
From the 1Department of Emergency and Critical Care Medicine, Hitachi General Hospital, Ibaraki and 2Department of Emergency and Critical Care Medicine, The University of Tokyo Hospital, Tokyo, Japan
Objectives: Belt electrode skeletal muscle electrical stimulation can induce muscle contraction of the whole lower body. This study examined the efficacy of belt electrode skeletal muscle electrical stimulation on reducing loss of muscle volume in critically ill patients.
Methods: Intensive care unit patients were randomly assigned to control and electrical muscle stimulation groups. In both groups, early rehabilitation was administered from day 2 of admission. In the electrical muscle stimulation group, belt electrode skeletal muscle electrical stimulation was administered. Femoral muscle volume was evaluated with computed tomography on days 1 and 10.
Results: Ninety-Four severely ill patients were included 47 patients were assigned to each group. Femoral muscle volumes of 16 control and 21 electrical muscle stimulation group patients were measured. For both groups, femoral muscle volume decreased significantly from day 1 to day 10 (p < 0.0001). The mean rate of muscle volume loss was 17.7% (standard deviation (SD) 10.8%) for the control group and 10.4% (SD 10.1%) for the electrical muscle stimulation group (p = 0.04). The score for stair-climbing of Barthel Index was significantly better in the electrical muscle stimulation group 3.9 (SD 4.0) than in the control group 1.5 (1.5) (p = 0.04).
Conclusion: Belt electrode skeletal muscle electrical stimulation has the potential to inhibit muscle volume loss in critical care.
Key words: electrical muscle stimulation; critical care; intensive care unit acquired weakness; muscle volume; rehabilitation.
Accepted Aug 14, 2019; Epub ahead of print Aug 30, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Kensuke Nakamura, Department of Emergency and Critical Care Medicine, Hitachi General Hospital, 2-1-1, Jonan-cho, Hitachi, Ibaraki, 317-0077, Japan. E-mail: mamashockpapashock@yahoo.co.jp
Belt electrode skeletal muscle electrical stimulation can induce muscle contraction of the whole lower body. We examined its efficacy in intensive care. We randomly assigned intensive care unit patients to control and electrical muscle stimulation groups. Early rehabilitation was administered from day 2 and electrical muscle stimulation was administered by belt electrode skeletal muscle electrical stimulation. Femoral muscle volume was evaluated using computed tomography. Ninety-four severely ill patients were included and assigned to 47 control and 47 electrical muscle stimulation groups. Femoral muscle volumes were decreased significantly during day 1 to day 10 in both group, however, electrical muscle stimulation significantly inhibited muscle volume loss. There was a trend to improve the activity of daily living at discharge for electrical muscle stimulation. Belt electrode skeletal muscle electrical stimulation can be introduced from the acute phase of intensive care and inhibit muscle volume loss in critically ill patients.
Physical deterioration and muscle weakness among patients in the intensive care unit (ICU), caused by immobilization and by various illness and inflammation, are collectively termed intensive care unit acquired weakness (ICU-AW) (1, 2). Early rehabilitation can improve activities of daily living (ADL), exercise function, length of hospital stay, and mechanical ventilation (3–6). However, there are no publications regarding its effect on ICU-AW (7). It is often difficult to provide adequate physical therapy to critically ill patients due to disturbance of consciousness or the use of sedative agents (8). Although early rehabilitation in the ICU is regarded as a safe intervention (9–11), the safety of active physical therapy requires further research.
Electrical muscle stimulation (EMS) is used in physical therapy to induce muscle contraction via nerves using the application of electrical pulses below the pain threshold. EMS can be applied to patients with disturbance of consciousness (12, 13), therefore its use in critically ill patients is anticipated; and some reports have described its efficacy (14–16). A popular type of EMS is the pad type, which induces muscle contractions between pads. Belt-electrode skeletal muscle electrical stimulation (B-SES) is a belt-type EMS that induces contraction of wide and multiple muscles between belts, and which can be used to provide exercise to the entire lower body (17, 18). There are no study publications regarding the use of B-SES for critically ill patients, although it may be effective for use in physical therapy in the ICU.
The aim of the current study was to evaluate the efficacy of B-SES in reducing muscle volume loss in the early acute phase in ICU patients. A randomized control trial (RCT) was conducted. Functions such as ADL are most important for patients; however, maintenance of skeletal muscle volume is also important for critically ill patients. Loss of muscle volume is associated with muscle weakness, impaired physical function and mortality (19, 20). An earlier study by our group assessed femoral muscle volume using computed tomography (CT) scanning to evaluate ICU-AW with high inter-rater reliability and 3-dimensional evaluation (21). In the current study was used to evaluate exact and whole femoral muscle volume loss before and after intensive care with and without B-SES.
Patient selection
Patients admitted to the ICU at the emergency and critical care centre of Hitachi General Hospital from September 2017 to March 2018 were included in the study. This is a medical and surgical ICU for patients admitted from the emergency department and those with in-hospital acute deterioration. Exclusion criteria were: patients who had had a scheduled operation; mild cases or expected discharge from the ICU within 3 days; died by day 2; second admission to our ICU; younger than 20 years old; pregnant or believed pregnant; extracorporeal membrane oxygenation; multiple-drug-resistant bacteria detected; lower extremity event, such as infection, injury, or amputation; pacemaker implanted; neuromuscular diseases; CT not performed on the first day; designated as “do not attempt resuscitation”; unable to obtain informed consent; or cases included in other clinical trials.
This study is registered in University hospital Medical Information Network, UMIN000029349 on 29 Sep 2017. https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000033541.
This study was approved by the Ethics Review Board of Hitachi General Hospital (2017-52) and registered in University hospital Medical Information Network (UMIN) (number 000029349). Informed consent was obtained from all the participants.
Protocol
Informed consent was received from patients who had been admitted to the ICU. Included subjects were assigned a random number 0 or 1 using software (FileMaker pro 16; FileMaker, Inc., Santa Clara, CA, USA), designating them as members of the control group or EMS group, respectively. Treatments were started with non-blinded patients. In both groups early rehabilitation was introduced by the physical therapists from the second day of ICU admission (day 2). In the control group, physical therapists gave the patients the maximum possible muscle loading, including range of motion exercise, kicking stability ball, standing exercise and ambulation exercise, depending on the patient’s condition, for 20 min a day, on the bed or at the bedside. In the EMS group, belt-type EMS (G-TES®; Homer Ion Corp., Osaka, Japan) was applied by physical therapists from day 2. Belt electrodes were attached at 5 points: around the patient’s waist, above the knees and above the ankles on both sides. Electrical muscle stimulation and exercise were introduced throughout the abdomen and all lower extremities between the belts (Fig. 1). Thereafter, EMS (frequency 20 Hz, pulse width 250 μs) was administered once a day, for 20 min, with a duty cycle with stimulation for 5 s and a 2-s pause. The electrical intensity was adjusted by the physical therapist based on adequate muscle contraction according to patient response, expression or change in vital signs, including heart rate.
Fig. 1. Belt-electrode skeletal muscle electrical stimulation (B-SES). The belt electrodes were attached to 5 points: around the patient’s waist, above the knees, and above the ankles. Electrical muscle stimulation and exercise were introduced between the belts throughout the abdomen and both lower extremities.
In both groups, the other physical therapies, including range of motion exercise, mobilization and ambulation, were provided by nurses (at times other than the 20-min EMS) according to the patient’s condition, both in the ICU and in the general ward. Rehabilitation intensity was planned and adjusted by the physical therapists once daily, and the nurses provided rehabilitation following their instructions. The rehabilitation, including muscle loading or EMS, was administered daily, including during holidays. The EMS or control rehabilitation provided by physical therapists in the ICU was continued until day 10 using the same procedure, even if the patient was discharged from the ICU to the general ward, while the frequency and intensity of rehabilitation provided by nurses in the general ward was reduced under the direction of the physical therapists, taking into account the patient’s condition. Rehabilitation protocols for both groups are described in Table I. Sedation and analgesia were planned and adjusted by the medical doctors, and not changed due to the rehabilitation. Weaning and spontaneous breathing trials for mechanical ventilation were also performed by the medical doctors.
Table I. Rehabilitation protocol in control group and electrical muscle stimulation (EMS) group. Each rehabilitation protocol is described. Belt-electrode skeletal muscle electrical stimulation (B-SES) in the EMS group, or muscle loading with range of motion exercise, kicking stability ball, standing exercise and ambulation exercise in the control group were introduced in 20 min sessions by physical therapists. All other physical therapies were applied similarly by the nurses to each patient according to the patient´s condition
This clinical study was approved by the ethics board of our hospital (2017-52) and is registered at the University Hospital Medical Information Network (UMIN) (number 000029349).
Outcomes and measurements
Acute skeletal muscle wasting in femoral muscles has been reported to occur within 10 days in critical illness (22), therefore the primary outcome chosen for this study was change in femoral muscle volume (%) from the first day the patient was admitted to ICU (day 1) to day 10. In both groups, plain femoral CT was performed on day 1 and day 10. Day 10 CT was performed even if the patient was discharged from the ICU to the general ward. Cases discharged from the hospital by day 10 were excluded. CT scanning was performed with 64-line/128-slice CT (120-kV tube voltage, 150–600-mA tube current (auto-exposure control), 0.35-s scan time, 0.625 × 64 collimation, 1.078 table pitch, and 2.5-mm slice) (Scenaria; Hitachi Ltd, Tokyo, Japan). Scanning was performed between the femoral head and patella, avoiding the pelvic organs as far as possible. Analysis was carried out using a system volume analyser (VINCENT®, Fujifilm Corp., Tokyo, Japan). All femoral muscles were extracted with the CT value of 0–100 in figures, reconstructed using 2.5-mm slices. Femoral muscle volume (ml) was calculated using sagittal direction integration of the cross-sectional area of the femoral muscle (21). The estimated maximum exposure radiation dose was calculated as 10–18 mGy by Waza-ari, a web-based CT dose calculation, and was minimized further by avoiding the pelvic organs. These analyses were performed by a radiology technician who was blinded to the patient group.
Secondary outcomes were: length of ICU stay, 28-day survival rate, hospital stay and mechanical ventilation, and Barthel Index (23) at discharge from the hospital. The Barthel Index at discharge was evaluated by nurses who were blinded to the patient group.
Age, sex, Acute Physiology, and Chronic Health Evaluation (APACHE II) score, Sequential Organ Failure Assessment (SOFA) score and complicating diseases were analysed as basic characteristics. The use of adjunctive therapy, such as mechanical ventilation, renal replacement therapy, steroid therapy, sedatives, vasopressive agents, and muscle relaxants, were evaluated. The description of sedatives and analgesics, administered when the first rehabilitation was introduced on day 2, were also analysed. As nutrition therapy was generally moved from the acute phase to the post-acute phase on day 7 in our ICU clinical practice (24), total calories per day, total protein per day and enteral nutrition/total nutrition ratio on day 7 were analysed for information regarding nutrition given in both groups.
For intention-to-treat analysis, 28-day survival, lengths of ICU stay, hospital stay, and mechanical ventilation were analysed as outcomes.
Sample size estimation
A power analysis using G*Power 3 for Windows (Heinrich Heine University, Dusseldorf, Germany) was performed during the planning phase of this study. The effect size was estimated by referring to our previous work (21), which reported that mean femoral muscle volume loss for 2 weeks after intensive care was 20.3% (standard deviation (SD) 10.3%). The detection effect amount was set as SD × 1, level of significance 0.05, and power 0.8, then a necessary sample size of 17 was calculated for each group. Therefore, 20 patients, in whom day 1 and day 10 CT analysis could be performed, were targeted for each group.
Statistical analysis
Differences were assessed using Student’s t-tests, paired t-tests, χ2 tests, and one-way analysis of variance between the control group and EMS group, when normality of distribution of each parameter was not rejected by Shapiro–Wilk test. A Mann–Whitney test was performed for ordinal data and when the normal distribution was rejected. Survival analysis was conducted using log-rank tests. All statistical analyses were conducted using software (JMP 14; SAS Institute Inc. [https://waza-ari.nirs.qst.go.jp/en/index.html]). The results are expressed as means and standard deviations (SD). p-values < 0.05 were inferred as significant.
The patient flowchart is shown in Fig. 2. During the study period, 220 patients were admitted to the ICU. Of these, 126 were excluded, and 94 were included in the study. The patients were randomly assigned to control (n = 47) and EMS (n = 47) groups, respectively. A final total of 16 control group patients and 21 EMS group patients were included in femoral muscle analysis on day 10. Most of the drop-outs by day 10 were patients who recovered and were discharged early. The intensity and frequency of other rehabilitations were the same in both groups (Table I).
Fig. 2. Patient flowchart. A total of 220 patients were admitted to the intensive care unit (ICU) during the study period. Of these, 126 were excluded and 94 included in the study. Forty-seven patients per group were randomly assigned to a control group and electrical muscle stimulation (EMS) group, respectively. Sixteen patients in the control group and 21 in the EMS group were finally included in femoral muscle analysis on day 10. DNR: do not attempt resuscitation, CT: computed tomography, ECMO: extracorporeal membrane oxygenation.
The basic characteristics for which final muscle volume analysis was conducted are shown in Table II. Age, sex, severity score, adjunctive treatments, and complicating diseases were not significantly different between groups. Steroid use was almost 30% in both groups. Muscle relaxants were rarely used. Vasopressive agents and sedatives were administered to almost all patients in both groups. The use of sedatives and analgesics was not different between the groups (Table II). The given nutrition on day 7 was almost 22 kcal/kg/day, with protein 0.9 g/kg/day, in both groups, with 70% by enteral feeding. Both groups included many patients with sepsis as a complication.
Table II. Basic characteristics of each group for final femoral muscle analysis. Basic characteristics were not significantly different. Severe patients with mean sequential organ failure assessment (SOFA) score over 8 and Acute Physiology and Chronic Health Evaluation (APACHEII) score over 20 were included in the final analysis. Sedatives and analgesics administered when the first rehabilitation was introduced on day 2 were described with mean value (maximum and minimum)
Outcomes for the subjects in whom final muscle volume was analysed are shown in Table III and Fig. 3. Femoral muscle volume decreased significantly from day 1 to day 10 in both groups (p<0.0001). The mean rate of volume loss was 17.7% (SD 10.8%) (95% confidence interval; 95% CI 11.9–23.5) for controls and 10.4% (SD 10.1%) (95% CI 5.8–15.1) for EMS patients. The EMS group had significantly reduced the rate of muscle volume loss (41.2%) (p = 0.04). Mean Barthel Index at discharge was 29.0 (SD 18.8) (95% CI 12.0–46.0) for controls and 50.4 (SD 31.6) (95% CI 23.9–76.9) for EMS patients. Although total Barthel Index scores were higher in the EMS group, the difference was not statistically significant (p = 0.16). The Barthel Index score for stair-climbing (unable= 0, needs help= 5, independent up and down= 10) was better for EMS group 3.9 (SD 4.0) than in the control group 1.5 (1.5) (p = 0.04). There were no differences in other outcomes between groups.
Table III. Outcomes of respective groups for final femoral muscle analysis. Electrical muscle stimulation (EMS) contributed to significant inhibition rate of muscle volume loss (p = 0.0436). Barthel Index score at discharge was better in the EMS group, however, the difference was not significant (p = 0.163). The Barthel Index score for stair-climbing (unable = 0, needs help = 5, independent up and down = 10) was better for the EMS group than the control group (p = 0.04). Other outcomes were not different between groups. Differences were assessed by Mann–Whitney test
Fig. 3. Femoral muscle volume before and after intensive care in the control group and electrical muscle stimulation (EMS) group. Femoral muscle volumes: day 1 (black box) and day 10 (grey box). In both groups, muscle volume decreased significantly from day 1 to day 10 (p < 0.0001).
Basic characteristics of intention-to-treat analysis for each group are shown in Table SI1. The rate of mechanical ventilation was almost 80%. The 28-day survival curves (Fig. S11) were not significantly different (p = 0.79). The other outcomes: length of ICU stay, hospital stay, and mechanical ventilation, were also not significantly different (Table SII1). For all participants, there was no change greater than 20% from base rate for arterial pressure or heart rate, and no new arrhythmia event when the 20 min EMS or muscle loading was performed.
This RCT study examined the efficacy of EMS on loss of femoral muscle volume in critical care, and found that it significantly inhibited loss of muscle volume. The results suggest that EMS, applied via B-SES, could be introduced to critically ill patients fduring the acute phase of intensive care.
In this study EMS was introduced from day 2 of ICU admission. This is regarded as the earliest introduction of rehabilitation in the ICU. Early physical rehabilitation has been reported as related to harmful events at a rate of 5% or less (9, 11). It is regarded as safe, although a higher incidence of harmful events has also been reported (10). The results of one study suggest that overly active physical rehabilitation is not related to better outcomes (24). Therefore, caution is warranted in introducing active physical therapy during the acute phase. The results of the current study suggest that B-SES may be considered as an alternative physical therapy for use in early ICU rehabilitation.
Some RCTs have introduced EMS to critically ill patients during the early phase of intensive care. Although some reports show that EMS contributes to a reduction in rate of loss of muscle volume (25, 26) or maintainance of physical function (27–32), some studies found no change in that of muscle volume (30, 32, 33, 34) or that of physical function (25, 34) with EMS. We can speculate about the reasons for these different results, especially with regards to muscle volume. One explanation might be that the introduction and evaluation time-points differed in the respective trials. However, we consider that the most important reason was the method of evaluating muscle volume. In earlier studies, muscle volume outcome was evaluated using ultrasound, by measuring the circumference of femoral muscle or femoral muscle thickness. However, these evaluations are affected by oedema and fat in the muscle. Moreover, a 1- or 2-dimensional evaluation may have been unable to capture the region of the muscle on which the rehabilitation or EMS had an effect. If the same intervened muscle was evaluated, then it is possible that a portion other than the thickness evaluated had changed with the intervention. In this study, 3-dimensional evaluation of the bilateral whole femoral muscle by CT may have detected the change in the EMS-intervened muscle. An earlier study of EMS evaluated muscle volume using CT, but the study design, in which randomization was performed in the same patient by using one foot for EMS and the other as a control, might explain the negative result.
A further important factor is that the current study used B-SES, which can induce simultaneous contraction in all muscles from the abdomen to the toes. The efficacy of B-SES has been shown in healthy individuals and orthopaedic patients (17, 18); however, no studies have been published on the use of B-SES in an ICU or with critically ill patients. B-SES may be better suited for use in the rehabilitation of such severely ill patients. B-SES stimulation and 3-dimensional evaluation of the whole femoral muscle could be used based on the verified efficacy of EMS.
Although the current study did not find any significant difference between the groups in terms of total Barthel Index at discharge, higher Barthel Index scores were observed in the EMS group and the score for stair-climbing was significantly better. The rate of muscle volume loss may be associated with muscle weakness and impaired physical function (19, 20). In this study, EMS intervened in the whole lower body and maintained the muscle volume of the lower body. The reduced the rate of loss of muscle volume might be associated with areas of walking ability that require much more muscle function, such as the ability to climb stairs. Further research is needed to clarify the effect of EMS on physical function, using evaluation with many other functional tests.
Limitations
This study has a number of limitations. The study is an RCT, but some bias may be present as the treatment was not blinded to physicians, other medical staff or patients. The analysis was blinded only regarding the final evaluation of muscle volume and Barthel Index. This RCT was a single-centre study with a small sample size, and high rates of exclusion and drop-out. Caution is therefore warranted when interpreting the results with regard to general clinical practice. CT evaluation involves the problem of exposure to radiation. Although effort was made to minimize exposure, young patients could not be included in the study. Due to the ageing of Japanese society and national health insurance the study included many older adults (mean age over 70 years). The primary outcome was muscle volume. However, physical functions, such as muscle strength or endurance, and a long follow-up outcome, should be measured for ICU-AW. The given nutrition in this study was 22 kcal/kg/day, with protein 0.9 g/kg/day, on day 7 in both groups, which was lower than is recommended by critical care guidelines (35). While the nutrition target was higher, there were a number of reasons for this shortfall, especially for enteral nutrition. If more nutrition and protein had been delivered, the results may have been different to some degree.
Conclusion
B-SES can be introduced for critically ill patients during the acute phase of intensive care. It can significantly inhibit rate of loss of muscle volume.
The authors thank all the nursing specialists for their support for the study in their everyday work. Natsumi Koizumi, the research nurse in our department, deserves our special gratitude.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize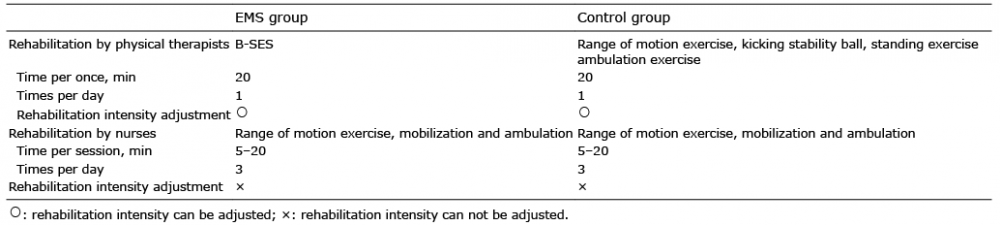 Click to show fullsize
Click to show fullsize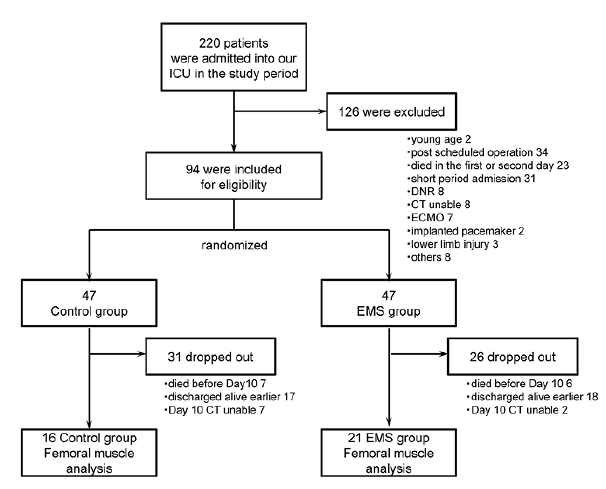 Click to show fullsize
Click to show fullsize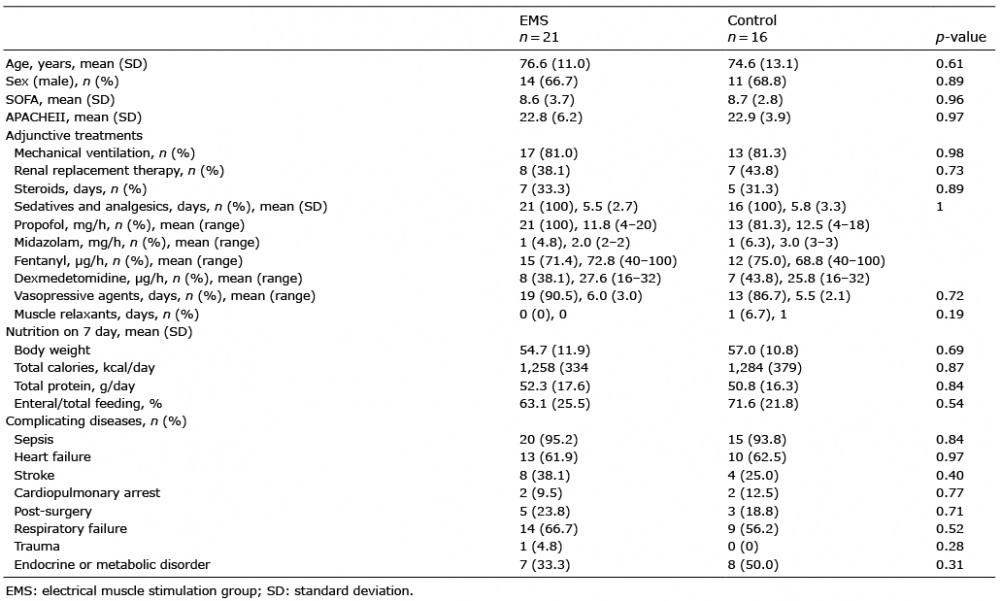 Click to show fullsize
Click to show fullsize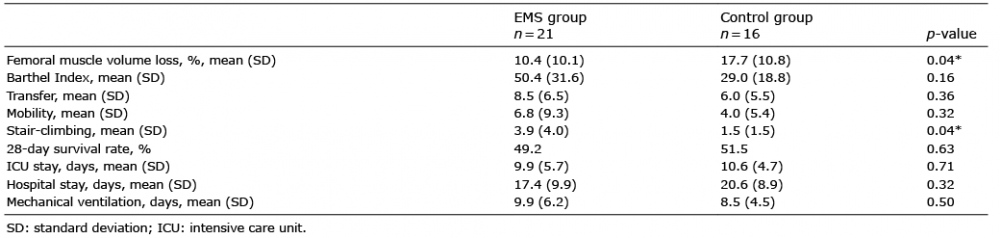 Click to show fullsize
Click to show fullsize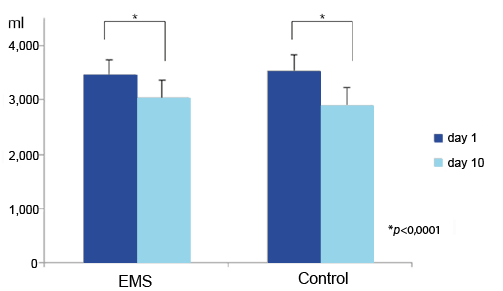 Click to show fullsize
Click to show fullsize