
From the 1Department of Orthopaedics and Traumatology, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong, 2Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul National University Bundang Hospital, South Korea and 3Department of Orthopaedic Surgery, Tohoku University School of Medicine, Japan
Objectives: To conduct a systematic review and meta-analysis to identify risk and associated factors for symptomatic rotator cuff tendinopathy.
Data sources: PubMed, CINAHL and Scopus were searched from inception to June 2017.
Study selection: Participants presented with signs and symptoms suggestive of rotator cuff tendinopathy/tendinosis/tendinitis, shoulder impingement syndrome, or subacromial bursitis diagnosed by clinical tests and/or conventional imaging.
Data extraction: Screening, quality assessment and data extraction were carried out by 2 reviewers.
Data synthesis: Sixteen studies were included in this review. Overall, 22 factors were identified and 5 factors were explored using meta-analysis. Pooled analyses provided strong evidence that age above 50 years (odds ratio (OR) = 3.31, 95% confidence interval (95% CI) = 2.30–4.76, I2 = 0%, p < 0.001) and diabetes (OR = 2.24, 95% CI = 1.37–3.65, I2 = 0%, p = 0.001) were associated with increased risk of rotator cuff tendinopathy. In addition, moderate evidence showed that work with the shoulder above 90° was associated with increased risk of rotator cuff tendinopathy (OR = 2.41, 95% CI = 1.31–4.45, I2= 83%, p = 0.005).
Conclusion: Age above 50 years, diabetes and overhead activities were associated with increased risk of rotator cuff tendinopathy.
Key words: rotator cuff tendinopathy; shoulder; overuse; risks; odd ratios; systematic review; meta-analysis.
Accepted Aug 21, 2019; Epub ahead of print Sep 5, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Hio Teng Leong, Department of Orthopaedics and Traumatology, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong. E-mail: annieleonght@cuhk.edu.hk
Rotator cuff tendinopathy is one of the common causes of shoulder pain. Successful treatment of rotator cuff tendinopathy remains challenging; thus, it is essential to identify risk and associated factors of rotator cuff tendinopathy in order to develop prevention interventions. The current review included 16 studies, and overall 22 factors were identified. Pooled analyses showed age above 50 years, diabetes and performing overhead activities were associated with increased risk of rotator cuff tendinopathy.
Shoulder disorders are common musculoskeletal problems in Western society, with a 1-year prevalence of 47% and lifetime prevalence of up to 70% being reported (1). One of the common causes of shoulder pain is rotator cuff tendinopathy, which is characterized by pain and weakness during external rotation and elevation (2). Rotator cuff tendinopathy is an umbrella term that includes different shoulder conditions affecting subacromial structures, such as rotator cuff tendinitis/tendinosis, subacromial bursitis and shoulder impinge-ment syndrome (2–4). Rotator cuff tendinopathy is refractory to treatments (5), results in impaired activities of daily living and has a significant socio-economic burden due to loss of work and treatment costs (6).
The management of rotator cuff tendinopathy is mainly conservative. Recent systematic reviews and meta-analysis showed low or limited evidence that passive therapies, such as therapeutic ultrasound (7), extracorporeal shockwave therapy (8), low-level laser therapy, transcutaneous electrical nerve stimulation, pulsed electromagnetic field therapy (9), and other injections, such as platelet-rich plasma (10) and corticosteroid injections (11), are effective for rotator cuff tendinopathy. These passive therapies work chiefly on symptom relief and may not alleviate the mechanical stress of tendon pathologies (12, 13). Exercise therapy has been shown to be effective in reducing pain and improving function in rotator cuff tendinopathy (3). However, approximately 40% of patients with rotator cuff tendinopathy fail to respond to conservative treat-ment (14–16), and more than half of patients report recurrent and persistent pain over the long term (17). Successful treatment of rotator cuff tendinopathy remains challenging; thus, it is essential to identify risk and associated factors of rotator cuff tendinopathy for the development of prevention interventions.
The cause of rotator cuff tendinopathy has been reported to be multifactorial. A combination of extrinsic mechanical compression (i.e. narrowing of the subacromial space) and tendon overuse/overload (i.e. repetitive overhead activities) have been shown to be the major mechanism of rotator cuff tendinopathy (18). Thus, the diagnosis of rotator cuff tendinopathy including rotator cuff tendinitis/tendinosis, subacromial bursitis and shoulder impingement syndrome, requires a battery of clinical tests and/or a combination of conventional imaging (3, 19, 20). A recent systematic review of risk factors related to rotator cuff tears has been reported by Sayampanathan & Andrew (21); however, their study included individuals with both symptomatic and asymptomatic rotator cuff tears diagnosed by conventional imaging or arthroscopic evaluation. Previous studies have reported poor correlation between symptoms related to rotator cuff pathologies and structural failure observed in imaging (22–25). Miniaci et al. (23) reported that 86% of asymptomatic professional baseball pitchers have rotator cuff pathology, identified by magnetic resonance imaging (MRI). In addition, Girish et al., (26) reported that 96% of men without shoulder symptoms have structural abnormalities identified by ultrasound, including subacromial bursal thickening, supraspinatus tendinosis, and supraspinatus tears. Thus, the presence of structural tissue failure in large numbers of people without symptoms challenges the validity of imaging to identify the source of symptoms (2). Noting that the hallmark characteristics of rotator cuff tendinopathy are pain and weakness during arm elevation (2), the potential risk factors of symptomatic rotator cuff tendinopathy may not be identified in the previous systematic review (21). The aim of this study was to conduct a systematic review to identify risk and associated factors under the umbrella term of symptomatic rotator cuff tendinopathy, including rotator cuff tendinosis/tendinitis, shoulder impingement syndrome, and subacromial bursitis.
Protocol
A systematic review was performed using a predetermined protocol in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (27). Our review has been registered with the PROSPERO database (registration number CRD42017069708) (28).
Search strategy and criteria
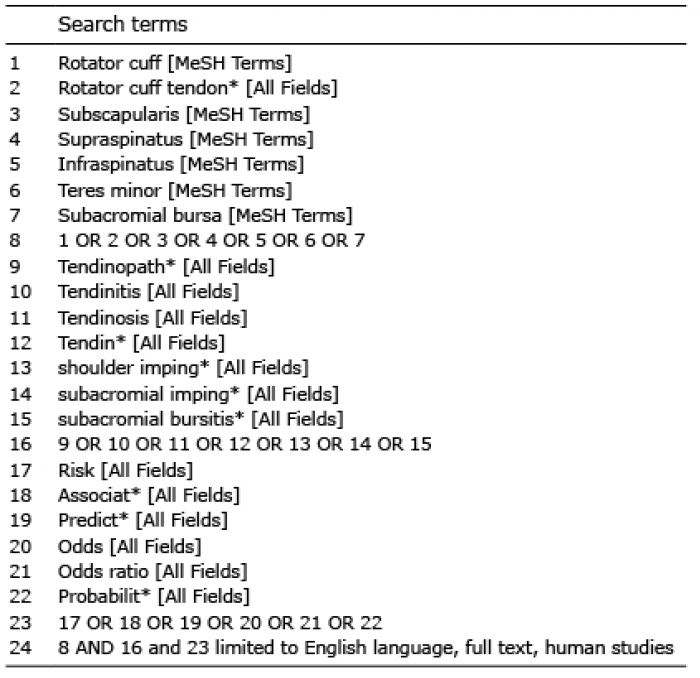
An electronic database search of PubMed, CINAHL, and Scopus was undertaken from inception to June 2017. The keywords used are shown in Table I. Supplementary searches were carried out by hand searching the reference lists of the included studies. The search results were imported into reference-manager software (Endnote X5; Thomson, New York, USA) to avoid duplication of records.
Table I. Keywords used in the PubMed database
A study was included if: (i) participants presented with signs and symptoms suggestive of rotator cuff tendinopathy/tendinosis/tendinitis, shoulder impingement syndrome, or subacromial bursitis diagnosed by clinical tests and/or conventional imaging (3, 19, 20); (ii) the study design was cross-sectional, case-control, prospective, and retrospective analyses; and (iii) the study report was published in English and full-text articles prior to June 2017. A study was excluded if: (i) participants were diagnosed with a rotator cuff full thickness tear or calcified tendinopathy, and other postsurgical conditions (3, 19, 20); (ii) the study population involved animal models or cadavers; and (iii) the study report was published as case studies, reviews (systematic and narrative), editorials, commentaries and opinion-based papers. Relevant studies were accessed for full-text review prior to inclusion in the systematic review.
Two reviewers (LHT, HX) independently screened all titles and/or abstracts and reviewed the studies identified for inclusion. Disagreements were resolved by consensus between the 2 reviewers or by a third reviewer (FSC) when required.
Assessment of methodological quality and risk of bias
Two reviewers (LHT and HX) independently assessed the methodological quality and risk of bias using a modified version of the Downs and Black (DB) checklist (29). We adapted the 15-item version of the original DB Checklist, which was previously used in a review of intrinsic and extrinsic risk factors associated with heel pain (30) and kinematic variables associated with anterior cruciate ligament reconstruction (31). The adapted version was deemed appropriate for this review as it does not apply questions relating to methodological design validity associated with an intervention. A total score ≥ 12 indicates high methodological quality, a score of 10 or 11 indicates moderate quality, and a score ≤ 9 indicates low quality (31). Disagreements in scores were resolved by consensus between the 2 reviewers or by a third reviewer (FSC) when required. Intra-class correlation coefficient (ICC) 2-way mixed-effects analysis was calculated using SPSS Version 24 for Windows (SPSS Inc., Chicago, IL, USA) to measure the interrater agreement between the 2 reviewers for quality assessment.
Data extraction and data synthesis
All data were extracted independently by 2 reviewers (LHT and HX). Disagreements were resolved by consensus between the 2 reviewers or a third reviewer (FSC) when required. Data extraction was based on a standardized form that includes: (i) the characteristics of the study (authors, years, design and country), (ii) the characteristics of participants (sample size, study population, sex and age), (iii) diagnostic criteria of rotator cuff tendinopathy (physical examination/imaging and inclusion criteria), (iv) prevalence/incidence, (v) investigated risk/associated factors, and (vi) reported significant results published in odds ratios (ORs) with their corresponding 95% CI.
Narrative synthesis was undertaken to categorize the identified risk/associated factors into 6 domains (demographics, systematic diseases, anthropometrics, mechanical factors, sports activities and psychological factors). When data from at least 3 studies could be combined, a meta-analysis was performed to obtain a pooled estimate of the ORs with their corresponding 95% CI. A random-effects model was used, and dichotomous data were weighted by the Mantel-Haenszel method. The I2 index was computed to represent the between-study heterogeneity, and the thresholds used were “low” (I2 = 25%–49%), “moderate” (I2 = 50%–74%), and “high” (I2 ≥ 75%) (32). A forest plot was made to show the ORs and 95% CI of each identified risk factor. The level of significance was set at 0.05 and Review Manager 5.3 (Cochrane Collaboration, Oxford, UK) was used for data analyses.
Level of evidence
Based on the methodological quality ratings, the identified risk factors were classified into 5 levels of evidence, based on the method used by van Tulder et al. (33) and Hart et al. (31): (1) Strong evidence: pooled results derived from 3 or more studies with a minimum of 2 high-quality studies that were statistically homogenous (I2 > 0.05); may be associated with a statistically significant or non-significant pooled result; (2) Moderate evidence: pooled results derived from multiple studies that were statistically heterogeneous, including at least one high-quality study; or from multiple moderate/low-quality studies, which were statistically homogenous; (3) Limited evidence: pooled results derived from 1 high-quality study or multiple moderate/low-quality studies, which were statistically heterogeneous; (4) Very limited evidence: pooled results derived from one moderate/low-quality study; and (5) no evidence: pooled results that are insignificant and derived from multiple statistically heterogeneous studies (regardless of quality).
Identification of studies
The electronic search identified 433 studies. After excluding 100 duplicates, 333 titles and abstracts were screened, and 303 irrelevant articles were excluded. The remaining 30 articles were obtained for full text, and another 16 articles were excluded based on the inclusion and exclusion criteria. Two additional articles were identified through hand searching of the reference lists of the included studies. A total of 16 articles were included in this systematic review (34–49), of which 10 were eligible for meta-analysis (Fig. 1) (34, 36–38, 41–44, 46, 49).
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram of the search strategy.
Methodological quality and risk of bias
The methodological quality scores of articles are reported in Table II. On the basis of the modified DB criteria, the median methodological quality of all 16 studies was 12/15 (range 8–15). There were 12 studies of high quality, 3 of moderate quality and one of low quality. The intraclass correlation coefficient for the inter-rater agreement between the 2 reviewers was 0.879 (95% CI 0.667–0.956).
Table II. Methodological quality assessment using the modified Downs and Black Checklista
Study characteristics
The 16 included studies were published between 1993 and 2017. The characteristics of the included studies are shown in Table III. Studies consisted of 1 prospective, 1 retrospective cohort, and 13 cross-sectional and 1 case-control studies representing 9 countries. The sample size ranged from 52 to 6237. The age of the participants ranged between 17 and 86 years. Of the included studies, 2 examined the general population (42, 43), 13 examined the working population (34, 36–41, 44–49) and one evaluated elite athletes (swimmers) (35). Clinical diagnostic tests (Hawkins-Kennedy/ Neer’s test/Empty can/painful arc/resisted abduction, internal rotation, external rotation or forward flexion of the shoulder) were performed in 14 studies to determine the diagnosis of rotator cuff tendinopathy, and 2 studies combined the use of clinical diagnostic test and imaging to confirm the diagnosis of rotator cuff tendinopathy (38, 42). Details of the diagnostic criteria of each study are summarized in Table III. The overall prevalence of rotator cuff tendinopathy ranged between 1.2% and 40% (general population = 1.2% (43), working population = 2.0–40% (34, 36, 37, 39–41, 44–49) and elite swimmers = 1.7% (35)).
Narrative synthesis
Factors that were associated with increased risk of rotator cuff tendinopathy are summarized in Table III. Overall, 22 potential risk factors were identified and were categorized into:
Demographics. Age above 50 years old (OR ranged between 1.03 and 4.10) (34, 36, 38, 41, 44, 49); Female sex (OR = 0.33, 95% CI = 0.14–0.78) (37); and Previous shoulder injury (χ2 = 24.9, p < 0.001) (35).
Systematic diseases. Diabetes (OR ranged between 2.90 and 4.70) (41–44); Hypertension/cardiovascular disease (OR = 4.49, 95% CI = 1.66–12.2) (34); and Osteoarthritis (OR = 2.39, 95% CI = 1.41–4.07) (42).
Anthropometrics. Shoulder instability (χ2 = 30.5, p < 0.001) (35); and Increased waist circumference (OR = 2.0, 95% CI 1.10–3.50) (43).
Mechanical factors. Work with the shoulder above 90° (OR ranged between 3.30 and 4.70) (36, 41, 42, 49); Repeated and sustained arm abduction (OR = 2.60, 95% CI 1.40–5.0) (36); Heavy manual work (OR = 3.81, 95% CI 1.93–7.51) (42); Repetitive work (OR ranged between 2.90 and 3.12) (39, 44); High frequency of work (OR ranged between 2.02 and 3.35) (39, 45, 46); High force exposure of work (OR ranged between 3.33 and 4.80) (39, 45); and Vibration work (OR ranged between 1.04 and 2.83) (45, 47, 48).
Sports activities. Swimming (OR = 1.98, 95% CI 1.11–3.53) (42); and Weight training (OR = 2.32, 95% CI 1.07–5.05) (42).
Psychological factors. High psychological demand (OR ranged between 1.30 and 3.19) (40, 44, 49); Low co-worker support and work with temporary workers (OR = 2.20, 95% CI 1.20–4.20) (36); Low job control/ decision authority (OR ranged between 0.79 and 6.68) (40, 44–46); Poor safety commitment (OR = 1.66, 95% CI 1.16–2.38) (40); and Job dissatisfaction (OR = 3.11, 95% CI 1.52–6.37) (34).
Meta-analysis
An OR with 95% CI was available for only 10 of the included studies due to limitations in the data presented (34, 36–38, 41–44, 46, 49). Thus, pooled meta-analysis was feasible for only 5 factors. These were age above 50 years (Fig. 2), female sex (Fig. 3), diabetes (Fig. 4), working with the shoulder above 90° (Fig. 5), and psychological demand (Fig. 6). Strong evidence showed that age above 50 years among the working population (OR 3.31 (95% CI 2.30–4.76, Z = 6.43, p < 0.001) and diabetes among the general and working population (OR 2.24, 95% CI 1.37–3.65, Z = 3.21, p = 0.001) were associated with increased risk of rotator cuff tendinopathy, and the between-study heterogeneity for both factors was low (between study I2 index=0%) so pooled analyses were deemed valid. Moderate evidence showed that working with the shoulder above 90° was revealed to be associated with increased risk of rotator cuff tendinopathy among the working population (OR 2.41, 95% CI 1.31–4.45, Z = 2.82, p = 0.005), but high levels of between-study heterogeneity (I2 index = 83%). Nevertheless, female sex (OR 1.31, 95% CI 0.83–2.05, Z = 1.15, p = 0.25) and psychological demand (OR 1.40, 95% CI = 0.95–2.08, Z = 1.69, p = 0.09) may not be associated with increased risk of rotator cuff tendinopathy among the working population, and the between-study heterogeneity was moderate (I2 index = 69% and 64%, respectively).
Fig. 2. Forest plot synthesizing the overall odds ratio for rotator cuff tendinopathy in individuals aged 50 years and above. 95% CI: 95% confidence interval; M-H = Mantel-Haenszel test.
Fig. 3. Forest plot synthesizing the overall odds ratio for rotator cuff tendinopathy in females. 95% CI: 95% confidence interval; M-H = Mantel-Haenszel test.
Fig. 4. Forest plot synthesizing the overall odds ratio for rotator cuff tendinopathy in individuals with diabetes. 95% CI: 95% confidence interval; M-H = Mantel-Haenszel test.
Fig. 5. Forest plot synthesizing the overall odds ratio for rotator cuff tendinopathy for work with the shoulder above 90°. 95% CI: 95% confidence interval; M-H = Mantel-Haenszel test.
Fig. 6. Forest plot synthesizing the overall odds ratio for rotator cuff tendinopathy for individuals with high psychological demand. 95% CI: 95% confidence interval; M-H = Mantel-Haenszel test.
This systematic review and meta-analysis examined factors that were associated with increased risk of rotator cuff tendinopathy. Overall, 22 potential risk factors were identified. Pooled analyses provided strong evidence of age over 50 years and diabetes being associated with increased risk of rotator cuff tendinopathy. In addition, moderate evidence showed that working with the shoulder above 90° was associated with increased risk of rotator cuff tendinopathy.
The aetiology of rotator cuff tendinopathy is multifactorial, and has been classified as intrinsic, extrinsic or a combination of both (50). Our finding showed that age above 50 years appears to be a significant factor in the intrinsic aetiology of rotator cuff tendinopathy among the working population, which is consistent with the knowledge regarding age-related degenerative changes in ageing rotator cuff tendons (36, 44, 51, 52). Biomechanical studies showed that there is decreased ultimate strain, decreased ultimate load, decreased elasticity, and decreased overall tensile strength in ageing tendons (53–57). In addition, microscopic and biochemical pathological changes showed degeneration of the tenocytes and collagen fibres, accumulation of lipids and ground substance (glycosaminoglycans) in ageing tendons (51). Nevertheless, there is no consensus as to whether pathological changes in the rotator cuff tendon are primarily due to ageing or a secondary consequence with mechanical overuse/overloading (50).
The findings of the current study showed that systematic disorders, such as diabetes, have been identified as risk and associated factors for rotator cuff tendinopathy among the general and working populations (41–44). Recent evidence showed that patients with diabetes had a 2.11-fold higher risk of rotator cuff disorders compared with those without diabetes (58). Previous studies have shown that hyperglycaemia associated with diabetes affects tendon collagen cross-linking (59) and reduces proteoglycan content (60). In addition, other studies also reported that people with diabetes demonstrated limited shoulder joint mobility, reduced shoulder muscle strength and impaired shoulder function compared with non-diabetes controls (61); and sonographic evaluation also revealed rotator cuff degeneration among patients with diabetes (62). Thus, strict control of diabetes with lifestyle/diet modification and careful monitoring of load progression during exercises may be indicated for the prevention and management of rotator cuff tendinopathy in diabetic patients (63). Nevertheless, other systematic disorders, such as cardiovascular disease (34) and osteoarthritis (42), were also reported to be associated with rotator cuff tendinopathy. However, the number of studies investigating these factors is small and the studies were largely heterogeneous; therefore, conducting a meta-analysis was impossible.
For the extrinsic mechanism, the mechanical theory has been proposed to be the main aetiology of rotator cuff tendinopathy. Micro-injuries in the tendon resulting from overload can lead to matrix and cell changes, altered mechanical properties of the tendon, and contribute to failed healing of the tendon (2, 19). Work with the shoulder above 90° was revealed to be associated with increased risk of rotator cuff tendinopathy among the working population (36, 41, 42, 49). Evidence from biomechanical studies supports these findings, and it is reported that the intramuscular pressure in the rotator cuff muscles increases with extreme arm elevation (64). In addition, overhead activities may mechanically compress or irritate the subacromial tissues and tendon structures between the humeral head and the acromion, resulting in rotator cuff tendinopathy (65). Moreover, other mechanical work-related factors, such as heavy manual work (42), repetitive work (39, 44), high frequency of work (39, 45, 46), high force exposure of work (39, 45) and vibration work (45, 47, 48), have been identified to be associated with increased risk of rotator cuff tendinopathy. Based on our findings, extrinsic factors that overload or mechanically compress or irritate the subacromial tissues and tendon structures between the humeral head and the acromion may contribute to rotator cuff tendinopathy.
Psychological factors, such as high psychological demand (40, 44, 49), low job control/decision authority (40, 44, 46), poor safety commitment (40), job dissatisfaction (34), and low co-worker support and work with temporary workers (41), have been reported to be risk and associated factors for rotator cuff tendinopathy among the working population (37). Pooled data analysis was conducted for high psychological demand (36, 44, 45, 49). However, our results showed a trend that high psychological demand might be associated with increased risk of rotator cuff tendinopathy and the between-study heterogeneity was high (I2 = 64%). The current findings may suggest that the awareness of psychological variables may be associated with rotator cuff tendinopathy. Clinicians should consider using validated screening tools for detection of the presence of psychological variables, and addressing individual psychological variables and the underlying cognitive behaviour should be considered as the management and prevention of rotator cuff tendinopathy (66).
The current systematic review and meta-analysis had several limitations due to the inherent biases of the included studies. Thus, caution should be taken when interpreting the findings. First, publication bias may be present, as only English language studies were included and only 3 databases were searched. Secondly, most of the included studies were either cross-sectional studies or cohort studies with diverse populations, although the majority of the included studies examined the working population (13/16). Pooled analysis showed age above 50 years and work with the shoulder above 90° were associated with increased risk of symptomatic rotator cuff tendinopathy among the working population, and diabetes was associated with increased risk of symptomatic rotator cuff tendinopathy among the general and working population. More prospective studies are required to identify the exact risk factors for rotator cuff tendinopathy in the general population and athletes of overhead sports. Thirdly, inconsistency in the method of tendinopathy diagnoses may explain the large between-study heterogeneity. In the present systematic review, we included only symptomatic patients with rotator cuff tendinopathy diagnosed by clinical tests or conventional imaging, which have been adopted in previous studies in order to identify those with rotator cuff tendinopathy (3, 19, 20). The majority of the included studies used clinical diagnostic tests to determine the diagnosis of rotator cuff tendinopathy. Future studies should combine the use of clinical diagnostic testing and imaging to confirm the diagnosis of rotator cuff tendinopathy. Finally, among the 22 potential risk factors that were identified, only 5 factors were explored with meta-analysis. This may be due to the small number of studies and the fact that the studies were largely heterogeneous; therefore, conducting a meta-analysis was impossible. Further high-quality prospective studies in regard to risk factors for rotator cuff tendinopathy are required.
In conclusion, this study demonstrates that there is evidence indicating that age above 50 years and diabetes are associated with increased risk of symptomatic rotator cuff tendinopathy. In addition, overhead shoulder activities above 90° were associated with increased risk of symptomatic rotator cuff tendinopathy. Further high-quality prospective studies are required to identify the exact risk factors for rotator cuff tendinopathy.


 Click to show fullsize
Click to show fullsize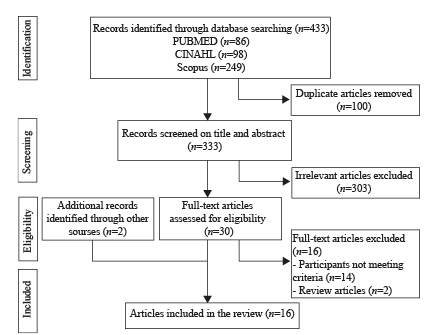 Click to show fullsize
Click to show fullsize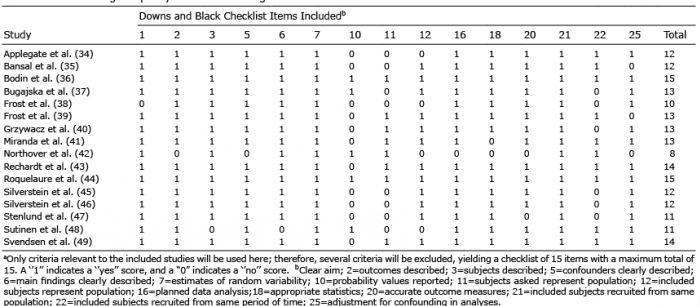 Click to show fullsize
Click to show fullsize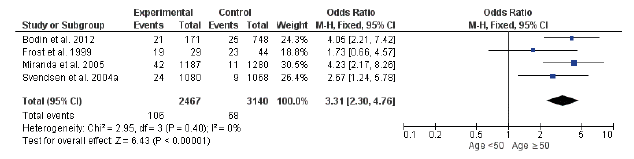 Click to show fullsize
Click to show fullsize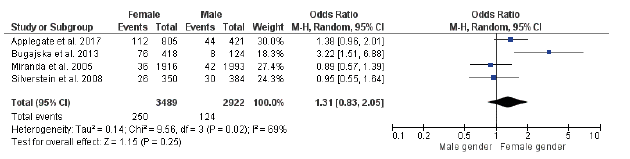 Click to show fullsize
Click to show fullsize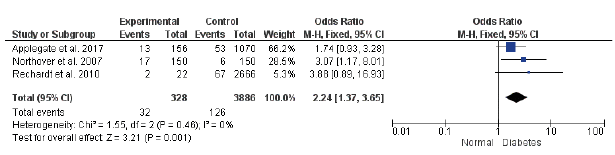 Click to show fullsize
Click to show fullsize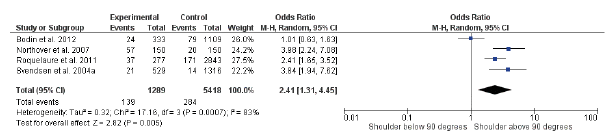 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize