
From the 1School of Rehabilitation Science, McMaster University, Hamilton, Ontario, 2Department of Physical Therapy, University of British Columbia, Vancouver, British Columbia and 3Department of Physical Therapy, University of Western, London, Ontario, Canada
Objective: To determine whether there are differences in exercise-associated changes in cognitive func-tion between males and females living with stroke.
Design: Secondary analysis of data from a prospective assessor-blinded randomized controlled trial.
Participants: Fifty participants (50–80 years, > 1 year post-stroke, able to walk ≥ 5 m).
Methods: Participants were allocated into a 6-month aerobic exercise programme (14 males, 11 females) or balance and flexibility programme (15 males, 10 females). Working memory (Verbal Digit Span Backwards Test), selective attention and conflict resolution (Stroop Colour-Word Test), and set shifting/cognitive flexibility (Trail-Making Test B) were assessed before and after the programmes.
Results: There was a group × time interaction in females (effect size 0.28, p = 0.03), which was not observed in males (effect size 0.01, p = 0.62). Females demonstrated a Stroop Colour-Word Interference test change of –2.3 s, whereas males demonstrated a change of +5.5 s following aerobic exercise. There were no differences between exercise groups in either sex for any of the other outcomes (working memory and set-shifting/cognitive flexibility).
Conclusion: Females living with stroke may demonstrate a greater response to exercise on selective attention and conflict resolution compared with males with stroke. These findings suggest that there may be sex-specific effects of exercise on cognitive func-tion in individuals with stroke.
Key words: sex; cognition; stroke; rehabilitation; exercise; randomized controlled trial.
Accepted Oct 2, 2019; Epub ahead of print Oct 14, 2019
J Rehabil Med 2020; 52: jrm00002
Correspondence address: Ada Tang, McMaster University, School of Rehabilitation Science, 1400 Main Street West, Institute of Applied Health Sciences 403, Hamilton Ontario L8S 1C7, Canada. E-mail: atang@mcmaster.ca
Exercise can improve thinking and memory in people with stroke, but we do not know if men and women improve to the same degree. This study examined whether there were differences in thinking and memory between men and women with stroke after 6 months of aerobic or balance/flexibility exercise. Volunteers were randomly assigned to a 6-month aerobic exercise programme or a balance/flexibility exercise programme. Thinking and memory skills were tested before and after the exercise programme. Women did better then men on a test of attention and problem-solving after exercise. There were no differences between men and women in any other test. These findings show that exercise may be better for improving attention and problem-solving in women living with stroke than in men.
Stroke is one of the leading causes of mortality and morbidity worldwide, and the sequelae from stroke have physical, psychosocial and cognitive consequences (1). While individuals may recover from physical disability resulting from stroke, cognitive impairments may limit the extent of independent living and community re-integration (2, 3). Approximately 70% of individuals with stroke experience cognitive impairments (4, 5), associated with functional decline (6, 7), reduced quality of life (6) and increased dependence in activities of daily living (8).
Exercise may benefit cognition in individuals living with stroke, such as executive function and memory (9, 10). Evidence in both single group studies and randomized controlled trials suggest that exercise may improve cognitive function after stroke. In single group studies, 12 weeks of aerobic and resistance training improved working memory, but not attention or executive function in a population of 9 individuals >12 months post-stroke (11). Six months of combined aerobic and resistance training led to improvements in global cognitive function in 41 patients ≥10 weeks post-stroke (12), and a 6-month exercise and recreation intervention improved cognitive flexibility, verbal memory and response inhibition, but not working memory or task-switching, in 11 participants ≥12 months post-stroke (13). In randomized controlled trials, the findings have been less consistent. Quaney and colleagues (14) found that an 8-week upper body cycling training programme was more effective at improving motor learning, processing speed, implicit memory, and motor function, but not executive func-tion, compared with a stretching control intervention in 38 participants ≥ 6 months post-stroke. Liu-Ambrose & Eng (15) demonstrated that a 6-month exercise and recreation programme resulted in improved selective attention and conflict resolution, and working memory in 28 individuals ≥ 12 months post- stroke. In contrast, Tang et al. (16) found no changes in working memory, set-shifting/cognitive flexibility, or selective attention and conflict resolution following 6 months of high- or low-intensity exercise in 47 individuals > 1 year post-stroke. Recently, a systematic review of 14 studies and 736 participants with stroke reported improvements in attention and processing speed, but not in executive function or working memory following physical activity training (17). These inconsistencies in the literature may be due to differences in cognitive domains assessed, outcome measures, exercise protocols used, or participant characteristics (17).
Sex refers to biological features related to physical and physiological aspects, such as hormone function, gene expression, chromosomes, and reproductive/sexual anatomy (18), whereas gender is a socially constructed attribute influencing how individuals behave, interact, and perceive themselves and others. Older females are known to be at higher risk of stroke than males (19), have higher rates of stroke-related mortality (19), present with more co-morbidities (20, 21), and experience more severe disability (20, 21). Sex may also be a potential moderator of the effects of exercise on cognitive function in older adults, given that female sex may positively influence the strength of the relationship between exercise and cognition (22, 23). An early systematic review published in 2003 (18 studies, 197 participants) reported that studies involving a high proportion of healthy older females demonstrated greater improvements in cognition following exercise training compared with studies involving a high proportion of healthy older males (22). In 33 older adults with mild cognitive impairment, executive function improved to a greater degree in females compared with males following 6 months of aerobic training (24). In addition, in 152 older adults with mild cognitive impairment, females demonstrated greater improvements in attention and memory following 12 months of moderate intensity walking (25). Recently, a systematic review of 41 studies involving 5,156 older adults reported that exercise was associated with greater improvements in executive functioning in studies involving a high proportion of females compared with a low proportion of females (26).
To date, there have been no studies examining sex differences in cognition following exercise interventions in individuals with stroke. Therefore, the objective of this study was to determine whether males and females living with stroke demonstrate different responses with respect to changes in working memory, set-shifting/cognitive flexibility and selective attention and conflict resolution following 6 months of aerobic or balance and flexibility exercise. Given that preliminary literature has displayed sex-specific improvements in cognition, favouring females, it was hypothesized that females with stroke would demonstrate greater improvements in executive functioning following aerobic exercise vs. balance and flexibility exercise compared with males.
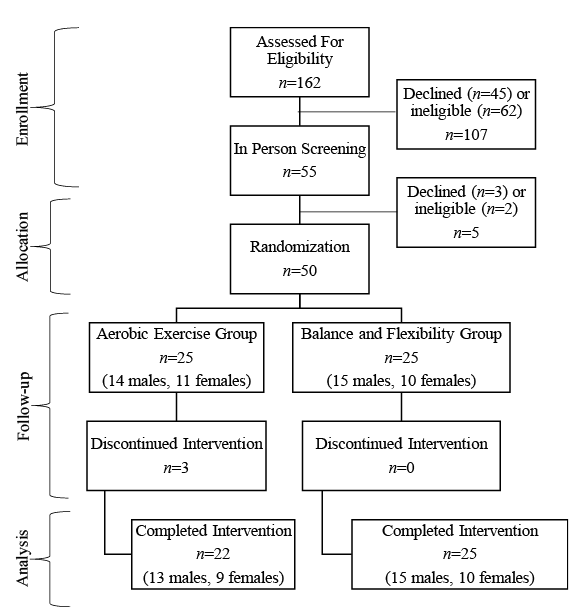
This study was a secondary analysis of data from a prospective assessor-blinded randomized controlled trial (27) that examined the effects of aerobic and balance and flexibility exercise on cardiovascular outcomes in 50 participants living in the community with stroke (Clinical Trial Registration; http://www.clinicaltrials.gov. Unique identifier: NCT01189045). Details of the main study are provided elsewhere (27), but, in brief, individuals were eligible if they were: between the ages of 50 and 80 years, > 1 year post-stroke, and able to walk ≥ 5 m. Exclusion criteria were: stroke from aneurysm, tumour, infection or significant health conditions that would preclude participation in exercise (presence of cardiovascular abnormalities, pacemaker, serious musculoskeletal or other conditions). Eligible participants were randomized into either a 6-month aerobic exercise (AE) programme or balance and flexibility (BF) programme using a 1:1 allocation sequence and permuted block sizes of 2 or 4. The flow of participants throughout the study is shown in Fig. 1.
Fig. 1. Consolidated Standards of Reporting Trials (CONSORT) diagram depicting participant flow through study.
The sample size calculated for the original analysis was determined as n = 24 per group. This was based on a 10% change in aerobic capacity, the primary outcome of the original study, utilizing an alpha level of 0.05, type II error of 90% and a standard deviation (SD) of 3 (27). While the original sample size was not established to examine subgroups of secondary outcomes, this was a preliminary analysis of sex differences in cognitive function following exercise after stroke.
Assessments
Upon study entry, participants were assessed for stroke severity and motor recovery using the National Institutes of Health Stroke Scale (28) and the Chedoke-McMaster Stroke Assessment (29), respectively. Aerobic capacity was assessed using a graded maximal exercise cycle ergometry test (27), and walking ability using 5-m self-selected gait speed and the 6-Minute Walk Test (30). The Montreal Cognitive Assessment (31, 32) and Center for Epidemiologic Studies– Depression Scale (33) were used to evaluate global cognitive function and presence of depressive symptoms, respectively.
Cognitive outcome measures
The Verbal Digit Span Backward Test (34), Trail-Making Test B (35, 36), and Stroop Test (37) were conducted to evaluate the effects of exercise on executive functioning at baseline and at 6 months (post-exercise). These outcome measures were selected based on the difficulties with executive functions (cognitive processes responsible for controlled, goal-directed behaviour) commonly observed after stroke (16).
The Verbal Digit Span Backwards Test (34) assesses working memory by verbally presenting random number sequences of increasing length to the participant, who then relayed the numbers back to the examiner in reverse order. One point was scored for each correct sequence relayed (maximum score 14); higher scores indicate better performance (34). The Verbal Digit Span Backwards Test has moderate concurrent validity with the Executive Function Performance Test in people with stroke (38).
The Trail-Making Test Part B (35, 36) was used to assess set shifting/cognitive flexibility, where the participant traced a line alternating between encircled numbers and letters (i.e. 1-A-2-B-3-C, etc.). The test was timed (in seconds, maximum 300 s), where shorter times indicate better cognitive flexibility (36). Selective attention and conflict resolution (problem-solving) were assessed using the Color-Word Stroop Test (37), where the participant identified the ink colour of words presented in incongruent coloured inks (e.g. the word “blue” printed in red ink). The time (in s) required to complete the test was recorded, where shorter times indicate better performance (37). The Trail-Making Test Part B and Color-Word Stroop test have good test-retest reliability in people with stroke and older adults, respectively (37, 39, 40).
Interventions
Both interventions took place 3×/week at 60 min/session with 3 instructors per 12–13 participants. In the aerobic exercise (AE) programme, exercise was performed at intensities that progressed from 40% to 80% of heart rate reserve. Each AE session involved a 10-min warm-up and cool-down and a 30–40-min aerobic component (walking, cycle ergometry, marching-on-the-spot, repeated sit-to-stand, and step ups onto platform steppers). In the BF programme, exercise was non-aerobic in nature and intensity was maintained below 40% heart rate reserve. Participants in the BF programme progressed through activities involving stretching, postural awareness, balance exercises and weight bearing. In order to minimize contamination between groups, the exercise classes were held at different times of the day and different spaces within a multi-purpose research facility.
Statistical analysis
Descriptive statistics were performed for all variables by sex (mean (SD) or median (IQR) for continuous variables and frequencies for categorical variables). In addition, χ2 or Fisher’s exact tests (if expected counts were less than 5) were performed for all categorical variables and independent t-tests or Mann–Whitney U tests were conducted for all continuous variables, by sex.
To evaluate the effects of exercise on cognition, disaggregated analysis (18) using a 2-way mixed analyses of covariance were conducted for each cognitive test, for each sex, with age (years) and baseline Montreal Cognitive Assessment scores (continuous variable) included as covariates. Older age is an important predictor of cognitive outcome and development of cognitive impairment post-stroke (41), and baseline cognitive status may be a factor influencing the extent of change. There is no non-parametric equivalent of the 2-way mixed analyses of covariance; thus, this method was used regardless if normality was met, due to the robust nature of the test. Data were analysed using Statistical Package for the Social Sciences (Version 23.0, Chicago, IL, USA). A significance level of p < 0.05 was used.
Baseline characteristics for the 50 participants enrolled in the study, separated by sex and group, are shown in Table I. While National Institute of Health Stroke Scale values indicate that participants had a mild severity of stroke, mean aerobic capacity and 6-Minute Walk Test scores were 53.7% (SD 138) (42) and 60% (SD 28.6) (43) of normative values, respectively. Males and females were similar in all characteristics at baseline with the exception of mean aerobic capacity (males 19.5 ml/kg/min (SD 6.4), females 12.7 ml/kg/min (SD 3.8), p < 0.001). There were no other differences between groups, within each sex at baseline. Baseline cognitive outcome scores, separated by sex and group, are shown in Table II.
Three (2 females and one male from the aerobic exercise group) of the 50 participants did not complete the study for reasons unrelated to the intervention and were deemed cases missing completely at random. Thus, analyses were performed from 47 participants who completed the main study. Pre- and post-training data on cognitive outcomes were not obtained for 5 participants due to significant aphasia (One female with missing data for Stroop Test and Trail-Making Test B, one male with missing data for Trail-Making Test B), difficulty understanding test instructions (2 males, one with missing data for Stroop Test and one with missing data for Trail-Making Test B) and colour blindness (1 male missing Stroop Test data). These individuals were excluded from the analysis. In addition, for individuals who were missing post-training cognitive data; baseline scores were carried forward.
Table I. Baseline characteristics for males and females, by intervention group
Table II. Baseline scores for cognitive measures for males and females, by intervention group
Data for results of cognitive outcomes are shown in Table III. After controlling for age and baseline Montreal Cognitive Assessment scores, a group × time interaction effect was observed in females for the Stroop test (F = 5.53, p = 0.03, effect size 0.28) that was not seen in males (F = 0.25, p = 0.62, effect size 0.01) (Table III). Specifically, females demonstrated a Stroop Colour-Word Interference test change of –2.3 s, whereas males demonstrated a change of +5.5, following AE. There were no differences between exercise groups in either sex for any of the other outcomes (working memory and set-shifting/cognitive flexibility) (Table III).
Table III. Changes in cognitive function in males and females, controlling for age and Montreal Cognitive Assessment score
Our previous analysis concluded that exercise was not effective in improving cognitive function, whereas this study extends this analysis to indicate that females demonstrated improvements in selective attention and conflict resolution following AE, whereas males did not. Other aspects of cognitive function (working memory and set-shifting/cognitive flexibility) did not demonstrate sex differences in treatment response. The positive benefits of exercise observed in females with stroke is consistent with previous studies that also reported selective improvements in the Stroop test performance among females (44, 45). Impairments in executive function are often the first cognitive domains affected by ageing (46), and are common after stroke (47, 48). Older females without known cognitive impairments perform better on tasks of executive function compared with males (49), suggesting that executive function may be selectively preserved in females and thus more responsive to improvement with exercise training, although further research to confirm this finding is warranted (26). Previous studies in the stroke population have also demonstrated exercise-associated improvements in the Stroop test (13, 15, 24, 50), but our results are the first to report that the beneficial effects may be influenced by sex.
The mechanisms underlying sex differences in the effects of exercise on executive function are not known. Hormonal and neurotrophic factors have been proposed as potential factors associated with cognitive function. Sex steroid hormones oestrogen (females) and testosterone (males) are associated with the preservation of cognitive function (23, 51–53), and emerging evidence in older adults suggests that this association may be more pronounced in females (54–56). For example, studies in older adults have demonstrated that, following menopause in females and andropause in males, remaining oestrogen levels (and to a smaller degree testosterone) were associated with improvements in semantic, episodic and working memory, as well as executive function in females only (54–56).
Brain-derived neurotropic factor (BDNF) is a neurotrophic factor that supports neuronal proliferation, growth, survival and synaptic plasticity and is involved in cellular mechanisms required for learning and memory (57). BDNF appears to be a mediator in the relationship between aerobic training and cognitive function, possibly due to its role in enhancing neurogenesis and reducing inflammation in the brain (58). Aerobic exercise results in the upregulation of BDNF in both individuals with (59) and without (60) neurological disorders, such as stroke, multiple sclerosis, Parkinson’s, and Alzheimer’s disease. While BDNF levels are known to decline with age, this decline is associated with cognitive impairment in older females only (61). Recently, it was reported that circulating levels of BDNF increased in older females following 6 months of aerobic training, whereas it decreased in males (62). Oestrogen has also been associated with greater BDNF expression in the hippocampus and cortex of females (63, 64). In animal models, mice exposed to an enriched environment involving running wheels stimulated greater upregulation of BDNF in several brain regions in female mice compared with male mice (65, 66). Similarly, in humans, greater duration, frequency and amount of total daily walking activity was associated with larger hippocampal volume in females, but not males (67). Taken together, these studies suggest that a unique, sex-specific link may exist between exercise and cognition, which may be mediated by BDNF (26).
In contrast to the improvements observed in selective attention and conflict resolution in females, we did not find improvements in other domains of executive function of working memory and set-shifting/cognitive flexibility in either males or females. This finding is aligned with previous research. For example, in a systematic review involving older adults, exercise was effective in improving visuospatial functioning and episodic memory but there were no sex-dependent effects observed (26). This suggests that males and females may perform similarly in certain cognitive domains. While there is still an absence of clear evidence to suggest that clinicians must consider the influence of sex within clinical decision making, it remains important to acknowledge that sex similarities and differences may exist. Further research is warranted.
A possible reason for these domain-specific effects may be that the duration was not sufficient or multi-modal exercise interventions are needed to elicit improvement in more cognitive domains. Specific exercise parameters to optimize improvement in cognitive function after stroke are currently unknown. The duration of exercise may play a role, as research in older adults has suggested that greater benefit is observed with exercise durations greater than 6 months (22). It is also possible that improvements in other cognitive domains may require more complex interventions, as opposed to aerobic training alone. A 12-week combined intervention involving aerobic and resistance exercise and cognitive training resulted in greater improvement in cognitive flexibility, working memory, and selective attention and conflict resolution compared with physical exercise alone in 179 post-stroke individuals (50). Thus, it appears that interventions that use a combined approach, along with those of longer durations, may be required for larger and more diffuse improvements in cognitive function to be observed (68).
Study limitations
The key limitation of this study is that it was not powered to detect changes in male and female subgroups in cognition post-exercise. However, it is likely that this limitation is minimal due to the small effect sizes; thus a fully powered study would potentially find clinically relevant differences. In addition, examining underlying mechanisms of cognitive improvement post-exercise was beyond the scope of this study. Furthermore, when measuring sex in the primary analysis, participants were provided with response options that did not differentiate sex and gender, or allow for non-binary responses, leaving potential for misclassification.
We acknowledge that gender, in addition to sex, may be another moderator in the relationship between exercise and cognitive function (18). Gender encompasses various sociocultural factors, such as education level, previous occupation, and engagement in exercise which can influence health behaviours, the environment and life course. Women access life-saving treatments less frequently than men, and fewer women participate in stroke rehabilitation, have higher institutional rates post-stroke, and have less social support during recovery in comparison to men (69). These sociocultural factors may influence baseline cognitive levels or the magnitude of change in cognitive function following exercise interventions. While we were not able to conduct gender-based analyses in the current study as information related to socio-cultural factors (level of education, hours of work, responsibility for caring for children etc.) were not collected and a gender index could not be created, future research should consider the role of gender in cognitive changes with exercise after stroke.
Conclusion
This study provides preliminary evidence to suggest that there may be sex differences with respect to exercise-associated changes in cognition specifically executive functioning after stroke. However, based on our findings, until more definitive results are reported, there is no clear rationale to support the consideration of sex in designing interventions post-stroke and it may be that males and females can be treated similarly. Given the prevalence of cognitive impairment post-stroke, further research is warranted to better understand this relationship and ultimately develop optimal sex-specific, evidence-based parameters for exercise training for people living with stroke.
This study was funded by the Vancouver Foundation/Carl and Elsie Halterman Research Fund and the Canadian Institutes of Health Research (CIHR) (MOP-111183). AT was supported by a personnel award from the Heart and Stroke Foundation, Ontario Provincial Office (CS I 7468), the Canadian Institutes of Health Research (MFE-98550) and the Michael Smith Foundation for Health Research (MSFHR) (ST-PDF-03003(11-1) CLIN), and JJE was supported by the CIHR (MSH-63617) and the MSFHR. TLA is a Canada Research Chair in Physical Activity, Mobility, and Cognitive Neuroscience.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize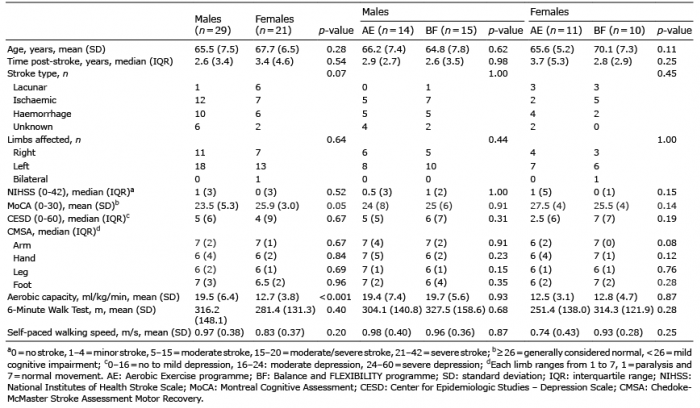 Click to show fullsize
Click to show fullsize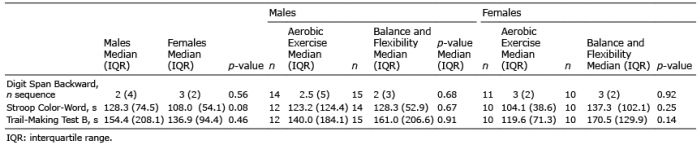 Click to show fullsize
Click to show fullsize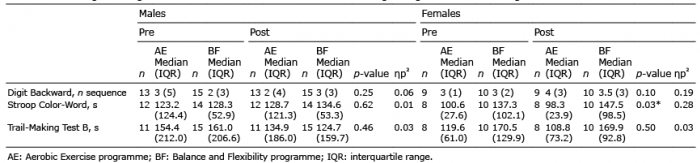 Click to show fullsize
Click to show fullsize