
From the Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia
Objective: To investigate whether a range of previously identified biopsychosocial risk factors were associated with poorer health-related quality of life after transport-related injuries.
Methods: This study involved 1,574 participants who sustained a transport-related injury, claimed compensation through the Victorian compensation scheme (in the Australian state of Victoria), and contributed to their cross-sectional outcome survey. Health-related quality of life was assessed using the EQ-5D-3L instrument.
Results: Of the 1,574 participants (mean age 44.8 (standard deviation 16.6) years, 61% reported poor recovery expectations, 55% reported high pain intensity, 54% reported poor satisfaction with care provided, and 41% reported no improvement in their recovery. Poor quality of life was defined as EQ-5D-3L summary score 0–0.70. Predictors of self-reported poor health-related quality of life included older age (65+ years) patients (adjusted odds ratios (aOR) = 1.73, 95% confidence interval (95% CI) 1.04–2.87), higher pain intensity (aOR = 2.17, 95% CI 1.27–3.71), self-reported pre-injury chronic pain (aOR = 1.47, 95% CI 1.00–2.17), self-reported pre-injury mental health issues (aOR = 2.62, 95% CI 1.80–3.82), no improvement in recovery in the last 3 months (aOR = 1.54, 95% CI 1.15–2.06), longer hospital stay (>7 days) (aOR = 2.34, 95% CI 1.43–4.21) and no support from the family (aOR = 2.37, 95% CI 1.62–3.46).
Conclusion: Biopsychosocial risk factors were associated with poorer health-related quality of life, regardless of the time since injury. Early assessment of these risk factors and tailored interventions will go some way towards improving outcomes among compensable patients with minor to moderate transport-related injuries.
Key words: recovery; health outcomes; road trauma; non-catastrophic injuries; compensation.
Transport-related injuries are a leading cause of dis-ability and mortality. The literature indicates that while some of these injuries are severe and catastrophic, most are classified as minor and moderate. In practice, it is expected that patients with minor and moderate injuries will recover with no serious consequences. How-ever, recent research shows that, while half of patients recover relatively quickly, the other half experience long-term physical and mental health disabilities. The current study found multiple biopsychosocial factors impacting patients’ outcomes. The use of the biopsychosocial conceptual framework, previous systematic review and qualitative study enabled assessment of specific biopsychosocial factors impacting recovery in patients claiming compensation for minor and moderate transport-related injuries. The identification of specific biopsychosocial factors identified as affecting recovery in this cohort will enable the development of a screening instrument to identify those of highest risk of poor recovery and to further develop strategies to facilitate enhanced outcomes.
Accepted Oct 8, 2019; Epub ahead of print Oct 16, 2019
J Rehabil Med 2020; 52: jrm00018
Correspondence address: Dr Stella Samoborec, Department of Epidemiology and Preventive Medicine, 553 St Kilda Rd, 3004, Melbourne, Vic. Australia. E-mail: stella.samoborec@monash.edu
Road trauma is a leading cause of disability and mortality worldwide, resulting in more disability-adjusted life-years than any other chronic disease (1, 2). It is estimated that, by 2020, transport-related injuries will be the third leading cause of disability-adjusted life years lost worldwide. In Australia, the annual cost of transport-related injuries is estimated at AU$27 billion (3). Specifically, most transport-related accidents result in minor and moderate injuries, with many patients claiming compensation for their injuries years after their accidents. This represents a significant cost to the compensation insurance schemes across Australia and the state of Victoria.
Victoria is a state in south-eastern Australia, which has a population of 5.4 million, representing 25% of the national census (4). The Transport Accident Commission (TAC) is a Victorian Government-owned organization set up to pay for treatment and benefits for people injured in transport accidents, promote road safety, and improve Victoria’s road trauma system.
Many studies have investigated recovery after road trauma, but most have focused on specific injury types, such as orthopaedic injuries (5), or on patients who sustain serious injury and are captured by trauma registries. Most patients with minor injuries are not hospitalized or represented in trauma registries. As such, factors contributing to physical and mental disabilities after patients sustain minor (e.g. whiplash, back and neck sprains and strains, lacerations, abrasions and contusions) and moderate (e.g. dislocation and fractures not requiring surgery) injuries are not well understood (6).
A large French cohort reported that almost half (45%) of patients with mild to moderate injuries never fully recover from their injuries (7), with 20% experiencing physical and mental disabilities 1 year after their injury. Similar findings have been reported in Australia in patients with compensable moderate to severe orthopaedic injuries (8).
There is some indication that patients who claim compensation have worse outcomes than those with no compensation claim (9–11), yet a recent systematic review demonstrated that the evidence remains inconclusive (12).
Recent data, collected by the TAC, have highlighted differences in outcomes between patients with similar minor and moderate injuries (internal source), yet the reasons for this variability remain unknown.
The aim of this study was to examine the association between a range of demographic and biopsychosocial factors and health-related quality of life following minor and moderate injuries sustained in transport accidents. Identifying factors that have the greatest impact on the post-injury health-related quality of life, and therefore on recovery, will inform the development of new screening tools and contextualized interventions to facilitate recovery.
Study setting
This study was conducted in the state of Victoria, Australia, where all people injured in land- or rail-based accidents are eligible to claim compensation for treatment, income replacement, rehabilitation and long-term support services via the TAC, regardless of fault (13).
Study design
Since 2009, the TAC has collected information from patients about their quality of life, health, vocational and claimant experience and wellbeing through an annual Client Outcomes Survey (COS) to assess health and recovery outcomes in those without catastrophic injury. The survey includes standardized measures of vocational and health status prior to injury, current vocational status, current physical and mental health status, persistent pain, mobility and functional independence, access to and satisfaction with healthcare, and satisfaction with the TAC service.
This study involved a cross-sectional analysis of de-identified COS data (financial year 2015/2016) linked with additional demographic and injury data extracted from the TAC’s administrative claims dataset.
The study was approved by Monash University Human Research Ethics Committee (MUHREC Project Number 2016 1044 760).
Study participants
A detailed description of participants involved in 2015/2016 COS has been described elsewhere (14).
The study sample consisted of patients who had a claim duration of at least 5 months. Participants were ineligible for inclusion in the study if their claims were for work-related injuries; claims involved TAC staff; claims involved claimants with behavioural “risks” (i.e. if during prior communications claimants demonstrated anger, violence, abusive language or drug abuse); claims with identified sensitivities relating to accident anniversaries (within 2 weeks of the survey period); and claims involving fatalities.
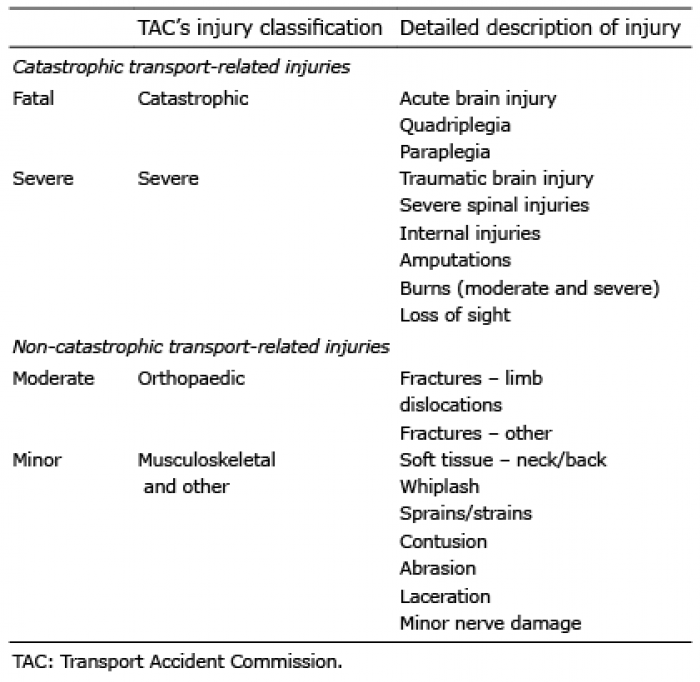
Participants aged over 18 years who sustained minor or moderate injuries in a road- or rail-based accident were eligible for inclusion in this study. The current TAC classification of minor and moderate injuries is outlined in Table I.
Table I. Classification of transport-related injuries
Variables
A recent systematic review (15) and qualitative study (16) provided the basis for selecting risk factors associated with poor recovery, to be tested in this study. The qualitative study sampled people contributing to the TAC COS, also used in this study. Demographic data, including injury characteristics, were extracted from the TAC’s administrative claims dataset, and included age, sex, education level, language, household structure, employment status at the time of the accident, return to work status and time since accident. Injury-related characteristics included admission to hospital, length of hospital stay, and injury severity. Injury severity was defined according to the TAC’s hierarchical classification of injuries; the hierarchy is evaluated by finding the most serious injury on the claim. At the TAC, injuries are coded in the claims system using the Systematized Nomenclature of Medicine (SNOMED) classification (TAC internal source).
Biopsychosocial factors collected as part of the Client Outcomes Survey
Biopsychosocial factors assessed in COS are shown in Table II and are classified according to the biopsychosocial domains (15). Biological factors included age, sex, pain status in the last 7 days, type of injury, pre-injury comorbidities, pre-injury chronic pain, and pre-injury depression and anxiety. Psychological factors included self-reported improvement in recovery in the last 3 months and recovery expectations. Social and health system factors included access to healthcare, satisfaction with healthcare, support from friends and family, hospitalization status and length of hospital stay.
Table II. Survey questions from the Client Outcomes Survey (COS) used to assess biopsychosocial factors impacting recovery
Health outcomes
Health-related quality of life was assessed using the EQ-5D-3L, a standardized measure, which assesses mobility, self-care, usual activities, pain/discomfort, and anxiety/depression (17). The standardized thresholds are divided into quartiles, with higher scores indicating better perceived health status. Summary index scores were calculated using age and sex population weights and the UK norms (18).
Statistical analyses
Baseline characteristics were presented using the descriptive statistics; means and standard deviations (SD), medians and interquartile ranges (IQR). Data between participants reporting “good”’ and “poor” health were compared using χ2 statistics for categorical and Mann–Whitney for continuous variables.
The EQ-5D-3L summary index score was calculated for each participant using age and sex population weights. The EQ-5D-3L summary score was dichotomized into “poor health” (i.e. poor and fair category 0–0.70 summary score) and “good health” (i.e. very good and good category 0.71–1.00 summary score) in accordance with the EQ-5D-3L user guide (19).
Logistic regression analysis was used to determine the association between predictor variables (i.e. biopsychosocial factors) and the dichotomized EQ-5D-3L summary score. Biopsychosocial factors were individually tested in univariate models. The odds ratio (OR) and corresponding 95% confidence intervals (95% CI) were reported. Those demonstrating a significant association (p-value < 0.05) with the outcome were added to a multivariate logistic regression model. The association between the biopsychosocial factors and the outcome was considered to be significant if the 95% CI crosses 1 (20). The multivariate model was adjusted for common confounders: age, sex, time since injury and injury severity (presented as adjusted odds ratios (aOR)). The analyses were performed using STATA Version 15.0 (StataCorp, College Station, TX, USA).
Study sample characteristics
Characteristics of the cohort are described in Table III. A total of 1,574 survey participants were included in the analyses, with a mean EQ-5D-3L health summary score of 0.71 (SD 0.25). More than half (56%) were male and 63% were in young (18–34) to middle-aged (35–54) age groups. More than one third of participants were in a relationship that involved children (37%) with secondary (44%) or tertiary undergraduate (41%) education level. Most participants stated that English was their native language (92%) and just over half were born in Australia (58%). At the time of the survey, only 12% reported full return-to-work (RTW).
Table III. Study participants demographic and injury characteristics
Significant differences were detected between those with good and poor outcome. Those who were more likely to report a poor health-related quality of life were older (29% vs 22%); female (51% vs 41%); had sustained a minor injury (60% vs 52%); lived in 1-parent family household (12% vs 6%); were born overseas (30% vs 24%); did not have English as their native language (12% vs 6%); and had a claim duration of >36 months (23% vs 14%).
In relation to the biopsychosocial factors impacting health-related quality of life, 61% of participants reported poor recovery expectations and no improvement in recovery over the last 3 months (41%); more than half reported experiencing pain (55%) and were not satisfied with the level of care provided by their health professionals (54%) (Fig. 1).
Fig. 1. Prevalence of the biopsychosocial barriers associated with poor health-related quality of life (n = 1,574).
Table IV shows the results of the logistic univariate and multivariable analysis.
Table IV. Association between predictor variables and poor outcomes
Biological factors that were significantly associated with poorer health-related quality of life included older (65+ years) age (aOR = 1.73, 95% CI 1.04–2.87); moderate to severe levels of pain (aOR = 2.17, 95% CI 1.27–3.71); pre-injury chronic pain (aOR = 1.47, 95% CI 1.00–2.17) and pre-injury mental health issues (aOR = 2.62, 95% CI 1.80–3.82).
Psychological factors that were significantly associated with poorer health-related quality of life included poor recovery expectations (aOR = 1.66, 95% CI 1.04–2.65) and perception of no improvement in condition over the last 3 months (aOR = 1.54, 95% CI 1.15–2.06).
Social factors that were significantly associated with poorer health-related quality of life included issues accessing medical services (aOR 2.27, 95% CI 0.86–1.53); no family support (aOR = 2.37, 95% CI 1.62–3.46); and length of hospital stay > 7 days (aOR = 2.34, 95% CI 1.43–4.21).
The aim of this study was to gain further insights into the profile and health outcomes of compensable patients in the Australian state of Victoria who have minor to moderate transport-related injuries. The study demonstrated that most biopsychosocial factors tested were associated with poorer health-related quality of life, after adjusting for common confounders. Furthermore, the study demonstrated that psychosocial factors (i.e. pre-injury mental health issues, poor perceptions of quality of care received, no access to care needed, no improvement in recovery, no support from friends and family and poor expectations of successful recovery) that were associated with worse outcomes may provide a greater ability to predict outcomes compared with traditional measures, such as injury severity, age and sex. All these factors, alongside initial injury and pre-injury affected health, appeared to have affected patients’ health-related quality of life.
A recent systematic review demonstrated that health-related quality of life among people injured in road accidents was significantly reduced for patients with minor to moderate injuries in comparison with the general population (21). The review revealed similar results to our findings; older females, with lower socioeconomic status and pre-injury mental health issues were most vulnerable group to loss of quality of life following road accidents.
Pre-injury mental health issues demonstrated the strongest association with poor outcomes. Whilst previous research suggested that affected mental health is one of the most disabling consequences of injury, it is not known how affected pre-injury mental health status influences outcomes. Some studies reported that minor physical injury could unmask mental health issues, which include presentations of psychosomatic reactions due to personality coping defences (11). In addition, mental issues can be further complicated and exacerbated when injuries result in a loss of skills and physical capabilities that significantly affect daily activities such as work, study and socializing. Nonetheless, even though we were not able to test the extent of how much pre-injury mental health issues changed or exacerbated patients’ outcomes, it appears to be an important factor to measure when assessing recovery outcomes (i.e. if recovery is defined as return to pre-injury health state). Affected mental health can be a trigger for other issues that could affect recovery, and therefore further research is required to understand the underlying mechanisms of the causal effect and relationship.
High levels of pain, a well-known risk factor for poor recovery (22), were reported by more than half the study participants, suggesting poor pain management. A recent qualitative study demonstrated that many GPs in Victoria refuse to treat patients going through compensation due to the complexity associated with managing their claims (23). The extent to which poor pain management in TAC claimants could be attributable to GP quality of care in this cohort is unknown, but requires further research.
More than half of patients involved in this study (54%) reported poor quality of care received from their health professionals. These findings correlate with a study of 120 road trauma survivors in the Australian state of Victoria, in 2011–2012, in which claimants reported a lack of coordination of post-discharge care, no consistent point of contact for ongoing management after discharge, prolonged waiting times and time constraints on appointments (24). The implication of such findings applies in particular to GPs, who patients perceive as “gate-keepers” for managing their recovery.
The importance of enhanced support for patients with musculoskeletal injuries is now well known. A recent qualitative study, investigating the role of social support in this cohort, suggested that these patients may benefit from support groups and maintenance of existing support networks (25). Another study reported that social support had a positive impact on physical health, persistent pain and return to work (26). The findings of the current study are consistent with previous studies reporting the significance of adequate and enhanced social support in patients with physical or mental disabilities.
Few studies allow the direct comparison of results, as other studies have focussed on particular injury types, such as whiplash-associated disorders, or particular factors, such as pain (8, 27–30). However, a recent longitudinal study from Queensland, Australia, involving compensable minor to moderate injury cohort, revealed that similar biopsychosocial factors were associated with poor recovery outcomes (31). The study also stressed the importance of early assessment of multiple biopsychosocial factors and the importance of looking beyond the injury to the “whole person”.
This study has a number of limitations. First, data were collected through a cross-sectional survey, which meant that it was not possible to analyse risk factors in the same cohort over time, or to determine the exact nature of the relationship between factors and outcomes. We attempted to control for time since injury in an effort to reduce this limitation. Selection bias is likely to be present, as all patients were compensation clients, yet sample was randomly selected in order to reduce selection bias. We do not know if our results would be applicable to a wider non-compensable injured population or to patients managed by other compensation agencies, hence caution is advised when generalizing these findings. Thirdly, this study is limited to the analysis of the association between variables available in the current survey, and many other factors identified through previous qualitative study were not tested (32). Finally, the EQ-5D-3L was the only validated instrument in this study. Patient-reported factors collected in the COS survey have not been validated previously.
In summary, these findings carry important policy, practice and research implications. The results will help the TAC to develop screening instruments to identify high-risk groups for non-recovery in the early stage of claims lodgement. The findings will also help in further development of a model that can identify patients’ needs so that targeted interventions can be implemented to facilitate enhanced outcomes. However, it is unlikely that improvement in outcomes will be achieved only with changes made in the compensation system; a greater understanding on how general practice can better engage with claimants and the TAC should be a priority. It is likely, and it has been previously emphasized (33, 34), that a multidisciplinary approach is needed in order to meet a patient’s complex needs. A multidisciplinary approach not only involves the GPs, but must also involve professional teams at multiple levels of the healthcare infrastructure, such as psychologists, neuropsychologists, social care workers, case rehabilitation managers, community nurses and rehabilitation specialists. The overall outcome of injured patients is probably determined by a successful integration of medical, psychosocial, financial and vocational resources. However, in order to assure that those in greatest need receive the appropriate multidisciplinary care approach, it is crucial to identify them as early as possible through targeted screening.
The authors would like to thank the funders and the Steering Committee members and gratefully acknowledge technical advice and support received from the TAC’s representatives. Finally, we express our gratitude to the individuals who participated in the study.”
SS has received Capital Markets Cooperative Research Centre scholarship funded by the Transport Accident Commission. The funders had no role in study design, data collection, data analysis or preparation of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize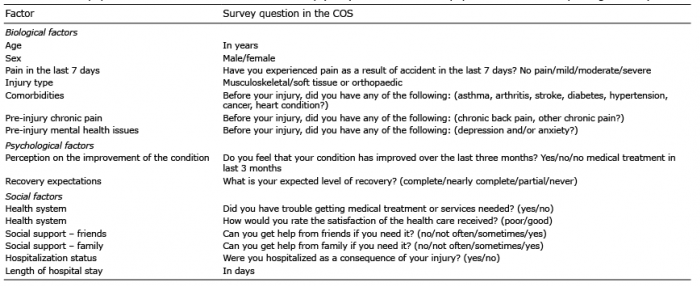 Click to show fullsize
Click to show fullsize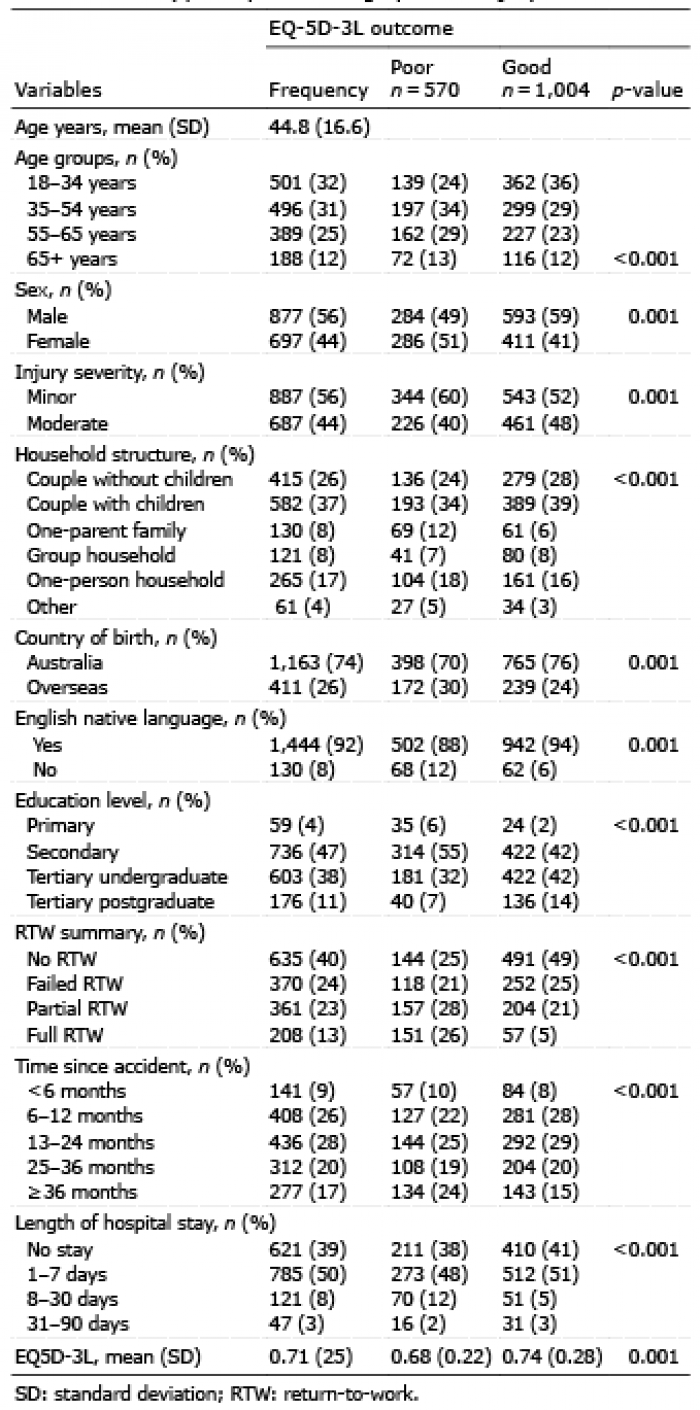 Click to show fullsize
Click to show fullsize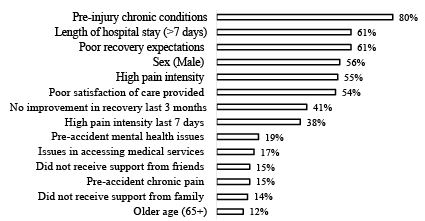 Click to show fullsize
Click to show fullsize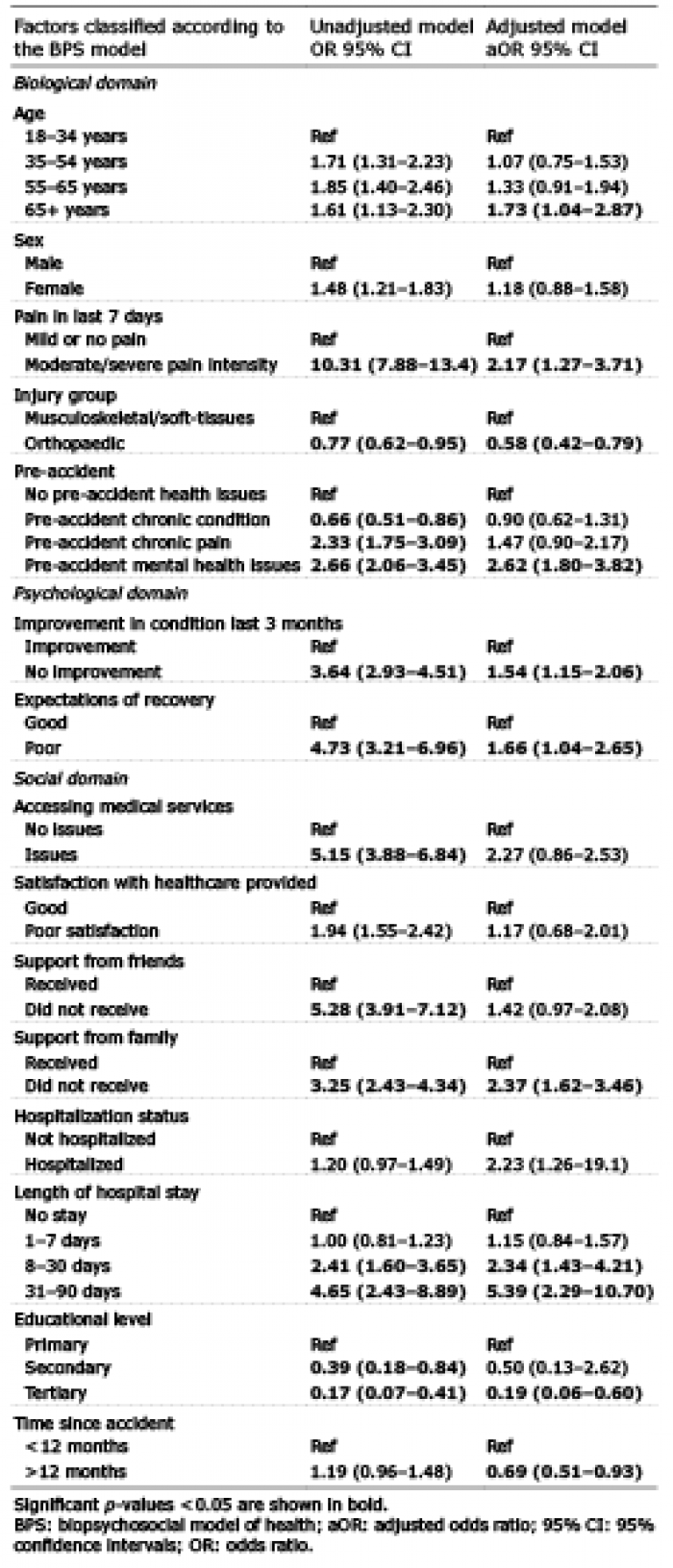 Click to show fullsize
Click to show fullsize