indicates higher distress levels. The continuous GHQ-28 score was calculated based on a Likert scoring of 0, 1, 2, 3, resulting in a scale of 0–84. The dichotomized GHQ-28 score was based on a case scoring of 0, 0, 1, 1, resulting in a scale of 0–28. Based on a comparable study (11) the cut-off was set at 5 in the dichotomized GHQ-28 variable. Scores <5 indicated a normal mood, and scores ≥5 indicated a low mood.
Three secondary outcomes were explored. The Yale-Brown single-item questionnaire (Yale) measures the individual’s presence or absence of depression (26). The Stroke and Aphasia Quality of Life Scale-39 (SAQOL-39g) addresses dimensions of stroke-specific health-related quality of life and is adjusted for people with aphasia (27). SAQOL-39g items are scored on a scale from 1 to 5, and mean scores are calculated for each dimension and for the total sum score. Higher scores indicate a higher quality of life. The SOC-13 measures the main concepts of SOC theory (16). In this study, the SOC-13 items were scored on a scale from 1 to 5. The total sum score was calculated after reversing the scores of the reversely formulated items, resulting in a scale from 13–65. Higher scores indicate higher levels of comprehensibility, manageability, and experiences of meaningfulness in life.
The fatigue questionnaire (FQ-2), Lee’s fatigue scale (LFS-5) (28) and the Ullevaal Aphasia Screening test (UAS) (29) were included to describe the sample.
Sample size calculations
Sample size was determined based on the primary outcome measurement. With the power set at 80% and the significance level (α) at 0.05, the estimated sample size was 300 patients (150 per group). The calculations were based on a repeated measures logistic regression model of the output variable “normal mood” (GHQ-28). In this study, the power of finding a statistically significant difference between groups was 80% for an OR of 1.9 or higher.
Randomization and blinding
A computer-generated block randomization procedure was used to allocate the patients into either the intervention or control arm. Participants were randomly assigned in blocks of 10, stratified by the recruiting centre with an allocation ratio of 5:5. An assistant independent of the research group prepared opaque randomization envelopes with 5-digit patient identification numbers printed on the outside and a note specifying intervention or control on the inside. Two regional study coordinators performed the randomization. Group allocations were communicated solely to the patient and the IP delivering the intervention. To maintain blinding during follow-up, a text message was sent from the study coordinator to the participants before the data collector contacted them with a reminder not to reveal their group allocation.
Statistical methods
The data were analysed using the Statistical Package for the Social Sciences (SPSS), version 25.0, for Windows (IBM Corp., Armonk, NY, USA). All statistical tests were intention-to-treat analyses performed as 2-sided tests with a significance level of α=0.05. Missing data were imputed using multiple imputation by chained equations (MICE) in SPSS (30), and all reported results from the statistical analyses were combined results across 5 imputations based on Rubin’s rule (31).
A logistic regression with time points (T1 vs T2) as the single independent variable was used to assess the odds of a normal mood (GHQ-28<5) and not having depression (Yale) from T1 to T2 separately per treatment group. The changes in mean scores on the SAQOL-39g and SOC-13 from T1 to T2 were examined for each treatment group using paired-sample t-tests.
Logistic regression analyses were used to analyse the effects of the intervention on mood (GHQ-28) and depression (Yale) at 6 months. Multiple linear regression analysis was applied to determine whether participating in the intervention was statistically significantly associated with the participants’ scores on the SAQOL-39g. Based on conceptual and theoretical assumptions, the following baseline characteristics were controlled for in the regression models in each analysis: group allocation, sex, age at admission, rehabilitation services at baseline, care responsibility, living arrangements, comorbidity, stroke severity (NIHSS), stroke aetiology, stroke symptom localization, depression, fatigue and SOC (SOC-13). The baseline value of the outcome measurement analysed was also added as a covariate because the results of the by-group analyses showed significant changes between time points. A variable of recruitment centre was in addition included in the logistic regression analysis of GHQ-28 to control for a potential effect of recruitment centre.
The SAQOL-39g was analysed for both the original and log-transformed (2**) variables because of the non-normal distribution of the data. The results were compared, and no significant differences were found. To simplify interpreting the results, only outcomes from the original data analysis are presented herein.
Independent-samples t-tests were used to test for statistically significant differences in the mean scores on the SOC-13 between the intervention and control groups.
Ethics
The ethical approval of the study was provided by the Regional Committee for Ethics in Medical Research (REC) (2013/2047) and the Data Protection Authorities (2014/1026). The study followed the guidelines of the Declaration of Helsinki.
When invited to participate, eligible participants received oral and written information about the study from trained clinical staff who also obtained informed consent.
If patients showed signs of severe emotional distress during the interviews or intervention, the interviewer/intervention personnel were instructed to offer to interrupt the interview or intervention and consider contacting their general practitioner, a family member or home-care services.
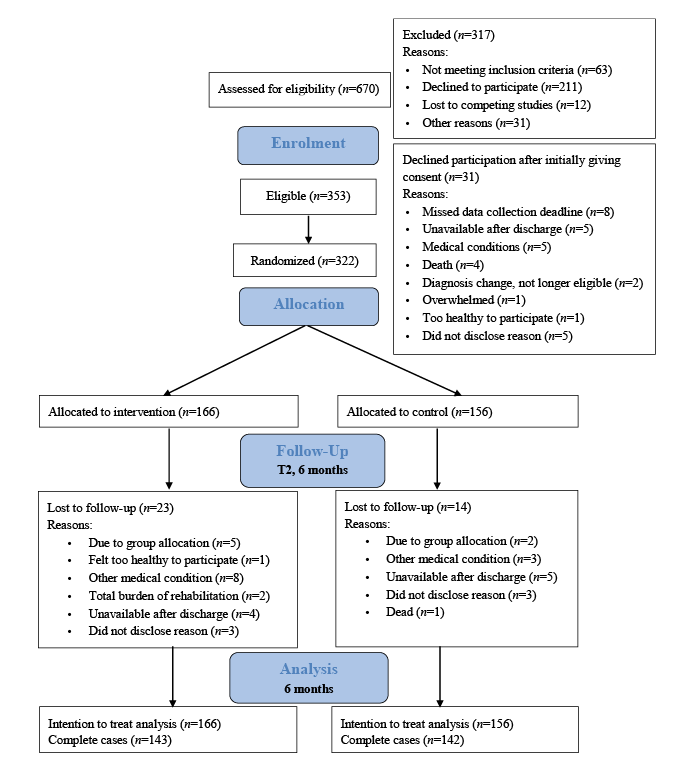
A total of 670 stroke patients were assessed for eligibility, of whom, 353 consented to participate. A final total of 322 participants were randomly assigned to the intervention (n = 166) or control (n = 156) group. The REC only gave permission to register information on the sex and age of the participants who declined to participate. Unfortunately, not all recruiting centres provided complete data; however, in the largest recruiting centre the mean age of those who consented were 64.1 years compared with 64.4 years in the group who did not consent (p = 0.893). The proportion of men and women who consented, 60.8% and 39.2%, respectively, compared with 58.2% and 41.8% who did not consent (p = 0.679) shows no sex disproportion in the groups.Thirty-one participants declined after initially giving consent, reasons are listed in the flow diagram (Fig. 1). Twenty-three participants (7.1%) in the intervention group and 14 (4.4%) in the control group were lost to follow-up at 6 months. Consequently, 285 participants (88.5%) completed the follow-up assessments at 6 months. Fig. 1 shows the participant flow diagram.
Fig. 1. Flow chart of the study.
Baseline characteristics were generally well balanced between the groups (Table I). A numerical difference was noted for depression (Yale), on which 17.5% of participants in the intervention group and 27.6% of those in the control group reported depression at T1. The participants’ mean age was 8 years younger than that of the average stroke patients admitted to hospitals in Norway; 5% more were men, and more patients scored ≤5 on the NIHSS upon hospital admission (70% vs 65%) (2).
Table I. Sample characteristics of the stroke study sample (n = 322) at baseline
Analysis of the implementation fidelity showed that the intervention’s core components were delivered according to protocol, although the intervention trajectories were individualized (32). Based on a composite score of the adherence measures (number of sessions, timeliness of starting, and duration of intervention), 80% of the intervention programmes were implemented with high fidelity. This means that the intervention trajectory was complete (≥6intervention sessions); it began between 4 and 8 weeks (mean 49 days (n = 147)) after the stroke, and the frequency and total duration were a maximum of 17 weeks from session 1 to session 8.
Primary outcome
After dichotomizing the sum score, 99 of the 166
patients (59.6%) in the intervention group and 93 of the 156 patients (59.6%) in the control group had normal mood (GHQ-28<5) at 6 months. Table II shows that, compared with that at baseline, the proportion of participants with normal mood increased in both the intervention and control groups.
Table II. Effect of intervention on outcomes 6 months after stroke
After controlling for the baseline characteristics and recruitment centre, in the logistic regression model, no benefit of the dialogue-based intervention was observed over usual care on mood at T2 (OR: 0.898: 95% CI: 0.54–1.50, p = 0.680) .
By separately exploring the results for the intervention and control groups, it was found that no baseline characteristics demonstrated statistically significant effects on mood at T2 in the intervention group. Two baseline factors affected the odds of a normal mood at T2 in the control group. Higher SOC (OR: 1.098, 95% CI: 1.01–1.19, p = 0.026) increased the odds of normal mood, while comorbidities (OR: 0.282, 95% CI: 0.09–0.83, p = 0.022) decreased the odds of normal mood. This difference should be further explored when the 12-month data are available.
Secondary outcomes
Thirty-seven participants (22.3%) in the intervention group and 36 (23.1%) in the control group reported depression at 6 months (Yale). Compared with those at T1, the intervention group had 8 more participants (4.9%) who reported depression, while the control group had 7 fewer participants (5.4%) who reported depression.
After controlling for the baseline characteristics, the logistic regression model for depression (Yale) showed no benefit of the intervention over usual care at T2 (OR: 1.248, 95% CI: 0.64–2.41, p = 0.507).
By separately exploring the results for the intervention and control groups, it was found that depression at T1 statistically significantly increased the odds of depression at T2 for both the intervention (OR: 5.054 95% CI: 1.73–14.74, p = 0.003) and the control group (OR: 8.965 95% CI: 2.79–28.72, p = 0.001) at 6 months.
Table II shows that the physical domain score on the SAQOL-39g changed significantly from T1 to T2 for both the intervention and control groups.
After controlling for the baseline characteristics in the multiple linear regression model, the analysis showed no benefit favouring the intervention over usual care on the SAQOL-39g mean score (B = –0.026, CI: –0.13–0.08, p = 0.637) at 6 months. Table II lists the subdomain statistics.
When the intervention and control group results were explored separately, it was found that the T1 SAQOL-39g score was a predictor of the T2 SAQOL-39g score in both the intervention (B = 0.380, CI: 0.08–0.67, p = 0.015) and control group (B = 0.464, CI: 0.29–0.63, p < 0.001) at T2. For the intervention group, the NIHSS scoring predicted the T2 SAQOL-39g score (B =–0.030, CI: –0.51 ao –0.01, p < 0.004) and for the control group, the SOC-13 (B =0.013, CI: 0.01–0.02, p < 0.034) predicted the SAQOL-39g score.
Table II shows that the mean sum score on the SOC-13 did not change significantly from T1 to T2 in the intervention or control group, and that the between-group difference at 6 months was not statistically significant.
Main findings
Compared with baseline, the proportion of participants reporting normal mood statistically significantly increased in both the intervention and control groups at 6 months. In contrast to our hypothesis, this study failed to demonstrate that a dialogue-based intervention promoted psychosocial well-being in the intervention group compared with the control group.
No change was detected in the SOC after the intervention. However, the results indicated that a higher SOC level might have a protective effect against the potentially stressful situation imposed by a stroke. The SOC is considered to be strongly related to perceived health (16). Despite the adverse health experiences after a stroke, participants with higher SOC scores had higher odds of a normal mood and higher scores regarding health-related quality of life at T2. This result is consistent with Antonovsky’s (16) theory on salutogenesis, which explains how some people manage well despite adverse health experiences. This finding is also supported by a recent study on how personal factors, such as proactive coping, influence stroke outcomes, seem to be stable over time (33) and demonstrated that in the period from 2 months to 2 years after stroke personal factors did not improve naturally.
Our results differed from those reported in a comparable study that evaluated the effect of motivational interviewing on mood (11). Watkins and colleagues reported a significant difference between the intervention and control groups at 3 months, with 49% of the participants in the intervention group and 39% of the participants in the control group having normal mood at 3 months. At 12 months, the difference between the groups remained significant, with 48% of participants in the intervention group and 37% of participants in the control group reporting normal mood. Watkins’ study was conducted in a hospital with a different and shorter intervention, and the data were primarily collected by mail. Comparably, a substantially higher percentage of participants in both groups (59.6%) had normal mood at 6 months in our study. Although the results failed to demonstrate effectiveness of this dialogue-based intervention for promoting psychosocial well-being after stroke, conducting an RCT in a complex setting with face-to-face data collection imposes several factors that may explain the neutral results obtained in this study.
The Norwegian authorities have encouraged rehabilitation services delivered in the municipalities through the Coordination Reform (12) and through the clinical guidelines for treatment and rehabilitation after stroke (19). A considerable proportion of participants reported receiving rehabilitation services post-stroke (66% at T1 and 55% of T2). Therefore, the rehabilitation needs of some participants may have already been met through usual care. No standardized psychological support exists in the follow-up after stroke in Norway and we lack a complete overview of the content of the follow-up that the participants received. However, since the participants lived in more than 70 different municipalities, we must assume that the follow-up varied substantially.
The most frequently reported follow-up was physical therapy (59% at T1, 36% of T2). This finding was supported by a recently conducted study comparing stroke rehabilitation in Norway and Denmark, suggesting that follow-up focuses more on physical rehabilitation in Norway, while psychological support is better organized and implemented in Denmark (34).
We experienced that some of the participants struggled to distinguish ordinary healthcare services from the intervention, and participants in the control group perceived the study participation and the structured assessment interviews as a form of intervention. Conducting face-to-face assessments ensured high compliance and complete data during collection, but also had some disadvantages. Face-to-face interviewing is a form of social interaction and merely being involved in these interviews may have positively affected the patients’ psychosocial well-being. Having an interviewer visit their homes 1 and 6 months after discharge may have also led to the perception of having received an intervention, even by those in the control group.
Social desirability bias (35) is another factor that potentially affected the results. If the respondents had acted in ways or held attitudes that they felt were undesirable, their answers might have been affected. Consequently, they might have underreported socially undesirable attitudes and behaviours while enhancing attitudes and behaviours they believed were expected in coping with their life after stroke.
Stroke recovery is multifaceted. Finding the optimal instrument to capture the impact of a psychosocial intervention rather than the expected natural recovery after stroke was challenging. Recovery depends on different mechanisms and treatments at different phases after the acute injury, which range from hours to many months. Although improvement varies among individuals, most patients improve during the first period following the stroke because of acute care treatment and post-lesional plasticity (36).
Another issue is a possible ceiling or floor effect of the outcome measures, which is a known risk with instruments addressing aspects of psychosocial well-being (37). Many participants had no or minor stroke symptoms and limited adverse effects on their daily living activities after their stroke. This outcome resulted in maximum scores on several questions, especially on the SAQOL-39g.
Furthermore, well-being is a subjective phenomenon. Physical sequelae, side-effects of medication, and overall spontaneous improvement may affect how patients answer questions immediately after a stroke compared with 6 months post-stroke. This personal reporting of subjective appraisal introduces the possibility of a response shift into the assessment. A response shift is a change in the meaning of one’s self-evaluation due to changes in the respondent’s internal standards of measurement and values or a redefinition of the construct by the respondent (38). A response shift may lead to a reconsideration of the current life and affect the outcome measurement scores. This outcome could occur in both groups regardless of adding an intervention and may result in underestimating the treatment effect of psychosocial interventions (38).
The strengths of the study were the thorough development, feasibility and customization of the intervention, which were conducted as recommended by the UK MRC guidance for developing and evaluating complex interventions (13).
In addition, the study was conducted per the rigorous recommendations in the CONSORT statement (39). The intervention fidelity was high and the study was conducted according to protocol.
All personnel involved in the data collection and intervention delivery, underwent a 3-day training programme, individual guidance according to need by members of the research team and participation in group sessions throughout the study.
However, the study had some limitations. We cannot be sure that the training and follow-up of the intervention personnel were sufficient for all of them.
Although the participants represented the largest group of stroke patients admitted to hospitals in Norway, patients with the most severe stroke or aphasia were difficult to include due to early enrolment and difficulties in obtaining informed consent.
The 2 most common reasons for declining to participate, were that they did not feel the intervention suited them or that they had too much going on to commit to participation, but detailed information on the reasons for non-participation were limited due to strict ethics guidelines limiting questions regarding decline.
If a standardized test was not applied in the evaluation of cognitive function (e.g. due to aphasia), the recruiting personnel reported cognitive challenges as “mild”, “moderate” or “severe”, based on information from the assessments made by the multidisciplinary team. This procedure did not provide reliable information that was applicable to the analysis.
Unfortunately, we do not have a sufficient number of participants to perform subgroup analyses for potentially vulnerable groups, such as those experiencing cognitive challenges, aphasia or lacking social support.
In addition, we questioned whether the control group functioned as intended, because participants in both the intervention and control groups had substantial follow-up time as part of their usual care. The control group also received personal home visits for data collection, which they may have interpreted as an intervention, which thus may have impacted their psychosocial well-being (More details from the control group experiences will be reported as part of the study´s process evalution) . The participation may also have increased the awareness of stroke-related changes and facilitated reflection on psychosocial well-being, changes and symptoms that secondarily affected the outcome.
In conclusion, psychosocial well-being, as measured by the GHQ-28, improved significantly during the first 6 months after stroke in both the intervention and control groups. The results at 6 months indicated that participating in a dialogue-based intervention during the first 6 months post-stroke in addition to usual care did not affect psychosocial well-being. Further research is needed to investigate which factors promote psychosocial well-being after stroke, particularly among patients at high risk of experiencing psychosocial problems.
The authors thank all the patients who participated in the study. We acknowledge all participating centres of the RCT for granting access to participants and especially the recruitment personnel for their efforts in enrolling participants into the trial. We thank the data collectors for their extensive contribution to the complete data collection and the intervention personnel for conducting a remarkable number of interventions.
Clinical Trial Registration. URL: https://clinicaltrials.gov. NCT02338869; registered 10/04/2014.
Funding. The research leading to these results received funding from the European Union Seventh Framework Programme (FP7-PEOPLE-2013-COFUND) under grant agreement no. 609020 - Scientia Fellows (LKB), the South-Eastern Norway Regional Health Authority (Project number 2013086) (US, LKB) and the Extra Foundation (2015/FO13753) (EGH).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize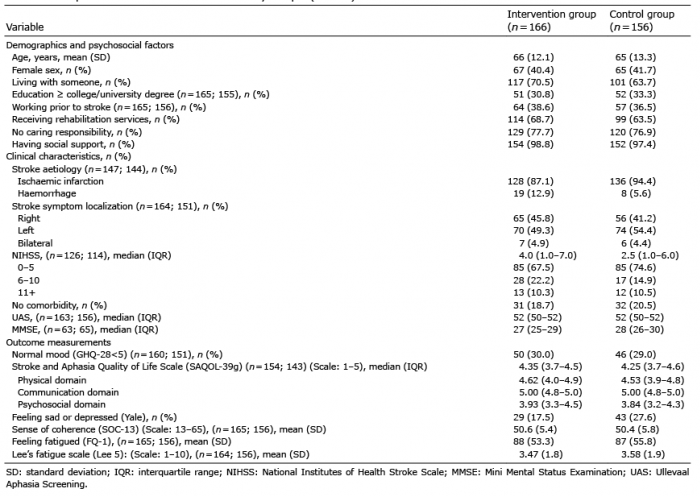 Click to show fullsize
Click to show fullsize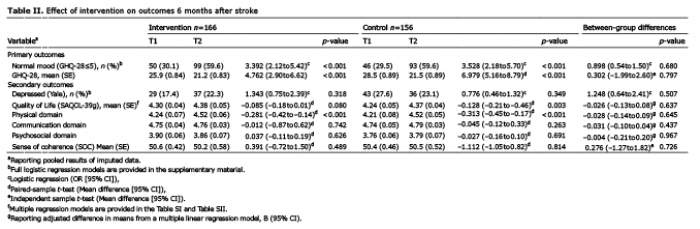 Click to show fullsize
Click to show fullsize