
From the 1Department of Orthopaedics, Rehabilitation Medicine and Physical Therapy, Leiden University Medical Centre, Leiden, 2Department of Biomedical Data Sciences, Section Medical Decision Making, Leiden University Medical Centre, 3Basalt, The Hague, 4Basalt, Leiden, and 5Faculty of Health, Nutrition and Sports, The Hague University for Applied Sciences, The Hague, The Netherlands
Objective: Despite the increasing availability of
eRehabilitation, its use remains limited. The aim of this study was to assess factors associated with willingness to use eRehabilitation.
Design: Cross-sectional survey.
Subjects: Stroke patients, informal caregivers, health-care professionals.
Methods: The survey included personal characteristics, willingness to use eRehabilitation (yes/no) and barriers/facilitators influencing this willingness (4-point scale). Barriers/facilitators were merged into factors. The association between these factors and willingness to use eRehabilitation was assessed using logistic regression analyses.
Results: Overall, 125 patients, 43 informal caregivers and 105 healthcare professionals participated in the study. Willingness to use eRehabilitation was positively influenced by perceived patient benefits (e.g. reduced travel time, increased motivation, better outcomes), among patients (odds ratio (OR) 2.68; 95% confidence interval (95% CI) 1.34–5.33), informal caregivers (OR 8.98; 95% CI 1.70–47.33) and healthcare professionals (OR 6.25; 95% CI 1.17–10.48). Insufficient knowledge decreased willingness to use eRehabilitation among patients (OR 0.36, 95% CI 0.17–0.74). Limitations of the study include low response rates and possible response bias.
Conclusion: Differences were found between patients/informal caregivers and healthcare professionals. However, for both groups, perceived benefits of the use of eRehabilitation facilitated willingness to use eRehabilitation. Further research is needed to determine the benefits of such programs, and inform all users about the potential benefits, and how to use eRehabilitation.
Key words: stroke; barriers and facilitators; implementation; rehabilitation; eRehabilitation, survey.
Accepted Jul 8, 2019; Epub ahead of print Aug 15, 2019
J Rehabil Med 2019; 51: 665–674
Correspondence address: Berber Brouns, Albinusdreef 2, NL-2333 ZA Leiden, The Netherlands. E-mail: b.brouns@lumc.nl
The use of digital eRehabilitation after stroke (e.g. in serious games, e-consultation and education) is increasing. However, the use of eRehabilitation in daily practice is limited. As a first step in increasing the use of
eRehabilitation in stroke care, this study examined which factors influence the willingness of stroke patients, informal caregivers and healthcare professionals to use eRehabilitation. Beliefs about the benefits of eRehabilitation were found to have the largest positive impact on willingness to use eRehabilitation. These benefits included reduced travel time, increased adherence to therapy or motivation, and better health outcomes. The willingness to use eRehabilitation is limited by a lack of knowledge about how to use eRehabilitation.
Stroke is a major cause of disability worldwide (1), including long-term physical and cognitive impairments (2). Recovery of these functions requires specialized multidisciplinary stroke rehabilitation (3). Due to the increasing incidence of stroke and the major increase in the cost of healthcare (4), there is a need for more efficient rehabilitation strategies. The rapid growth of accessible and affordable information and communication technology (ICT) offers a potential solution, and may improve the effectiveness of rehabilitation (5, 6).
The use of ICT in rehabilitation (i.e. eRehabilitation) is a method for delivering rehabilitation in addition to conventional modes of delivery in the sub-acute and chronic phases of rehabilitation. eRehabilitation is delivered using a variety of possible ICT devices, such as computers, tablets and smartphones, and includes exercise programmes, serious gaming (conducting rehabilitation through playing games), education and e-consultations (7). Randomized clinical trials (RCTs) showed that eRehabilitation can decrease stroke-related impairments (6, 8, 9), reduce physical effort required from healthcare professionals, make rehabilitation accessible to larger number of stroke patients (5), make it possible to continue therapy-related cognitive and physical activities after discharge (10), decrease chronic disability, and facilitate home-therapy (11, 12). A positive attitude toward the use of eRehabilitation was found among all end-users, including stroke patients, informal caregivers (13–15) and healthcare professionals (16, 17). The use of eRehabilitation has been associated with enjoyment, extra feedback, physical and cognitive benefits and the possibility to address the limitations of the current rehabilitation system, such as limited therapy hours, low motivation and poor adherence to exercise (18).
Despite these promising results and widespread agreement about the importance and potential of eRehabilitation, its implementation (i.e. making eRehabilitation effective in stroke rehabilitation) is lagging behind (19). A previous focus group study explored which factors influence the implementation of eRehabilitation (20). This study, together with other literature, reported that the implementation of eRehabilitation is hampered by a lack of confidence about using hardware or software (15, 21) and the fear that eRehabilitation could replace face-to-face contact (13, 16, 20). Skilled healthcare professionals or informal caregivers are needed to support patients in using complex ICT programs (11, 14, 20). Healthcare professionals raised concerns about adapting the rehabilitation process when added eRehabilitation (22). Moreover, eRehabilitation is feasible only if tailored to the individual needs of the recovering patient (18, 20). In addition, the safety of unsupervised rehabilitation exercises is unknown (11) and lack of substantial reimbursement by insurers is hampering its widespread implementation (6). Healthcare professionals’ decision to start using eRehabilitation is influenced by their beliefs about how eRehabilitation helps them in performing their work (23).
Although the above-mentioned studies have identified some factors influencing the use of eRehabilitation, it is not known which factors have the greatest impact. This insight is necessary in order to tailor an implementation strategy to the factors that may influence use of eRehabilitation, and to develop an effective implementation strategy to increase the use of eRehabilitation in stroke patients. Therefore, the aim of this study was to assess which factors are associated with willingness to use eRehabilitation after stroke, for patients, informal caregivers and healthcare professionals.
Design and setting
This cross-sectional study within the Dutch medical specialist rehabilitation setting used a single online survey, based on the results of a previous focus group study (20). The present study was conducted in June 2016, among stroke patients, their informal caregivers and healthcare professionals at 2 rehabilitation centres (Basalt The Hague and Basalt Leiden). It was approved by the Medical Ethics Review Board of Leiden University Medical Centre [P15.281]. STROBE statements were used for adequate sampling, analyses and reporting.
Subjects
Stroke patients were selected if they met the following inclusion criteria: aged ≥ 18 years, having started rehabilitation after June 2011 and completed it before May 2016, living independently, able to understand and read Dutch, and having an email address. A total of 400 patients, 200 from each rehabilitation centre, were randomly selected from a list of approximately 2,700 eligible patients. They received an invitation email from a rehabilitation physician who was involved in this study, including an introduction to the study and a link to the online survey. The email also included information for the informal caregivers and a link to a separate survey for the informal caregivers. Since not all patients had an informal caregiver, the number of informal caregivers invited is unknown.
Healthcare professionals were eligible if they had at least 2 years of experience working in a multidisciplinary stroke team and were still actively seeing stroke patients in rehabilitation care in the Netherlands. Invited healthcare professionals included 3 disciplines that are commonly involved in stroke rehabilitation: rehabilitation physicians, psychologists and physiotherapists. These disciplines were invited since the eRehabilitation intervention in this study concerned physical and cognitive training, 2 domains that are mostly addressed by these disciplines. A Dutch medical address book including most healthcare professionals in the Netherlands was used to identify members of the 3 disciplines. All eligible healthcare professionals who worked in rehabilitation care received an invitation email.
Non-responders received 2 reminders via email, 2 and 4 weeks after the invitation. Immediately after completing the survey, participants were sent a note thanking them for their willingness to participate. Although participants were invited by email, they completed the survey anonymously, with only the IP address known to the researchers. The personal characteristics collected were not traceable (e.g. age was used instead of date of birth). Participants did not receive the results of the study.
Development and content of surveys
Preceding focus group study. The survey was developed based on the results of an earlier focus group study (20). In 8 focus groups (2 with healthcare professionals and 6 with patients/informal caregivers), barriers and facilitators for willingness to use eRehabilitation were identified. Participating healthcare professionals included physiotherapists, psychologists, occupational therapists, speech therapists, rehabilitation specialists and managers. Participating patients were selected using purposeful sampling. The analysis and results of the focus group study have been published in detail elsewhere (20).
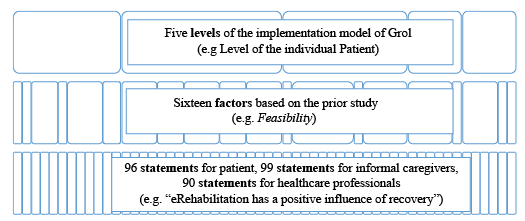
Barriers/facilitators regarding related topics were merged into factors based on Grol’s implementation model (24). This model includes 6 levels; the innovation, the organizational context, individual patients, individual professionals, the social context, and the economic and political context. The focus group study identified 14 factors at 5 levels (Fig. 1). Factors at the social level were not identified and therefore not incorporated in the present survey. One change was made to the factors identified in the focus group study; for the purpose of the survey the factors Motivation to change, at the level of both the individual patients and the individual professionals, was divided into Motivation to change and Motivation not to change, resulting in 16 factors being included in the present study.
Fig. 1. Relationship between levels, factors and statements.
Survey content. Separate surveys were developed for patients, informal caregivers and healthcare professionals. The surveys consisted of 3 parts: (i) questions about responder characteristics, (ii) statements about barriers and facilitators influencing willingness to use eRehabilitation for stroke patients, and (iii) questions about willingness to use eRehabilitation;
(i) Responder characteristics. All 3 surveys included questions about age and sex. In addition, patients and informal caregivers were asked about the time since the stroke (in months), living status (living alone or living with partner/family), employment (paid job, no paid job), self-perceived impairment (cognitive, physical, communicative), use of electronic devices in daily life (smartphone, tablet, laptop, computer) and previous experience with eRehabilitation (no, yes; if yes: exercises, games, information).
For healthcare professionals, the survey started with the question “Are you working with stroke patients?” If not, the survey was ended. If yes, 12 questions followed, regarding their work setting (primary care, rehabilitation centre, general hospital), years of work experience, number of new stroke patients per month and their current use of eRehabilitation (no, yes; if yes: exercises, games, information).
(ii) Barriers/facilitators statements. For the current study, each potential barrier and facilitator identified in the focus group study was translated into a neutral statement. A total of 69 statements were formulated, based on the transcripts of the focus group sessions of patients, informal caregivers and healthcare professionals. For patients and informal caregivers, 26 statements were formulated, based on barriers/facilitators that were not reported by the healthcare professionals. This concerned the design of the eRehabilitation in terms of colour, use of pictographs and beliefs about the skills and knowledge required to use eRehabilitation. Three statements were formulated for the informal caregivers alone, concerning the information provided to them. Nineteen statements were formulated for the healthcare professionals only. These included organizational constraints, integration of eRehabilitation in the current rehabilitation process, and monitoring patients’ results. The barrier/facilitator statements thus included 95 (69 + 26) statements for the patients, 98 (69 + 26 + 3) statements for the informal caregivers and 88 (69 + 19) statements for the healthcare professionals (see Appendix I for all statements). The influence of the barriers/facilitators mentioned in the statements on willingness to use eRehabilitation was rated on a 4-point Likert scale (1=unimportant, 2=somewhat unimportant, 3=somewhat important, 4=important, or 1=disagree, 2=partly disagree, 3=partly agree, 4=agree).
(iii) Willingness to use eRehabilitation. Since eRehabilitation is still not widely used, the surveys included 1 question about willingness to use eRehabilitation: “Would you like to use eRehabilitation in addition to the regular rehabilitation care?”’ (yes, no).
The surveys were tested in a pilot study with 3 stroke patients who were still undergoing rehabilitation treatment (1 male, 2 females; mean age 59 years; mean time since stroke 10 weeks; all undergoing in-patient rehabilitation for stroke) and 3 healthcare professionals (2 males, 1 female; 2 physiotherapists, 1 occupational therapist; mean age 38 years; mean work experience 13.3 years) working in a rehabilitation centre. The surveys were tested for feasibility, legibility, readability and presentation (e.g. perceived statement difficulty, response errors, screen layout, etc.). Testing led to small changes in the phrasing and layout. The survey for informal caregivers was adjusted based on feedback from the other surveys.
Statistical analysis
Participants who completed ≥ 90% of the survey were included in the analysis, and we did not impute for missing values. Analysis of survey data was carried out using Statistical Packages for the Social Sciences (IBM SPSS 22.0 for Windows).
Participant characteristics. Participant characteristics included socio-demographic data and disease- and work-related characteristics, presented as numbers with percentages or means with standard deviation (SD). Age and sex of responders were compared with those of the stroke population of 2,700 eligible patients in the 2 participating rehabilitation centres, using independent t-test and and Wilcoxon-Mann-Whitney test.
Descriptive analyses. Median scores with interquartile ranges (IQR) were calculated for each of the statement about barriers/facilitators. Based on the median score, the 5 most important statements were reported for each group (patients, informal caregivers and healthcare professionals), and for physicians, physiotherapists and psychologists separately. For statements with a similar median, a more specific ranking (lowest number equals largest influence) was made, based on the mean.
Association between barriers/facilitators and willingness to use eRehabilitation. The association between a barrier/facilitator and willingness to use eRehabilitation was assessed using logistic regression analysis. The methods were comparable to those used in previous qualitative research about barriers and facilitators to the implementation of innovations in healthcare (25, 26). This analysis was performed separately for patients, informal caregivers and healthcare professionals, and consisted of 3 steps:
All statements about barriers/facilitators were merged into factors, as predefined in the focus group study. The internal consistency of each factor (i.e. group of statements) was calculated using Cronbach’s alpha. A Cronbach’s alpha of 0.7 was considered acceptable (27) and was determined using a factor analysis with an orthogonal rotation approach, using principal component analysis and varimax rotation (28).
Univariate logistic regression analyses were performed to assess whether a factor was significantly associated with willingness to use eRehabilitation. Factors were used instead of statements, to prevent over-fitting of the logistic regression model by including too many variables. The factors were included as the independent variables, and willingness to use eRehabilitation as the dependent variable. In addition to the factors derived from the focus group study, the characteristics of responders asked for in the first part of the survey, viz. age, discipline (healthcare professionals only) and previous use of eRehabilitation (patients and healthcare professionals only) were also included in the analysis. Odds ratios (OR) with a 95% confidence interval (95% CI) are reported.
As individual factors may be related to others, the factors and responder characteristics significantly associated with willingness to use eRehabilitation were included in a multivariate logistic regression analysis using a backward likelihood ratio method. OR values with 95% CI are reported. An OR higher than 1 indicates that a factor was positively associated with willingness to use eRehabilitation, while an OR lower than 1 indicates that a factor was negatively associated with willingness to use eRehabilitation.
Participant characteristics
The survey was completed by 125 of the 368 (34%) invited patients, 43 informal caregivers (response rate unknown) and 102 of the 288 (37%) invited healthcare professionals (Fig. 2). Reasons for non-response were not verified, except for 30 (10%) healthcare professionals that did not complete the survey because they were not working with stroke patients.
Fig. 2. Study inclusion flow.
Respondent characteristics for the patients, informal caregivers and healthcare professionals were as follows: mean age was 58.2 years (SD 11.4), 58.4 years (SD 12.0) and 41.9 years (SD 10.5), respectively; and 72 (58%), 16 (37%) and 25 (24%), respectively, were male (Table I). Age and sex did not differ between the responders and the sample of 2,700 patients eligible for this study. Mean time since stroke was 30.6 months (SD 29.2). Most patients (n = 113, 90%) and informal caregivers (n = 41, 95%) used electronic devices such as laptops, tablet or smartphone daily. One-quarter of the patients (n = 30, 24%) and more than one-third of the healthcare professionals (n = 38, 37%) had used eRehabilitation before, and 106 (84%) patients, 38 (88%) informal caregivers and 97 (92%) healthcare professionals reported that they were willing to use eRehabilitation. Of the 102 healthcare professionals, 41 (39%) were physiotherapists, 14 (13%) psychologists and 47 (45%) physicians. Most healthcare professionals (n = 73, 72%) worked in a rehabilitation centre; other settings included primary care (n = 9, 9%) and hospital (n = 34, 32%).
Table I. Characteristics of patients, informal caregivers and healthcare professionals participating in a survey on the use of eRehabilitation
Descriptive statistics
The 5 most important barriers/facilitators influencing willingness to use eRehabilitation are shown in Table II. One facilitator appeared in the top 5 highest scoring statements for both patients, informal caregivers and healthcare professionals, viz. “The use of eRehabilitation has a positive influence on the patient’s recovery.” (see Table IIa). Other barriers/facilitators in the top 5 for patients and informal caregivers mostly concerned statements belonging to the factors Advantages of use (such as the possibilities of online information, online agenda, online survey, etc.) and Motivation to change, at the level of individual patients (i.e. benefits of using eRehabilitation for patients, such as reduced travel time and increased motivation). Healthcare professionals mostly endorsed statements belonging to the factor Feasibility (such as support from a helpdesk, video-instructions or frequently asked questions (FAQs)). A ranking for all statements based on the median and mean is shown in Appendix I.
When calculated for each discipline separately, only the facilitator “A helpdesk is available for patients” in the factor Feasibility was found in the top 5 for all disciplines (see Table IIb). The top 5 for physicians mostly involved statements belonging to the factor Attractiveness (such as the content of an eRehabilitation programme), while that for psychologists consisted mostly of statements belonging to the factor Motivation to change at the level of individual patients (such as benefits of using of eRehabilitation). Physiotherapists endorsed statements in 5 different factors (Organization of care, Accessibility, Attractiveness, Advantage of use, and Feasibility).
Table IIa. Five highest scoring statements (based on median and mean) for willingness to use eRehabilitation (range 1–4) among stroke patients, informal caregivers and professionals, as medians (interquartile range)
Table IIb. Five highest scoring statements (based on median and mean) for willingness to use eRehabilitation (range 1–4) after stroke, for each individual discipline, as medians (interquartile range)
Association between influencing factors and willingness to use eRehabilitation
A confirmatory factor analysis (step 1) showed that the mean Cronbach’s alpha of statements merged into factors was 0.82 (range 0.6–0.9), with 1 factor loading below 0.7.
In step 2 (univariate regression analyses), a statistically significant association was found for all end-users between willingness to use eRehabilitation and the factors Feasibility, Organization of care and Motivation to change (at the level of the individual patient, see Table III). For the patients, the factors Accessibility, Attractiveness, Advantages of use, Time and Knowledge were also significantly associated with willingness to use eRehabilitation; for informal caregivers, an association was found for the factors Accessibility and Advantages of use; for the healthcare professionals, an association was found for the factors Time and Motivation not to Change (at the level of the individual professional). In addition to the factors in the model by Grol (25), we tested the responder characteristics of age, discipline and previous use of eRehabilitation, and these were found not to be significantly associated with willingness to use eRehabilitation (see Table III).
Step 3 (the multivariate logistic regression analysis) showed that the factor Motivation to change at the level of the individual patient was positively associated with willingness to use eRehabilitation by patients (OR 2.68; 95% CI 1.34–5.33), informal caregivers (OR 8.98, 95% CI 1.70–47.33) and healthcare professionals (OR 4.08, 95% CI 1.36–12.23). For patients, the factor Knowledge (including the statement “I don’t have sufficient knowledge to use eRehabilitation”) was negatively associated with willingness to use eRehabilitation (OR 0.36 and 95% CI 0.17–0.74).
Table III. Factor analyses and uni- and multivariate regression analyses for each factor of the model by Grol and for responder characteristics, for patients, informal caregivers and healthcare professionals
This cross-sectional study among patients, informal caregivers and healthcare professionals has shown that barriers/facilitators influencing willingness to use eRehabilitation are largely similar for patients and caregivers, but are different for healthcare professionals. Whereas its use by patients/caregivers is more associated with the opportunity to improve their health via eRehabilitation, its use by healthcare professionals is more associated with its feasibility. In addition, willingness to use eRehabilitation by patients, informal caregivers and healthcare professionals was positively associated with its expected benefits for stroke patients (e.g. reduced travel time, increased motivation, better health outcomes, increased therapy adherence, etc.). Patients’ willingness to use eRehabilitation was negatively associated with a lack of knowledge regarding its use.
For all end-users, the 5 most important factors found in this study have shown that a “positive influence on patient recovery” is the most important facilitator for willingness to use eRehabilitation. This might sound obvious, but, in fact, many potential barriers/facilitators for all kinds of healthcare innovations are quite obvious. The logistical regression analyses has revealed that other factors that might seem obvious, such as sufficient time for education and proper financial arrangements, are not associated with willingness to use eRehabilitation and should therefore have lower priority in an implementation strategy. In any case, “positive influence on patient recovery” stands out for all stakeholders, so there is an urgent need for more evidence regarding this positive influence. This is one of the most important challenges in eRehabilitation. Although the potential advantages of eRehabilitation seem clear, the lack of currently available evidence hampers its implementation in stroke rehabilitation, therefore more high-quality research determining the effectiveness of eRehabilitation interventions is urgently required (6).
In contrast to the above-mentioned similarity, this study has also identified differences between end-users regarding certain factors that are important for willingness to use eRehabilitation. Patients/caregivers were more willing to use eRehabilitation because of its benefits (in this study merged in the factor Motivation to change). Many of these benefits were found important in previous studies, viz. the possibility to train at home (29), independent continuation of therapy activities (10) and easy contact with healthcare professionals after discharge or during outpatient therapy (16, 17). Thus, both personal contacts and a suitable eRehabilitation approach are important. Therefore, eRehabilitation appears to be best offered in a blended intervention in which it is added to conventional rehabilitation (7, 15). The 2017 Stroke Best Practice Recommendations also concluded that eRehabilitation interventions can only achieve their full potential if integrated in and added to existing stroke services delivery plans (30).
In contrast to the patients, the healthcare professionals considered the factor Feasibility to be the most important one. This includes support for patients from a helpdesk, video instructions and FAQ. Support for the healthcare professionals (which was also part of the factor Feasibility) was not reported to be important. This shows that healthcare professionals are concerned about sufficient patient support in the use of eRehabilitation during the care process. This is not in line with a previous study among health professionals by Liu et al. (23) about factors influencing the use of eRehabilitation. They reported that performance expectancy (“the degree to which an individual believes that using the system will help to attain gains”) was the strongest predictor of the use of new technologies by healthcare professionals. Liu’s “performance expectancy” section included 6 questions about patient outcomes, such as accomplishing patient goals quickly, improving daily life and increasing the quality of rehabilitation, and thus closely resembles our factor Motivation to Change at the level of the individual patient, which was considered important by patients/caregivers in the current study.
Our logistic regression analyses have shown that beliefs about potential patient benefits are associated with willingness to use eRehabilitation for patients, informal caregivers and healthcare professionals. The study by Liu et al. (23) already reported that performance expectancy (i.e. the benefits of using a system) is the strongest predictor of the adoption of new technologies by healthcare professionals. The present study suggests that this is also true for patients and their informal caregivers. Another factor associated with willingness among our patients to use eRehabilitation was Knowledge: patients have to feel confident about starting to use eRehabilitation. This is in agreement with the results of some previous studies. A review by Pugliese et al. concluded that the most commonly reported patient barrier was that of following instructions about how to use the device (31). A feasibility study by Palmcrantz et al. (29) found that the majority of stroke patients needed support from a physiotherapist to start using home-based eRehabilitation, and in a focus group study by Saywell & Taylor (32), the participants em-phasized that simple, explicit information on how and why to perform is crucial (31). Educating patients and involving them as partners in the development process was an important prerequisite for the successful use of eRehabilitation in stroke care (16).
Previous research has also shown that the use of technologies such as eRehabilitation is accurately predicted by healthcare professionals’ willingness to use new technologies (24). In the current study, willingness to use eRehabilitation, rather than the actual use of eRehabilitation, was used as the dependent variable. This was done because most of the patients and healthcare professionals invited to participate in the current study were not using eRehabilitation in their daily rehabilitation practice. Since willingness is an accurate predictor of actual use, the factors identified in the current study may not only influence willingness to use eRehabilitation, but also its actual use. In addition, univariate regression analyses showed no associations between willingness to use eRehabilitation and its prior use. In all, this suggests that willingness to use eRehabilitation is a good predictor of its actual use, but is not changed by prior experience with eRehabilitation.
This study had some limitations. First, patients were approached via email, and not all patients had registered an email address. This may have resulted in a response bias, since patients with an email address may have a different perspective on eRehabilitation compared with those without. Secondly, the limited response rate may have affected the generalizability of the results, since those with an interest in eRehabilitation may have been more willing to participate and may have perceived other barriers and facilitators to the use of eRehabilitation compared with those who did not respond. However, the response rate of the current study is comparable with that in other rehabilitation studies (33, 34), and the age and sex of responders did not differ from those of the non-responders. In addition, the age of our responders may seem low, but the Dutch medical specialist rehabilitation setting does not included geriatric rehabilitation care, which explains why the study sample was relatively young. This may have influenced out finding that age was not a significant factor. Thirdly, regression analyses could not be performed separately for the 3 disciplines of healthcare professionals, due to the small number of participants. In addition, occupational and speech therapists were not included in this study, although they do play an important role in stroke rehabilitation. Since these therapists participated in the previous focus group study, their perspectives were included in the survey, but need to be explored in future studies. The differences found between disciplines in the 5 highest scoring barriers/facilitators also warrant further research, in which occupational and speech therapists should be included.
In conclusion, barriers/facilitators and their association with willingness to use eRehabilitation differ among end-users. This implies that, during the development and implementation of eRehabilitation, all end-users must be involved to ensure that eRehabilitation suits users’ needs and that their willingness to use it is optimized. Important aspects that should be taken into account during both the development and implementation include motivation to change, feasibility and knowledge about using eRehabilitation. Since beneficial outcomes for patients are important factors in willingness to use eRehabilitation, future research should assess the effectiveness of stroke eRehabilitation, preferably in the context of a blended care strategy.
The authors would like to thank all the patients, their informal caregivers, and healthcare professionals who participated in the survey.
Funding: This project was supported financially by Stichting Innovatie Alliantie (grant 2014-046PRO).
Appendix 1. Ranking of statements in each factor, for patients, informal caregivers and healthcare professional. Lowest number equals largest influence
Appendix I. Cont


 Click to show fullsize
Click to show fullsize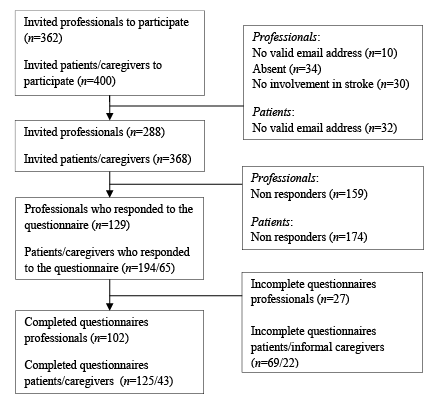 Click to show fullsize
Click to show fullsize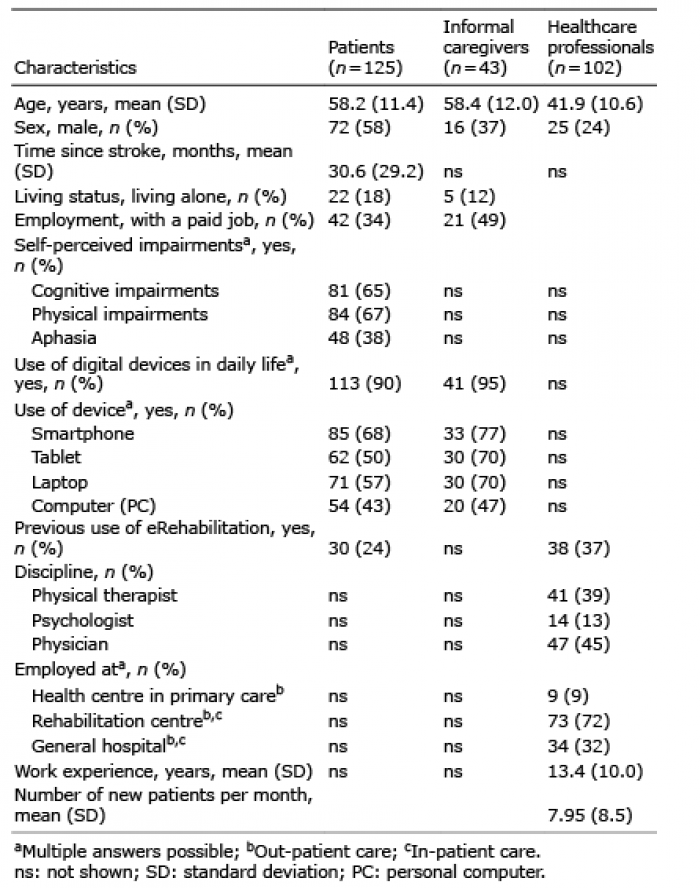 Click to show fullsize
Click to show fullsize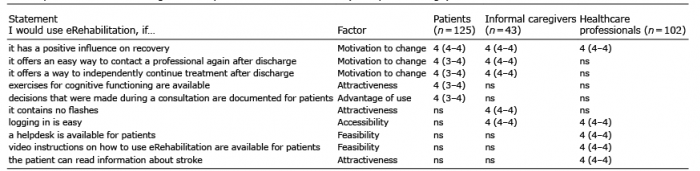 Click to show fullsize
Click to show fullsize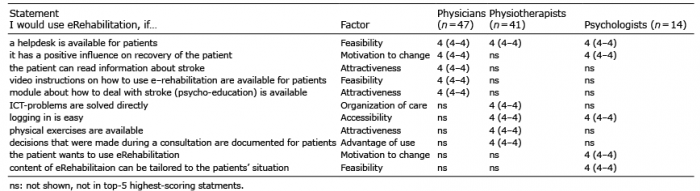 Click to show fullsize
Click to show fullsize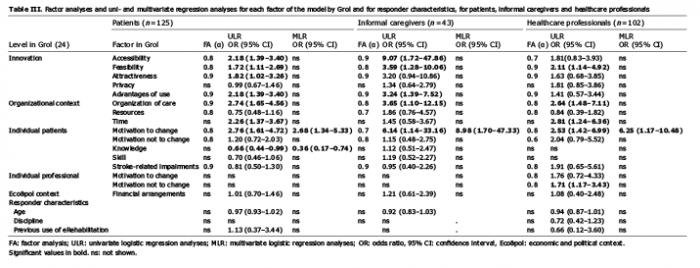 Click to show fullsize
Click to show fullsize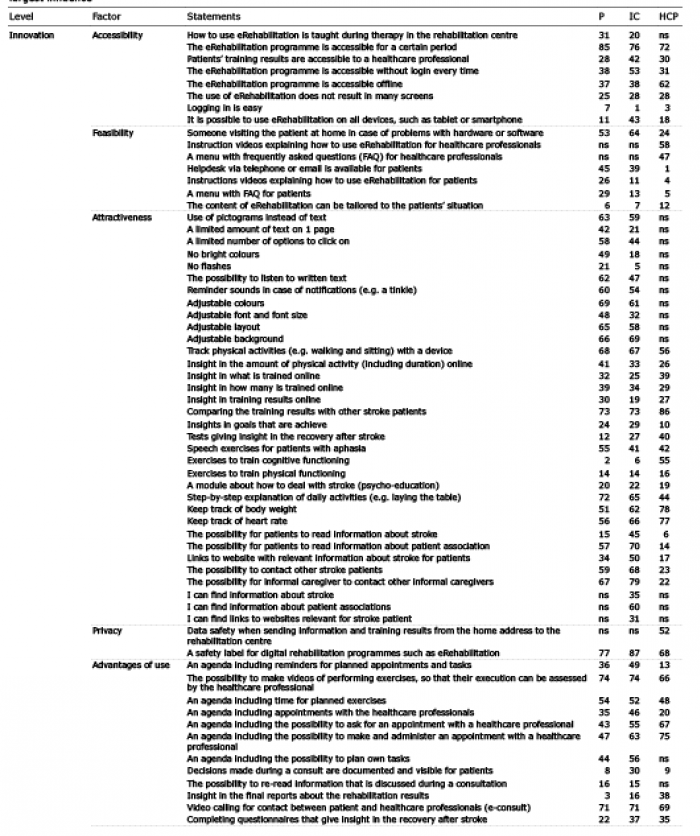 Click to show fullsize
Click to show fullsize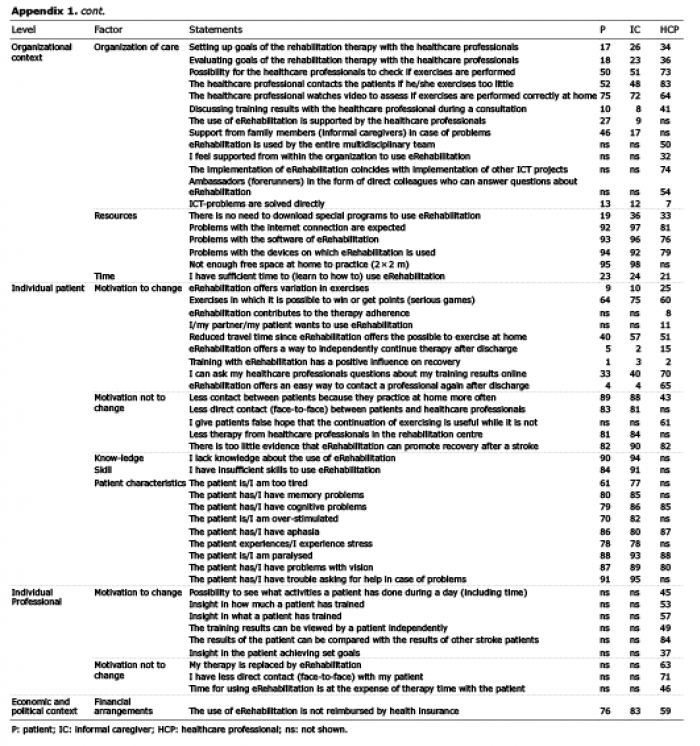 Click to show fullsize
Click to show fullsize