
From the 1Department of Health Sciences, Physiotherapy Research Group, Lund University, 2Department of Neurology, Rehabilitation Medicine, Memory Diseases and Geriatrics, Skåne University Hospital, 3Department of Clinical Sciences, Lund University, Lund, and 4Department of Health Sciences, Luleå University of Technology, Luleå, Sweden
Objective: To explore stroke survivors’ experiences of healthcare-related facilitators and barriers concerning return to work after stroke.
Design: A qualitative study.
Setting: Outpatient stroke rehabilitation unit at a University Hospital in southern Sweden.
Participants: A convenience sample of 20 persons admitted to Skåne University Hospital for acute stroke care (median age 52 years), in employment of at least 10 h per week at stroke onset and been referred to stroke rehabilitation within 180 days.
Methods: The interviews were performed by focus groups, and the data were analysed by content
analysis.
Results: Facilitating factors were a tailored rehabilitation content with relevant treatments, adequate timing and a structured stepwise return-to-work process. A lack of sufficient early healthcare information, rehabilitation planning and coordination were perceived as barriers. An early rehabilitation plan, a contact person, and improved communication between rehabilitation actors were requested, as well as help with work transport, home care, children and psychosocial support for families.
Conclusion: Tailored rehabilitation content and a structured stepwise return-to-work process facilitated return to work. Insufficient structure within the healthcare system and lack of support in daily life were perceived barriers to return to work, and need to be improved. These aspects should be considered in the return-to-work process after stroke.
Key words: stroke; return to work; healthcare; qualitative research.
Accepted Aug 14, 2019; Epub ahead of print Aug 28, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Gunvor Gard, Department of Health Sciences, Physiotherapy Research Group, Lund University, Lund, Sweden. E-mail: gunvor.gard@med.lu.se
To be able to return to work after stroke is important for health and well-being and participation in society. In this qualitative study, 20 stroke survivors were interviewed in focus groups about their experiences of healthcare-related facilitators and barriers. Perceived facilitating factors were a tailored rehabilitation content and a structured stepwise return-to-work process. A lack of sufficient early healthcare information, rehabilitation planning and coordination were perceived as barriers. An early rehabilitation plan, a contact person, and improved communication between rehabilitation actors were requested, as well as help with work transport, home care, children and psychosocial support for families. These aspects should be considered in order to improve the return-to-work process after stroke.
To be able to return to work (RTW) after stroke is important for health and well-being (1) and participation in society. In Sweden, approximately 23,000 persons have a stroke every year (2), 20% of whom are of working age. Stroke at a younger age leads to a substantial societal economic burden. The degree of disability after stroke is a strong determinant of economic cost. Concerning indirect costs for sick leave or disability pension, no clear relationship has been found between work absence and level of functional disability among stroke survivors aged 65 years or younger (3). The proportion of persons who RTW ranges from 19% to 73% (4), which indicates a need for an improved RTW process.
The United Nations (UN) declare that it is important to promote early RTW for persons with disabilities (5). RTW is a complex process, which can be facilitated or impeded by organizational, environmental or personal factors. Work climate, flexibility in work schedules and work adaptations, realistic occupational goals and availability of rehabilitation services have been shown to facilitate RTW. Also, flexible involvement of family, employers and co-workers, and personal factors, such as coping ability and motivation, facilitate RTW (1, 6, 7). Lack of cooperation between the clinical and employment sector and negative attitudes towards workplace adjustments from employers, as well as personal factors, such as stroke severity, fatigue and depression, are barriers to RTW (1, 6). Self-rated health 3 months after stroke has been shown to be strongly associated with RTW and a sustainable working situation after stroke (8).
In Sweden, acute stroke care is provided in stroke units and the majority of patients are discharged directly to their home. Primary care is the basis for long-term follow-up. The RTW organization of stroke patients in Sweden varies between hospitals, municipalities and County Councils. The new guidelines of the Swedish National Board of Health and Welfare advocate that all stroke patients should be followed-up by stroke professionals in a structured manner (9). In Sweden, the healthcare organization supporting patients after a stroke includes the whole rehabilitation chain from the hospital to the community. Four rehabilitation actors provide support for RTW in vocational rehabilitation (VR) in Sweden; the healthcare organization, the Social Insurance Office (SIO), the Employment Agency (EA) and employers (10). A labour union and an occupational health service may also be active in VR (10). The SIO determines whether an individual has the right to sick-leave and to coordinate resources for RTW. The employer has the responsibility to facilitate RTW according to the Swedish Working Environment Act. During this process, all stakeholders are involved, but do not always adequately cooperate with each other (10).
A review of qualitative studies regarding stroke patients’ perspectives concerning healthcare factors has shown that healthcare is fragmented, discharge services are poorly coordinated, and accessing health and social care in the community is difficult. The healthcare systems with which the patients interface and the interpersonal complexities they encounter must be improved in order to facilitate RTW (11). There is a need to transform the RTW approach so that services prioritize patients’ needs (12). Therefore, in-depth knowledge of stroke survivors’ experiences of healthcare-related facilitators and barriers to improve RTW is needed.
Aim
The aim of this study was to explore stroke survivors’ experiences of healthcare-related facilitators and barriers concerning RTW after stroke.
Patients discharged from the stroke unit at Skåne University hospital (SUS), who were on sick-leave due to the stroke onset, were referred to an outpatient stroke rehabilitation unit. Some patients underwent a multidisciplinary team assessment 4–8 weeks after stroke and, if needed, a multidisciplinary outpatient rehabilitation. Thereafter, they were referred to primary healthcare.
Participants
A convenient sample of 20 persons was selected from an on-going questionnaire study with the aim of identifying determinants for RTW after stroke. Participants fulfilling the following criteria were included in the questionnaire study: admitted to SUS for acute stroke care; aged 18–64 years at stroke onset; referred to outpatient stroke rehabilitation within 180 days after stroke onset, and were in employment for at least 10 h per week prior to the stroke. Persons not fluent in Swedish or with cognitive and/or language deficits that made them unable to answer the questionnaire were excluded. An invitation letter to take part in this interview study was sent to 39 persons who had answered the questionnaire between March and September 2017. Thereafter, they were contacted by telephone to confirm participation. Twenty-two persons agreed to participate and 17 declined or were unreachable. Two of the persons who initially agreed were unable to attend on the day of interview. A final total of 20 persons provided informed consent.
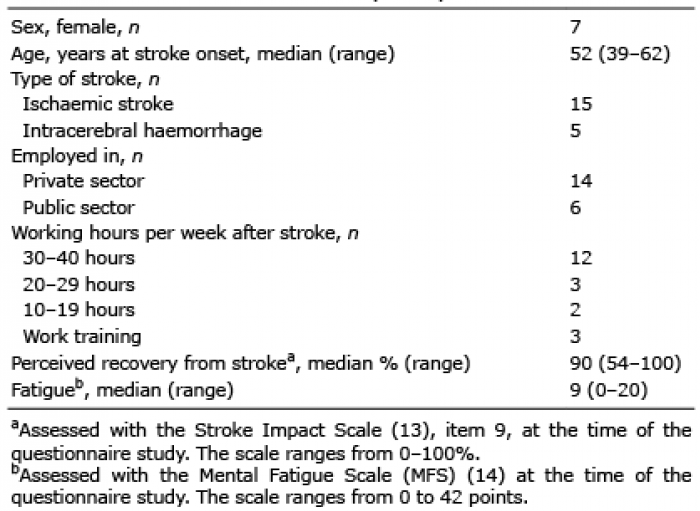
Table I describes the participants’ characteristics. Of the 20 participants, 15 had had a cerebral infarction while 5 had had an intracerebral haemorrhage. At the time of the interview, 16 persons had returned to their previous work. One participant returned to work for a few months and then retired shortly before the interview. Three persons were in work training, 2 of them had changed work due to the sequelae of the stroke, while the third person was in work training at the previous workplace. The participants perceived overall a good recovery from stroke, measured with the Stroke Impact Scale (SIS) (13). Fatigue, measured with the Mental Fatigue Scale (MFS) (14) was present in some participants.
Table I. Characteristics of the 20 participants
Qualitative interviews
The interviews were performed a median of 14 months post-stroke in focus groups to facilitate a group dynamic process with discussion between the participants (15, 16). By using focus group interviews, new research areas can be explored from the participants’ perspective (16). The study was designed in accordance with the COnsolidated criteria for REporting Qualitative research (COREQ) (17).
Procedure
In the interview guide, open questions were formulated based on earlier research and clinical experience. The main question was to describe various experienced facilitators and barriers to RTW related to healthcare. Follow-up questions were also used, such as “Can you tell more about that?” One of the authors (GG or IL) was the moderator and led the discussion. Three other researchers alternated as observers and asked supplementary questions. All had experience of stroke patients, but had not met the participants previously. The moderator endeavoured to create a trusting and supportive atmosphere to encourage all participants to share their views. The focus groups consisted of 3–5 participants and lasted for a median of 60 min (range 40–70 min). The discussions were audio-recorded and tran-scribed verbatim.
Analysis
The data were analysed using qualitative content analysis according to Graneheim & Lundman (15) in the following steps: first, the interview text was read as a whole and all content answering the research questions were identified as meaning units and categorized by 2 researchers (GG and IL) independently of each other. Thereafter, meaning units were identified, coded and sorted into subcategories and categories. A theme was also developed (15). The findings were discussed and validated several times between all authors. Quotations were inserted to validate the findings.
Ethics
The project was conducted in accordance with the Declaration of Helsinki (18) and approved by the Regional Ethics Review Board in Lund (Dnr 2016/1064). Written informed consent was obtained from all participants. Collected data were treated confidentially so that no individual could be identified.
In the analysis, an overall theme “Need for structured healthcare organization and support for return to work (RTW)” with 2 categories emerged: “Requesting rehabilitation planning, healthcare information and coordination”, and “Increased support in daily life would facilitate RTW”. The theme with categories and subcategories is described in Fig. 1. Each category and subcategory is described below with relevant quotations.
Fig. 1. Theme with cathegories and subcathegories.
Requesting rehabilitation planning, healthcare information and coordination
Adequate rehabilitation content and a stepwise RTW were facilitating factors, while insufficient communication between rehabilitation actors were barriers in the rehabilitation process. To improve the RTW process, the participants requested more information about stroke and its consequences and about regulations. Moreover, they asked for a rehabilitation plan in the early phase after injury, early contact with the rehabilitation unit, a contact person throughout the RTW process, and improved coordination between the rehabilitation actors.
Adequate rehabilitation content and timing facilitated return to work
RTW was facilitated by adequate rehabilitation content and timing. Positive experiences of rehabilitation interventions were, for example, interdisciplinary team rehabilitation or specific interventions, such as physiotherapy, cognitive behaviour therapy (CBT), mindfulness and consultations with occupational therapists and psychologists. Other facilitators were to be aware of the importance of rest to recover, to be responsive to bodily signals, but also to perform regular physical activity.
That’s [CBT] probably what has made it possible for me to increase my working hours now. I use mindfulness or guided meditation… and it helps. I’ve [also] been called up by an occupational therapist once a month and that’s been very good… to exchange ideas (Inf. 4).
Some participants reported that it was easier to receive rehabilitation for physical problems compared with psychosocial problems. A barrier to RTW was a lack of satisfactory psychosocial support. Continuing psychosocial support was needed, as was the opportunity to discuss RTW matters with others in the same situation. Concerning the timing, some wanted an early start to rehabilitation, while others needed a long period of rest prior to commencement of RTW.
I wish that there would be a therapy group for people who are in the same situation… how we can help each other, what kind of demands can I make at work. I would be open to that after 4 months, when I have come to terms with my situation a bit and it would’ve been OK to share it with others. Conversations would last for a while and later decline to every fourth or every sixth week[s] (Inf. 17).
I think you need more help mentally after some time than in the beginning… now the rumination starts (Inf. 5).
Moreover, they wanted support to deal with life as a whole; for example, psychological help to handle new priorities in the work situation. The participants also had comments on at which level of care the interventions should be offered.
…I should’ve received that kind of help [CBT] when I went home… it shouldn’t have been handled through the primary healthcare centre (Inf. 8).
Stepwise return to work facilitated the return to work process
A major facilitating factor for RTW was the ability to increase the working hours per week stepwise from 10 to 40 h/week. Without this stepwise process, it could be difficult to return to work.
But it was good that I could increase my working time, first part-time/half-time and then 75% and that was actually good… I did that for a few months. I took it easy when I came home [from work]. I didn’t do anything (Inf. 9).
To return to work early after stroke onset was perceived as a barrier, with negative effects.
In the beginning, I increased to 100% pretty quickly. And then my brain just shut down completely. So in reality, I needed a lot more time [sick leave] than I received (Inf. 4).
You’d need help that someone told you that “Don’t bother going to work. No matter how good you may be (Inf. 5).
Lack of early information, regular contact and a rehabilitation plan were barriers to return to work
A need for early information about stroke and its consequences, relevant regulations, early contact with a stroke rehabilitation unit, regular follow-ups, an early rehabilitation plan and a contact person were considered important, and were perceived as barriers if not provided. The participants requested information from healthcare professionals, from discharge and subsequently; for example, information about recovery as well as physical and mental fatigue.
…you’ve had very little information about, about what to expect… I have problems with my right hand… then I’m very… I get very tired as well. And that’s also – will that go away?...there’s no one who can really give an answer… I’ve never gotten any explanation (Inf. 1).
They also wanted information about relevant regulations.
We need a check list. “You’ve experienced a stroke: Think of this, do this, get in touch with the Social Insurance Agency”. You can’t take all of that in at once (Inf. 17).
To have brochures to inform employers and relatives about the disabilities after stroke was another suggestion to facilitate RTW. These could, for example, be a written text about hidden disabilities.
They [healthcare professionals] could provide some kind of information to various bosses, that we get tired and what happens in our brains. For there to be some kind of pamphlet to give to bosses…”here’s something to read up on so you’ll have some understanding” (Inf. 12).
Moreover, the participants suggested that a rehabilitation plan at an early stage after stroke onset and early contact with an outpatient stroke rehabilitation unit would facilitate RTW.
It would have been good to get a plan earlier. To receive [a rehabilitation] contact earlier (Inf. 9).
I would’ve liked to have had contact with [the stroke rehab] immediately (Inf. 17).
To get a professional contact and coaching directly after discharge and support further on during the process could also facilitate RTW.
Just to go and talk to someone that “now it’s like this” in a month you’ll be called to this” and so on. To know what’s gonna happen (Inf. 11).
You should get some kind of contact person… someone who calls and checks on you “how is it now, are you experiencing any problems?” could refer you to, well, here or there (Inf. 3).
I probably would’ve liked coaching support (Inf. 8)
… the absolute best thing would be to have an appointment with a counsellor immediately after discharge. Because there you talk about everything like work and help at home (Inf. 5).
The participants perceived a lack of regular follow-ups from the rehabilitation professional as a barrier to RTW. Another barrier was that each individual had to contact the primary care themselves for the follow-ups.
…nobody mentioned anything about follow-ups, having to call them myself and ask for a follow-up (Inf. 5).
[I would’ve liked] a follow-up from the healthcare “is it going in the right direction” a confirmation that something has been helpful and that we’re on the right track (Inf. 12).
However, some participants were content.
Everything has gone by itself automatically, like they [the hospital] had already planned how it was going to be (Inf. 12)
… instead, I asked myself “is this really necessary? I’m content. But had it been a more serious situation, I don’t know what I would’ve said (Inf. 13).
Insufficient communication between rehabilitation actors hindered return to work
Insufficient communication and coordination between healthcare professionals and rehabilitation actors (hospital, rehabilitation unit, primary healthcare, social insurance company); for example, regarding prescriptions and length of sick leave were barriers to RTW. Repeated short periods of sick leave were stressful and different physicians had different opinions about the length of sick leave.
There should’ve been someone to coordinate information to the Swedish Social Insurance Agency, to work, a contact person who helps me, who speaks for me and helps me with for example compensation from insurances.[It would be nice if] all information was in one and the same place, to get it from one source only (Inf. 16).
The physicians here at the hospital did not agree with the stroke rehab physicians about when I was going to start working (Inf. 5).
I had to run back and forth to the primary healthcare centre to get [the sick leave] renewed… it was very stressful (Inf. 4).
Increased support in daily life would facilitate return to work
Lack of support in daily life, such as help with work transport, practical help in the home situation and psychosocial support for the families were perceived as barriers. The participants suggested that increased support could facilitate RTW.
Work transport problems impeded return to work
Transport to and from work were barriers to RTW for those who had driving restrictions after stroke, for those without access to public transportation and for those who had long walking distances to public transportation. Some participants were allowed to drive, but did not have the energy to drive longer distances. Problems with work transport could be reduced by working from home.
I wasn’t allowed to drive a car, which immediately led to long days when you had to take the bus and it was a long walk to the bus. I thought that was the worst part, getting to and from work (Inf. 6).
Lack of practical help and psychological support for the family were barriers to RTW. Home care barriers to RTW were also expressed, such as lack of help with housework and children and need for psychological support for the family.
There was no support [from society or other], so my wife had to take care of every single thing at home. Had I been alone with the kids, I wouldn’t have been able to go back to work (Inf. 8).
I’m alone in my household. It’s difficult for me to manage a full-time job and to take care of the entire home (Inf. 6).
I did get help from a psychologist. But my family! They don’t get any questions about support (Inf. 8).
But I would’ve liked support for my family, for my kids, who still think it’s a bit traumatic… to [get help with] explaining to the kids… that somebody else had taken care of everyone in the family (Inf. 17).
The aim of this study was to explore stroke survivors’ experiences of healthcare-related facilitators and barriers to improve RTW after stroke. When analysing the data from the participants, a theme, “Need for structured healthcare organization and support for RTW” with 2 categories, “Requesting rehabilitation planning, healthcare information and coordination” and “Increased support in daily life would facilitate RTW” emerged as the result. Facilitating factors expressed were a tailored rehabilitation content with effective treatments, adequate timing and a structured stepwise RTW process. A lack of sufficient early healthcare information, rehabilitation planning and coordination were perceived as barriers. An early rehabilitation plan, early contact with the rehabilitation unit, a contact person, and improved communication between rehabilitation actors were requested. Increased support in daily life, including transport to and from work, home care and psychosocial support for the families were also requested.
Adequate rehabilitation content and timing facilitated RTW according to the first subcategory within the category “Requesting rehabilitation planning, healthcare information and coordination”. To receive a rehabilitation content tailored to the patients’ needs was experienced as a facilitator. Interdisciplinary rehabilitation, physiotherapeutic interventions, and psychosocial support were examples of facilitative treatments for RTW. The opportunity to rest and recover, to be responsive to bodily signals, but also to perform regular physical activity, were also mentioned as facilitators. The rehabilitation has to be coordinated with vocational rehabilitation (10, 19, 20). However, not only the content of the rehabilitation, but also the timing was important for RTW. Early psychosocial support was requested, but also support after a while, when new questions about the future arose. A competent rehabilitation professional may be responsible for providing such support, knowledge and opportunities for group discussions. Earlier research has confirmed the importance of psychosocial information, motivational support and practical advice (20). It is important that RTW programmes address psychosocial aspects (21, 22).
The second subcategory, “Stepwise return to work facilitates the RTW process” was described as a successive increase in working hours per week and was experienced to facilitate RTW. Those who had such a stepwise process were satisfied with it. They perceived that advice clarity about sick leave and to learn a step-by-step RTW according to one’s capacity helped them. In order to facilitate work performance after stroke, Burns and co-workers (23) recommend performance-based assessments, specific evaluations of work activities and work environment, education and interventions that include employer collaboration. Flexible work schedules are recommended by Hartke and co-workers (24). Education and assessment of work ability are important to facilitate RTW according to Hellman and co-workers (10). A job analysis can be a first step in a stepwise RTW process (10) and supply the rehabilitation team and employers with early knowledge and factual information about each patient. Suitable organization platforms at work where all rehabilitation actors can cooperate are also of importance for RTW (20).
A stepwise RTW implies a rehabilitation plan that could be revised several times (25). Also, all rehabilitation actors need adequate training and improved awareness of best practice guidelines to help stroke patients in their stepwise process to RTW (26, 27).
The third subcategory showed that the participants wanted early information, an early rehabilitation plan, early contact with the rehabilitation unit, a contact person and regular health contacts in order to improve RTW. Information about healthcare issues, stroke and its consequences, as well as knowledge about hidden disabilities, such as overload of sensory stimuli, cognitive impairments and fatigue, were requested. Today in Sweden, the hospital stay has been shortened and may be only a few days. This may mean that hidden disabilities may not be discovered until later at home when life and work demands increase.
Early information may lead to a clearer picture of the person’s abilities and limitations and facilitate the RTW process according to the fourth subcategory. With improved knowledge, patients can, in their turn, provide improved information to their employers, co-workers and relatives, who may also need stroke-related information (10, 21). Brochures and e-health tools (28) can be developed to inform employers, relatives and other stakeholders about the consequences of stroke. Relevant information can be given to employers at re-activation meetings, and relatives can be informed at structured follow-ups. A rehabilitation plan, based on the International Classification of Functioning, Disability and Health concept (ICF) (29) has been shown to encourage and increase participation in the rehabilitation process. Such a rehabilitation plan should be developed in the early phase and follow the patient throughout the process. A contact person to provide psychosocial support and coordination in the RTW process was asked for, a need also described earlier (10, 20). Such a contact person may also share early discussions of work-related issues with patients, employers and relatives, which may facilitate RTW (10, 20). Moreover, regular healthcare contacts were believed to facilitate RTW and these contacts could be arranged by organizing structured follow-ups, which are recommended by the national guidelines from the Swedish National Board of Health and Welfare (9). Another perceived barrier to RTW was insufficient communication and coordination between rehabilitation actors. The participants requested improved communication within the hospital care, as well as communication and coordination between the hospital and primary healthcare. The rehabilitation plan and the designated contact person discussed earlier can also be used as a communicator to facilitate improved interaction between the healthcare actors. Regular meetings between all stakeholders can facilitate coordination of the VR, potential work adjustments and future planning.
In the second category, it was described that increased support in daily life would facilitate RTW. Transport problems to and from work, as well as practical help and psychological support for the family were perceived as barriers to RTW. The participants had difficulties in managing both work and home tasks. Transport was a barrier to RTW for those who had driving restrictions after stroke or those lacking public transport or with long walking distances. Research indicates that the inability to drive a car may be a barrier to RTW (23). An interdisciplinary practice model for adults with mild stroke has been developed to enable successful return to driving and work. The model can be used in community rehabilitation to support recovery, transition, adaptation and community reintegration (23).
The participants emphasized that lack of practical help with household chores and children, as well as psychosocial support for the family, were barriers to RTW. These aspects have, to our knowledge not been highlighted previously. Psychosocial family needs may be addressed in professional counselling, as well as in a virtual context (23) by, for example, video communication, smart phones or apps. We suggest that community support services should be developed and include stroke survivors’ family situation and children. To further optimize RTW, community support services should be integrated with the process. Education by healthcare professionals to relevant stakeholders in society may improve the situation. After referral and relevant evaluations, persons with mild stroke can receive necessary community support, for example practical help with housework and children, to be able to return to work in accordance with the recommendations in the interdisciplinary practice model (23). Family members and relatives may also need to be informed about disabilities following stroke, such as cognitive limitations and fatigue, in order to understand the consequences of stroke in daily life more fully and thereby be more supportive in the RTW process.
Methodological discussion
A strength of the study was that the 20 informants volunteered to participate in the focus groups because of their interest in sharing their experiences, which they described freely during the interviews. Therefore, the data became rich. The study had clear inclusion criteria and obtained variety regarding age, sex, socio-cultural background, disability and type of work. The interviewers were familiar with performing both focus group interviews and qualitative content analysis.
Credibility refers to the researchers’ ability to capture the reality (30). All the researchers had earlier experience of working with qualitative methods and had a long-term understanding of stroke rehabilitation. The researchers worked close to the text in the analytic process and description of the results, which ensured confirmability according to Öhman (30). Triangulation was performed by the researchers. Dependability refers to the relationships between informants and researchers in terms of being interrelated and having had professional interaction with each other (30). The researchers had no earlier relation to the informants. All researchers had a pre-understanding of stroke, which may have influenced both the way the questions were formulated, and the analytic process. However, the results were grounded in the data and the analysis was performed close to the text. Concerning transferability, the knowledge obtained from this study may be transferable to similar contexts in other populations. Persons not fluent in Swedish or with severe cognitive and/or language deficits were excluded due to the study design. However, exclusion of these persons is a study limitation. Another limitation is that all participants had RTW or were work training and we thus lacked information from those who did not RTW.
Conclusion
A tailored rehabilitation content and a structured stepwise RTW process facilitated RTW. Insufficient structure within the healthcare system and lack of support in daily life were perceived barriers and need to be improved. These aspects should be considered in the RTW process after stroke.
Financial support was received from the Färs and Frosta Foundation, the Promobilia foundation, the Swedish Stroke Association and the Norrbacka-Eugenia foundation.
The authors are grateful to the individuals who volunteered to participate and to RPT, PhD Michael Miller for language editing and Camilla Andersson, Sanna Forsgren and Ann Nilsson for help with collecting the background data.


 Click to show fullsize
Click to show fullsize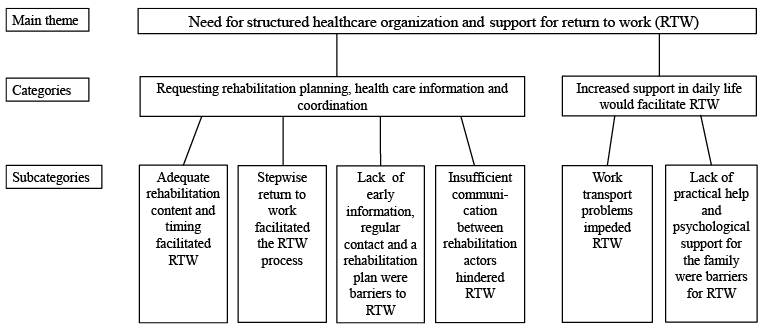 Click to show fullsize
Click to show fullsize