
From the 1Respiratory Care Service, University Hospitals of Geneva, Geneva and 2Institute of Sport Sciences of the University of Lausanne, Lausanne, Switzerland
Background: The outcome of surgery in deconditioned patients can be improved through prehabilitation. This study examined the effect of prehabilitation in patients diagnosed with lung cancer.
Methods: Candidates for lung cancer resection were assigned to high-intensity interval training (n = 74) or usual care (n = 77). Cardiopulmonary exercise testing and 6-min walk test were performed before and after training. High-intensity interval training consisted of 2–3-weekly, 2 × 10-min series of cycling at peak power, measured with cardiopulmonary exercise testing prior to training, with a 15-s on-off duty cycle, preceded by a 5-min warm-up and followed by a 5-min cool-down. Work-rate, heart-rate, saturation, dyspnoea and leg effort were monitored.
Results: Waiting time (median 25 days) allowed a median of 8 high-intensity interval training sessions to be performed. Adherence to mean high-intensity interval training was 87% (18% standard deviation; SD). High-intensity interval training power increased (23 watt, 95% confidence interval (95% CI): 20–26 watt), as did heart rate (14 bpm, 95% CI 11–16 bpm). Resting heart rate (–6 bpm, 95% CI –4 to –7 bpm) and heart rate 1 min post-cool-down decreased (–5 bpm, 95% CI –4 to –7 bpm). Aerobic capacity increased after high-intensity interval training (14%, 95% CI 3–26%), as did peak power output (median 7%, 95% CI 2–13%), but not after usual care. Six-min walk test score increased after high-intensity interval training (median 20%, 95% CI 14–26%), but not after usual care.
Conclusion: Short-term high-intensity interval training is feasible in deconditioned patients and increases cardio-respiratory fitness and walking capacity.
Key words: exercise; neoplasm; thoracic surgery; lung; prehabilitation; high-intensity interval training; HIIT.
Accepted Aug 13, 2019; Epub ahead of print Aug 29, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Bengt Kayser, Institute of Sport Sciences of the University of Lausanne, Synathlon, Uni-Centre, 1015 Lausanne, Switzerland. E-mail: bengt.kayser@unil.ch
High-intensity interval training is used increasingly in patient care. Various training patterns are used. For patients diagnosed with lung cancer, the first choice intervention is surgery. There is a wait of approximately a mean of 3 weeks between the clinical decision to operate and the intervention. A high-intensity interval training protocol was designed, to be performed during this time-window, to improve the physical condition of these patients before surgery. Patients cycled 3 times per week under supervision, performing 2 × 10-min series of 15-s sprints at peak power, interspersed with 15-s pauses. Compared to usual care, just before surgery, after 8 sessions of high-intensity interval training, the patients’ physical fitness was significantly improved while after surgery the outcome was improved.
A potential curative option for early-stage non-small cell lung cancer (NSCLC) is primary lung resection (1). However, physical deconditioning is a major risk factor for patients undergoing surgery, and low peak oxygen uptake (VO2peak) is a predictor of perioperative mortality and cardiopulmonary morbidity (2, 3). A VO2peak cut-off of 16 ml/kg/min and an anaerobic threshold VO2 cut-off of 10–12 ml/kg/min can distinguish between low- and high-risk for major postoperative complications (4). Pre-operative improvement in fitness (i.e. prehabilitation) is therefore clinically relevant. Prehabilitation reduces imminent risk prior to surgery and improves operative recovery and outcome (5). It also improves VO2peak, muscle strength and quality of life (6). Different prehabilitation programmes for patients with NSCLC have been evaluated, in home-based, out- and in-patient settings, using strength exercise, continuous and interval training on a cycle ergometer or treadmill, breathing and coughing exercises, and specific inspiratory muscle training (7–13).
Inspired by the use of interval training by athletes, short high-intensity intervals of activity, interspersed by recovery periods, so-called high-intensity interval training (HIIT), are used increasingly in patient care (14, 15). HIIT refers to series of repeated sessions of efforts close to, or even over that corresponding to, peak aerobic power (Wpeak), interspersed by active or passive recovery periods. The duration of these repeated bouts of effort varies and can last between 10 s and several min, with varying recovery periods in between.
Previously, we designed a randomized clinical trial (RCT) protocol with specific short-term pre-operative HIIT for patients with stage IIIA NSCLC. In the publication reporting the clinical results of this RCT the HIIT training protocol was not presented in detail (16). We therefore present here the proof-of-concept of the specific HIIT protocol used in the earlier RCT so that the method can be replicated. The feasibility of short-term HIIT was tested in deconditioned patients with NSCLC in the pre-operative period and the effects on aerobic capacity (VO2peak) and the 6-min walk test (6MWT) were quantified. The time-window for prehabilitation was from the time a decision was made to perform surgery until the actual surgery. This 2–3-week period, used for preoperative examinations and logistics, cannot be reduced in our setting and thus provided an opportunity for prehabilitation.
The HIIT protocol was inspired by a study in cardiac rehabilitation, reporting that HIIT at Wpeak was feasible and safe in deconditioned patients with chronic heart disease (17). Since many patients with NSCLC smoke and experience dyspnoea on exertion, we expected that this particular HIIT might limit the extent of dyspnoea during training. Our hypotheses were that candidates awaiting primary lung resection surgery for NSCLC would be able to perform such HIIT despite deconditioning, and that it would improve Wpeak, VO2peak, resting heart rate (HRrest), heart rate recovery (HR1min), dyspnoea and exercise capacity in these patients.
Design
The study was a registered PROBE trial using assessor blinding and intention to treat analysis (ClinicalTrials.Gov: NCT01258478 (16)). Following protocol approval by the Geneva University Hospitals ethics committee (protocol 06-225), informed written consent was obtained from patients with suspected or proven NSCLC stage IIIA or less. Consenting patients were randomized 1:1 into usual care (UC) or prehabilitation (PH)) using permuted blocks of 4. The randomization sequence was generated before the trial began and was kept concealed until the end of the study. Exclusion criteria were contraindications to perform cardiopulmonary exercise testing (CPET) (uncontrolled cardiac disease, severe pulmonary hypertension, uncontrolled asthma) (18) and limitations to adhering to the rehabilitation programme; for example, difficulty cycling.
Exercise testing
The primary study endpoint was pre- to post-prehabilitation aerobic capacity change. After enrolment, patients performed CPET according to ATS/ERS standards (American Thoracic Society and European Respiratory Society) (18) on an upright electronically braked ergometer (Ergoline GmbH, Germany). Gas exchange was measured breath-by-breath with a metabolic cart (Sensor Medics Model 2200 SP, Yorba Linda, CA, USA). In these severely deconditioned patients the usual maximum criteria could not be used and subjective exhaustion was the main reason for cessation of the test. VO2peak was determined as the highest mean VO2 over 20 s and Wpeak was defined as the highest power maintained for 20 s (19). The ventilatory threshold (AT) was determined with the V-slope method as primary criterion and the first rise in the ventilatory equivalent for oxygen (VE/VO2) as secondary criterion (20). CPET was repeated the day before surgery. At enrolment the patients performed a 6MWT according to ERS and ATS guidelines, repeated just prior to surgery (21).
High-intensity interval training
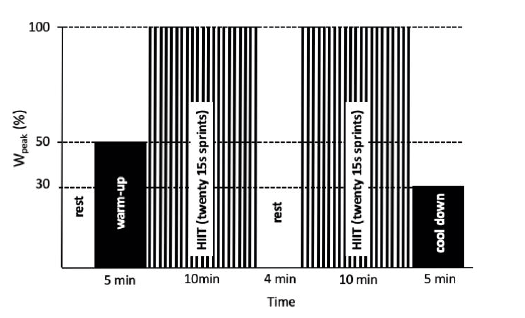
HIIT was performed between the decision for resection and its realization. For logistic reasons this period lasts 2–3 weeks in our setting. However, the waiting time for surgery was not prolonged in order to accommodate prehabilitation. Experienced respiratory physiotherapists supervised HIIT in personalized sessions (1–3 patients at a time), 3 times a week. Patients breathed room air throughout (no supplementary oxygen). HIIT was performed on an upright electromagnetic cycle ergometer (Motion Cycle 500, Emotion Fitness GmbH, Hochspeyer, Germany). Seat height was adjusted, and foot buckles ensured safety and comfort. The pedalling rate was 60–70 revolutions per min (RPM). After a 5-min warm-up at 50% Wpeak, patients performed HIIT, consisting of 15-s sprints at 100% Wpeak interspersed by 15 s of passive resting periods, for 2 series of 10 min, with a 4-min rest period in between. This was followed by a 5-min cool-down at 30% Wpeak (Fig. 1). The modified Borg Scale (0–10) was used to quantify dyspnoea and leg fatigue.
During HIIT the patients were verbally encouraged. Sessions lasted approximately 30 min, but could be terminated prematurely upon strong dyspnoea, cardiac arrhythmia, or if the patient did not feel well enough to complete the session. Initial HIIT power output was set at 100%Wpeak, as measured during the CPET after intake. If the patients were unable to complete sessions at 100%Wpeak the power was lowered according to their capacity to obtain a dyspnoea and leg fatigue of at least 5 Borg scale (i.e. less than “severe”). Power was increased again if dyspnoea or the sense of effort decreased below 5. An upper limit of 7 for dyspnoea and leg fatigue was set (corresponding to “very severe”). Work rate was adjusted each session as Borg ratings and HR evolved, to target CPET-determined HRpeak at the end of sessions.
Fig. 1. Overview of the high-intensity interval training (HIIT) paradigm. After 5-min warm-up at 50% Wpeak the participants performed 2 × 10-min blocks composed of 15-s sprints at 100% Wpeak interspersed by 15-s pauses, and a 4-min pause between the 2 blocks. A cool-down period of 5 min at 30% Wpeak completed the training.
Measurements
Prior to HIIT, while quietly seated on a chair (5 min), resting heart rate (HRrest), resting dyspnoea (Dysprest, Borg 0–10 scale), and resting saturation (SpO2rest) were measured. During HIIT, HR, SpO2, dyspnoea, and leg fatigue sensation (Borg 0–10 scale) were monitored. The measurements were taken at the end of warm-up, during HIIT (highest HR, HRsession) and 1 min after the cool-down period (HR1min). SpO2 and HR were measured with a finger pulse-oximeter (Rad-5, Masimo Corporation, Irvine, CA, USA).
Data analysis
For each patient, data for the first, middle and last HIIT training sessions were extracted and analysed. Data were analysed using Stata (v. 12), R (v. 3.3.2) and Prism (v. 8). Results were analysed using Student’s t-test, Mann–Whitney test and linear mixed effect models with a random effect on subject and a fixed effect on time for Wpeak, HRrest, HRsession and HR1min. Normality of data distribution was checked visually. Data are presented as means (with 95% confidence interval; 95% CI), medians (with interquartile range; IQ25–75%) or means (with SD). The alpha-level was set at 0.05.
Patients
A total of 189 patients were screened, 164 provided consent and 13 were excluded. Data for a final total of 151 patients were available for analysis; 74 PH and 77 UC. The period from enrolment until surgery was similar in the 2 groups (PH: median 26 days, IQ25–75%, 21–33 days; UC: median 25 days, IQ25–75%, 20–40 days). Adherence to the prescribed training sessions for PH was 87 ± 18% (median 8 sessions, IQ25–75%, 7–10 sessions). No adverse events were reported during the training programme. Baseline characteristics of the patients are shown in Table I. The 2 groups did not differ for preoperative patient characteristics (see 16).
Table I. Baseline characteristics of the study population
High-intensity interval training sessions
There were no significant differences for any of the measured variables between the first and the intermediate training sessions, except Wsession, which increased (mean difference 11 watt, 95% CI 8–13 watt, p < 0.001) and HRsession, which increased (mean difference 8 bpm, 95% CI 6–11 bpm, p < 0.001) (see Fig. 2).
Fig. 2. High-intensity interval training (HIIT) sessions 1–3. Resting heart rate prior to the training (HRrest,/min), power output during training (Wsession, watt), heart rate reached during training (HRsession,/min), 1-min recovery heart rate (HR1min,/min), dyspnoea (Borg 1–10) and leg fatigue (Borg 1–10). Boxes represent the 25–75% percentiles, whiskers represent the Tukey range, and lines in the box represent the median values of the distribution.
Wsession increased between the first and the last session (mean difference 23 watt, 95% CI 20–26 watt, p < 0.001). This was accompanied by a significant increase in HRsession (mean difference 14 bpm, 95% CI 11–16 bpm, p < 0.01). HR1min decreased significantly (mean difference 5 bpm, 95% CI 4–7 bpm, p < 0.001).
Dyspnoea sensation increased significantly from the first to the last session (mean difference 0.8 points, 95% CI 1.2–2.1 points, p < 0.001). Leg fatigue also increased significantly (mean difference 0.8 points, 95% CI 1.4–1.8 points, p < 0.001).
Overall, there was a decrease in HRrest and in HR1min between the first and the last training sessions, whereas Wsession and HRsession increased. There were no statistically significant effects of sex, age or body mass index (BMI) on the evolution of HRrest. The higher baseline HRrest at the start, the greater was the decrease in HRrest in the final session. The decrease in HRrest in the final session amounted to a mean of –2 bpm (95% CI –1 to –3 bpm, p <0.001) for an increase in 10 bpm HRrest at baseline (see Fig. 3).
Fig. 3. Reduction in resting heart rate after 3 weeks of high-intensity interval training (HIIT) (delta HRrest) as a function of baseline resting heart rate (HRrest).
Evolution of Wsession was not significantly affected by age, sex or BMI. There was a trend for an elevated baseline Wsession to be associated with a greater increase in Wsession. The increase in HRsession between the first and the last sessions was negatively associated with its baseline value and with age. The higher HRsession at the start, the lower the increase in the final session. With increased age HRsession increased less with training. The increase in HRsession dropped by a mean of 0.3 bpm (95% CI 0.1–0. 6 bpm, p = 0.014) per year.
Fitness and exercise capacity
There was significant decrease in HRrest from the first to the third sessions (mean difference –6 bpm, 95% CI –4 to –7 bpm, p < 0.001). Significant changes in CPET and 6MWT were observed at the end of the intervention for the PH group. There was a significant increase in VO2peak (median 14%, 95% CI 3–26%, p = 0.004), and in Wpeak (median 7%, 95% CI 2–13%, p < 0.01). There was a significant increase in the walking distance of the 6MWT (median 20%, 95% CI 14–26, p < 0.001) (Table II).
Table II. Changes in cardiopulmonary exercise testing (CPET) and 6-min walk test (6MWT) parameters for the usual care and prehabilitation groups in the preoperative period (deltas)
Cardiopulmonary exercise testing variable associations in the prehabilitation group
The Wpeak was higher in men compared with women (mean difference 13 watt, 95% CI 3–23, p = 0.010). There was a lower increase in Wpeak with an increase in age (the increase reduced by 0.58 watt per 1 year increment in age). There was less increase in Wpeak in patients with a higher baseline Wpeak (the increase reduces by 0.17 per increment of 1 watt in initial Wpeak)
The HRpeak during CPET was significantly lower in women compared with men (mean difference 7 bpm, 95% CI 1–13 bpm, p = 0.018).
The objective of this paper was to report the design, application and efficacy of a particular HIIT paradigm to improve cardiorespiratory fitness in deconditioned patients with lung cancer. Our hypotheses were that candidates awaiting primary lung resection surgery for NSCLC would be able to perform such HIIT despite deconditioning, and that HIIT would improve aerobic power output (Wpeak), aerobic capacity (VO2peak), resting heart rate (HRrest), recovery heart rate (HR1min), dyspnoea and exercise capacity (6MWT) in these patients. We found that the particular HIIT paradigm was well supported by this group of patients and that a median of only 8 training sessions significantly increased VO2peak and Wpeak. During the preoperative waiting period (median 25 days), VO2peak and 6MWT both increased by 15%, while they declined in the UC group.
Given that VO2peak is an important predictor of outcome for patients with NSCLC this finding is encouraging (2, 3). Not only VO2peak, but also 6MWT, was increased suggesting that the increase in aerobic power potentially translated into better exercise capacity in daily life settings. We previously published the clinical impact of this particular intervention on surgery outcome (16). The pulmonary complications, mainly atelectasis, were reduced by 45% in PH and the effect was more pronounced in patients who demonstrated a greater response to HIIT. This resulted in a mild reduction in the length of stay in the post-anaesthesia care unit (median –7 h, IQ25–75% –4 to –10 h) (16).
Our finding that just 8 training sessions over 3 weeks resulted in a significant improvement in fitness is in agreement with earlier work. HIIT was shown to result rapidly in positive aerobic effects; just 6 sessions of HIIT can produce these changes due to an increase in the mitochondrial content, thereby enhancing oxygen uptake (22). Several meta-analyses of controlled trials also confirmed that HIIT increases VO2peak and that the effect is greater for candidates who are less fit (14, 23). In addition, HIIT improves fitness in patients with severe heart disease (17).
At baseline the mean VO2peak and mean 6MWT distance were 18% and 42%, respectively, below the predicted values in these patients (16). It has been shown that cardio-respiratory fitness is an independent factor in mortality and length of hospitalization (24). In individuals undergoing non-cardiac surgical procedures high levels of preoperative function, in particular higher cardio-respiratory fitness, are associated with better survival after surgery (24–26). Due to the design of the current study it was not possible to include only severely deconditioned patients. However, it is possible that the more severely deconditioned patients could benefit the most, as suggested by the observed changes in resting heart rate.
Resting heart rate (measured in standardized conditions) was lowered as a result of the exercise training in our patients. A low resting heart rate is characteristic of a higher fitness level and is a predictor of all-cause mortality (27). It was demonstrated that HIIT improved resting heart rate more than did other modes of training in patients with coronary artery disease (28). Numerous trials have shown a mean decrease in resting heart rate of 3–10 bpm after HIIT training, conducted for 8 weeks, 12 weeks or 6 months, at 60–90% of Wpeak (29, 30). We saw a mean reduction in resting heart rate of 6 bpm after a median of 8 HIIT sessions at 100% of Wpeak. Since there was no significant change in HRrest between the first and the intermediate HIIT sessions, it can be assumed that it takes approximately 2–3 weeks to notice the first changes with this type of HIIT paradigm.
Exercise is associated with increased sympathetic and decreased parasympathetic activity and the period of recovery after maximum exercise is characterized by a combination of sympathetic withdrawal and parasympathetic activation. A mean extra resting heart rate recovery of –5 bpm was observed 1 min after cool-down in our patients. Heart rate recovery (HRR) after strenuous exercise has been shown to be more rapid among individuals with higher levels of fitness and following aerobic training programmes in a variety of adult and paediatric populations (31, 32). HRR is thought to represent both the restoration of parasympa-thetic input and the withdrawal of sympathetic tone after exercise; it may therefore be an indicator of changes in fitness level and overall training status (33).
Increased vagal activity associated with a faster HRR has been shown to be associated with a decrease in risk of death (34). In a systemic view it was found that HRR is considerably reduced after an aerobic exercise programme in patients with established heart disease (35). It was also demonstrated that HRR at 1–2 min recovery is a prognostic measurement (36). Further study is required to determine whether a mean extra reduction of 5 bpm in patients with NSCLC is of physiological importance with regards to a short-term rehabilitation programme. The HRR in our patients did not improve between the first and intermediate HIIT sessions, and the changes were seen only for the final session in comparison with the first session. In the later HIIT sessions the patients were well accustomed to exercise and they were exercising at higher intensities, with a significant increase in HRsession, dyspnoea and leg fatigue ratings. It is possible that the HRR changes occurred at the end because of the higher intensities of work, which demanded much more cardio-respiratory effort, and also that a training programme requires time to result in measurable changes. These findings also suggest that these deconditioned patients may not have been able to reach their “true” maximum aerobic capacity during the first CPET.
This study was performed with lung cancer patients awaiting surgery. The study took advantage of this important time-window of opportunity to assess whether exercise can have an important role in cardiorespiratory fitness in such a short time, as well as motivating patients to play an active role in their well-being (5). A systematic review of 18 pre-surgical exercise protocols suggested functional and clinical benefits, which are extremely important in cancer care, and pre-surgical exercise can therefore be considered as a potential adjuvant therapy (37). The American College of Sports Medicine clearly states in its guidelines for cancer survivors that exercise is safe in the pre-operative and post-operative periods, and leads to improved physical functioning and better quality of life (38).
The challenge in this trial was to maintain adherence despite the fact that some patients had marked deconditioning and highly sedentary levels. Twenty-two percent of the patients had an ASA score of 3–4 (patient has severe systemic disease that is not incapacitating, or patient has incapacitating disease that is a constant threat to life) (39). Adherence is a major limitation in any study using exercise as an intervention. It is imperative to have an exercise protocol that is enjoyable, especially because waiting for a potential life-saving operation is very stressful. There are several studies suggesting that HIIT is perceived to be more pleasurable even if it is more physically demanding than a moderate intensity exercise regime (40). Even though it was not systematically evaluated, we observed that our patients’ satisfaction and motivation improved from the first to the last sessions as the date of surgery approached. The patients who received prehabilitation also seemed to remain more active and motivated to get back to a fitter state in the post-operative period.
It would therefore be interesting to combine a prehabilitation HIIT regime with a post-operative rehabilitation programme to determine if the benefits obtained are maintained for a longer time and what influence it has on the quality of life of the patients. Combining or replacing a lower-body HIIT with an upper-body HIIT could also be interesting for patients who have lower limb impairment. Although 30% of the patients in the rehabilitation group had chronic obstructive pulmonary disease with dyspnoea at rest, and effort was a challenge, the training was well tolerated, indicating the possibility of its regular application in pulmonary rehabilitation programmes. It would be important to combine such training with nutrition coaching and psychological support for the patients in future studies in order to maximize the results.
Conclusion
A short-term HIIT paradigm using 15-s sprints at 100% Wmax is feasible and safe in the pre-operative period and increases cardio-respiratory fitness in patients with NSLCC.
This study was supported by the Clinical Research Centre of the University Hospital of Geneva and the Geneva Association Against Cancer. Methodological support was given by the Clinical Research Center, University of Geneva and Geneva Hospitals, Antoine Poncet. We also thank all the collaborators that made the study possible (16).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize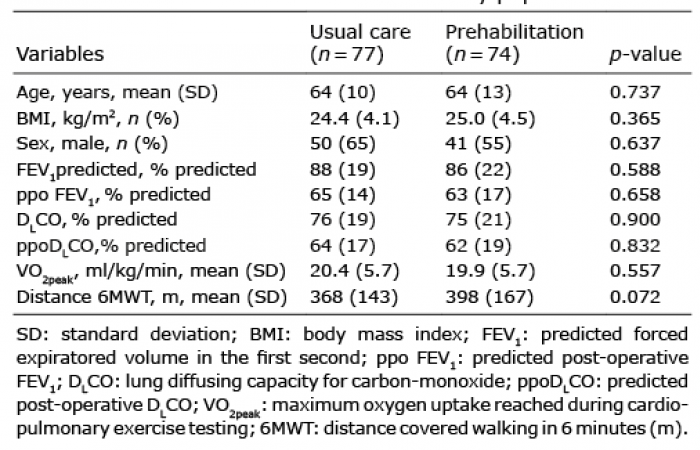 Click to show fullsize
Click to show fullsize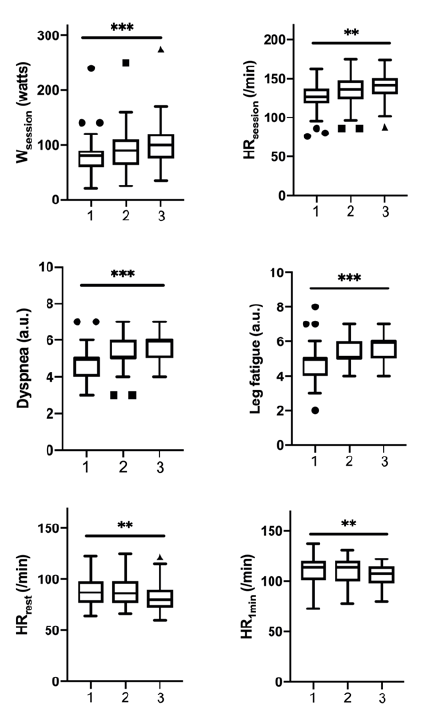 Click to show fullsize
Click to show fullsize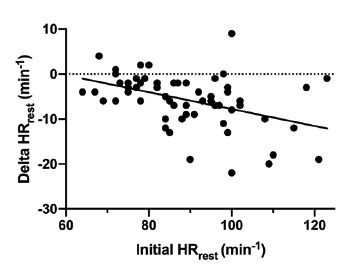 Click to show fullsize
Click to show fullsize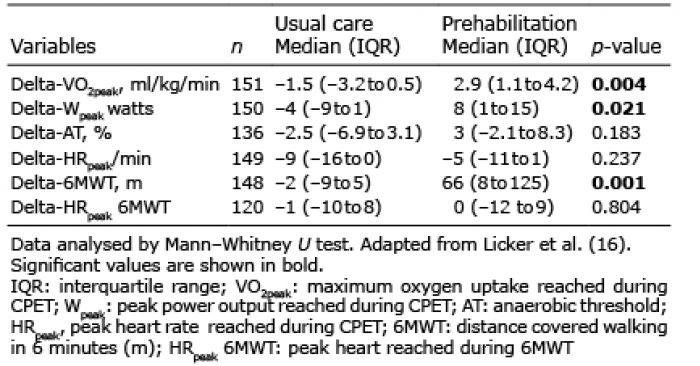 Click to show fullsize
Click to show fullsize