
From the 1School of Rehabilitation, Capital Medical University, 2Department of Orthopedics and Rehabilitation, Beijing Bo’ai Hospital, China Rehabilitation Research Center, Beijing and 3Department of Medical Research Center, International Science and Technology Cooperation Base of Geriatric Medicine, North China University of Science and Technology, Tangshan, China
*These authors contributed equally to this publication.
Objective: To identify differentially expressed serum proteins that could serve as sensitive biomarkers of heterotopic ossification in patients with traumatic brain injury.
Methods: From August 2014 to December 2015, 18 patients with traumatic brain injury were enrolled in the study, and blood samples were collected. Patients with traumatic brain injury were divided based on the presence (n = 9 patients, heterotopic ossification group) or absence (n = 9 patients, traumatic brain injury group or control group) of heterotopic ossification. Protein expression profiles were compared using 2-dimensional electrophoresis. Differentially expressed proteins were examined using matrix-assisted laser desorption/ionization and time-of-flight tandem mass spectrometry (MALDI-TOF/TOF). The differentially expressed proteins identified were further confirmed by Western blotting.
Results: Seven protein spots were differentially expressed between heterotopic ossification and traumatic brain injury groups in 2-dimensional electrophoresis analysis. Vitamin D binding protein (Gc protein), retinol binding protein 4 (RBP4) and haptoglobin expression decreased significantly in the heterotopic ossification group compared with the control group (p < 0.05), and this was further confirmed by Western blotting.
Conclusion: Lower levels of expression of Gc protein, RBP4 and haptoglobin may be closely related to heterotopic ossification after traumatic brain injury. These proteins may be potential biomarkers of heterotopic ossification secondary to traumatic brain injury.
Key words: traumatic brain injury; heterotopic ossification; proteomics, Gc protein, RBP4, haptoglobin.
Accepted Oct 24, 2019; Epub ahead of print Oct 29, 2019
J Rehabil Med 2020; 52: jrm00001
Correspondence address: Liu Kemin, Department of Orthopedics and Rehabilitation, Beijing Bo’ai Hospital, China Rehabilitation Research Center, Beijing, China. E-mail: keminlqliu@sina.com; and Li Zhiguo, International Science and Technology Cooperation Base of Geriatric Medicine, North China University of Science and Technology, Tangshan, China. E-mail: lizhigao@ncst.edu.cn
Heterotopic ossification secondary to traumatic brain injury results in limited range of motion in the affected joint. There is no optimal treatment for controlling heterotopic ossification. It is therefore of great importance to diagnose this condition. In order to identify potential biomarkers for heterotopic ossification, this study used proteomic techniques to compare the plasma profile of patients with traumatic brain injury with and without heterotopic ossification. Expression levels of 3 proteins were significantly lower in the heterotopic ossification group than in the control group. These proteins may be potential biomarkers of heterotopic ossification.
Traumatic brain injury (TBI) is common and its incidence is increasing. Clinical data have shown that 8–20% of TBI is complicated by heterotopic ossification (HO) (1). HO is defined as bone tissue that forms in the soft tissue around a joint. The exact pathophysiology of TBI-HO is not clear. However, several studies, such as those by Bidner et al. (2) and Kurer et al. (3), provide clear evidence for the hypothesis of a humoral mechanism for accelerated fracture healing with increased bone formation after TBI. Gautschi et al. (4) suggested an osteo-inductive effect of the cerebrospinal fluid from patients with severe TBI.
The onset of HO is accompanied by limited range of motion in the affected joint, and there is no optimal treatment for controlling the disease (5). The disability incurred as a result of HO is quite variable, and >20% of patients develop overt dysfunction as a result of soft-tissue loss, joint contractures, and chronic pain (6). Therefore, it is of great importance to diagnose this disease, and to find markers to determine whether HO is present after a TBI. At present, diagnosis of HO includes an analysis of a few biomarkers, such as serum alkaline phosphatase (7) and 24-h urinary prostaglandin levels (8). Creatine phosphokinase, prostaglandin E and matrix metalloproteinase 9 are potential biomarkers for neurogenic HO. However, the specificity and sensitivity of this analysis are poor (9–10). Proteomics has the potential to identify novel biomarkers from pathological tissues and biological fluids (11). Evidence exists that many disease processes are associated with specific quantitative and functional changes in proteins in pathological tissues (12). To find an easier and simpler diagnostic method and to identify pathogenic proteins associated with HO, we assessed plasma tissues from patients with TBI-HO for proteomic alterations.
The pathogenesis of HO in the context of a TBI is currently unclear. The basic assumption is that stimulating factors induce mesenchymal cells to differentiate into osteoblasts (1, 13). Chalmers et al. proposed 3 conditions necessary for the formation of HO: an osteogenic inducer, a precursor cell of bone formation, and an environment that permits osteogenesis. HO is thought to arise from an imbalance in the promotion and inhibition of osteogenesis induced by local and multiple systemic stimulating factors (14). Zhuang et al. (15) found that low expression of the alpha-2-HS-glycoprotein B chain was closely related to HO formation after a hip replacement. They concluded that AHSG B chain might serve as a sensitive protein biomarker of HO. Eun et al. (16) found that 6 proteins, including PRO2675, were highly expressed in patients with ossification of the posterior longitudinal ligament. They suggested that PRO2675 might serve as a sensitive protein biomarker for ossification of the posterior longitudinal ligament. Rodenberg et al. (10) suggested that matrix metalloproteinase-9 was a biomarker for early extracellular recombination, and that it might be useful for the early diagnosis of HO formation.
This study used proteomic technics to compare the plasma profile of patients with TBI with and without HO, with the aim of identifying potential biomarkers for HO.
Patients
From August 2014 to December 2015, a total of 18 patients with TBI were enrolled in the study. Of these 18 patients, 9 had HO (HO group) and 9 did not have HO (TBI group). Plasma samples were collected from each patient. Inclusion criteria for the TBI group were: age range 18–60 years; diagnosis of TBI according to clinical presentation and imaging findings (computed tomography (CT) and magnetic resonance imaging (MRI)); no serious hepatic, renal, hematopoietic, endocrine or psychiatric diseases; when coma was present, Glasgow Coma Score was between 3 and 12; and no HO was present before the TBI occurred. Inclusion criteria for the TBI group were, in the early stage (4–12 months after TBI), no signs of infection, disease progression and reduced range of motion in the affected joint; and X-rays of affected joints revealed HO.
Exclusion criteria were: any fractured limbs; any trauma (including burns) or previous surgery in the affected joints; accompanying spinal cord injury; or accompanying intracranial infection, myelitis, haemophilia, ankylosing spondylitis, senile idiopathic hyperostosis, diffuse idiopathic skeletal hyperostosis, ossification of the posterior longitudinal ligament, ossification of the ligamentum flavum or soft tissue ossification diseases.
Informed consent was obtained from all participants before collecting blood samples. The study was approved by the ethics committee of the China Rehabilitation Research Center (number 2015k056).
Plasma sample
Venous blood samples (5 ml) from each patient were placed in anticoagulant K2EDTA tubes. Within 2 h each sample was centrifuged at 4°C at 1,300 relative centrifugal force (RCF) for 10 min to remove blood cells. The supernatant was centrifuged at 2,400 RCF for 15 min to remove potentially remaining cellular material and platelets, in order to prepare platelet-poor plasma. The plasma was aliquoted and stored at –80°C until use.
Two-dimensional electrophoresis for protein separation
In order to reduce proteomic study heterogeneity and experimental cost, every 3 plasma samples were mixed randomly to form a new sample. Thus, a total of 3 mixed samples were prepared for each group (HO and TBI groups, 9 cases each). Each plasma sample was separated individually by 2-dimensional electro-phoresis and the differentially expressed proteins were identified by MALDI-TOF/TOF, as described previously (17). Briefly, 1.3 mg each of experimental group and control group plasma protein was loaded onto an immobilized pH gradient gel strip (pH3-10NL, 24 cm; GE Healthcare Life Sciences, Pittsburgh, PA, USA) using the in-gel rehydration mode. Protein was separated by first-dimensional electrophoresis (Ettan IPGphor 3 Isoelectric Focusing Unit, GE Healthcare Life Sciences), followed by 13%T and 3%C second-dimensional separation (Ettan DALT II System, GE Healthcare Life Sciences). Separated protein spots were visualized using colloidal Coomassie blue staining according to the manufacturer’s protocol. Images were analysed using Image Master 2D Platinum 6.0 software and protocol (GE Healthcare Life Sciences). To identify differentially expressed proteins, the differentially expressed protein spots were cut manually from the gels. Each excised protein spot was digested in-gel and identified by MALDI-TOF/TOF follow MASCOT analysis.
Western blot analysis
To avoid the uncertainties caused by sample mixture, all plasma samples were analysed by Western blot assay. Briefly, the protein sample (15 μg) was separated using a 12% polyacrylamide gel and electro-transferred to a nitrocellulose membrane in a Trans-Blot Semi-Dry Electrophoretic Transfer Cell (Bio-Rad, Hercules, CA, USA). Non-specific bands were blocked in TBS-T (25 mM Tris; 150 mM NaCl; 0.05% Tween20, pH 7.5) containing 5% skimmed milk at room temperature for 1 h. Membranes were subsequently incubated with the primary antibody anti-GC (1:1000 dilution; ABclonal), anti-HP (1:1000 dilution; Abcam), and anti-retinol binding-protein 4 (RBP4) (1:1000 dilution; ABclonal), and β-actin (1:5000 dilution; Sungene Biotech) overnight at 4°C, followed by incubation with anti-mouse or anti-rabbit horseradish peroxidise conjugated IgG at room temperature for 1 h. The immunocomplexes were visualized by chemiluminescence using the Amerisham ECL Western Blotting Detection kit (GE Healthcare Life Sciences). The signals were acquired by the molecular imager ChemiDocXRS+ (Bio-Rad) and then quantified using Quantity-One software, version 4.31 (Bio-Rad).
Statistical analysis
Statistical analysis was carried out using Student’s t-tests and false discovery rate (FDR), as described by Biron et al. (2). Data were expressed as the mean (standard deviation; SD), and all analyses were performed with SPSS 17. Groups were compared using a t-test for 2 independent samples. p-values < 0.05 were considered statistically significant.
The HO group comprised 2 males and 7 females, with a mean age of 52 years (SD 10.2). The mean disease course was 6.3 months (SD 0.5). The control group comprised 3 males and 6 females, with a mean age of 50 years (SD 9.2). Analysis of the baseline data of the 2 groups showed no significant differences in sex, age, course of the disease, or disease severity for HO (Table I).
Table I. Comparison of characteristics between patients with heterotopic ossification (HO group) and control group
Representative 2-dimensional gel electrophoresis (2-DE) patterns of plasma are shown in Fig. 1A. In the maps, most of the proteins are distributed in an area of pI 4.0–8.0 and molecular weight 14–97 kDa (Fig. 1A). Seven protein spots were found to be differentially expressed between the 2 groups (Fig. 1B). These spots were submitted for MALDI-TOF/TOF assay. Five proteins, with their MASCOT search results supporting identification data, are listed in Table II. The Mascot scores of the 5 proteins are > 60, which indicates that they are less likely to be wrongly identified (p < 0.05). In addition, compared with calculated pI and molecular weight, their pI variations is < 2 and molecular mass variation is less than 30%. These results imply that the possibility of incorrect identification of these proteins is very small.
Fig. 1. Differentially expressed plasma proteins between traumatic brain injury (TBI) and heterotopic ossification (HO) groups. (A) Comparison of plasma 2-DE patterns between TBI with and without HO. (B) Magnified comparison map of differentially expressed proteins.
Table II. Results of MALDI-TOF/TOF analysis of the differentially expressed proteins
The differential expression of GC, HP and RBP4 were further validated by Western blot analysis. As shown in Fig. 2, the expression levels of GC, HP and RBP4 were similar to those observed in the 2-DE gels. The abundance of protein was significantly altered (p < 0.05) in the plasma of patients with HO.
Fig. 2. Plasma abundances of specific proteins show differential expression between traumatic brain injury (TBI) and heterotopic ossification (HO) groups. Abundances were quantified for (top left) vitamin D binding protein (GC), (top right) retinol binding protein 4 (RBP4), and (bottom left) haptoglobin (HP). Top panels: Western blots show plasma samples probed with specific antibodies against the indicated proteins. Bottom panels: comparisons of mean±standard deviation (SD) volumes in patients with TBI-HO and with TBI alone. *p < 0.05.
Protein separation using 2-dimensional electrophoresis in this study showed that GC, HP, and RBP4 are differentially expressed in the plasma of patients with HO. These results were confirmed by Western blot analysis. The findings may contribute to improved understanding of the pathogenesis of TBI-HO. Moreover, they may represent new biomarkers for the diagnosis of HO secondary to TBI.
In 1959, a new plasma protein was first discovered by Hirschfeld, using immunological methods. This protein was named the “Gc protein” according to its immunological properties. It is also known as “vitamin D binding protein”, and its concentration in plasma is high. Gc protein is mostly secreted by liver cells and it possesses a number of biochemical functions. It facilitates binding between actin and vitamin D and it strengthens the chemotactic activity of C5 for neutrophils (18). A number of studies have shown that polymorphisms in the vitamin D receptor gene may be associated with ossification of the posterior longitudinal ligament (19, 20). Moreover, Gc protein-derived macrophage activating factor was shown to stimulate osteoclast activity and promote bone resorption (21, 22). Those activities suggest that the Gc protein might influence the formation of HO by affecting osteoclast activity.
In 2005, Yang et al. (23) reported the identification of a new adipose tissue factor, known as RBP4. RBP4 is a single peptide chain, mainly generated by fat cells in liver and placenta. The function of RBP4 is to transport small-molecular-weight hydrophobic proteins. It is also involved in vitamin A metabolism and storage. Interestingly, a phenomenon called “shifting” has been observed in many human diseases, where bone tissue is replaced with adipose tissue. For example, in ageing, long-term use of corticosteroids and long-term immobilization, reductions in bone formation are accompanied by increases in bone marrow adipose tissue. Both osteoblasts and adipose cells are derived from bone marrow mesenchymal stem cells. The shifting phenomenon suggests that the differentiation of bone marrow mesenchymal stem cells into adipogenic and osteogenic lineages are not isolated processes; instead, there appears to be a balance between these processes (24). Studies of adipocytes have shown that inhibiting RBP4 expression promoted adipogenic differentiation (25). Conversely, retinol could induce osteogenic differentiation and inhibit adipogenic differentiation in mesenchymal stem cells (26). These data suggest that RBP4 may play a role in osteogenic differentiation. On the other hand, RBP4 may be involved in the balance between bone resorption and bone formation by increasing bone resorption. The underlying mechanism may involve direct vitamin A stimulation of osteoclast formation (27). Because the vitamin A receptor and the 1,25 dihydroxy vitamin D3 receptor belong to the steroid and thyroid hormone receptor family, their functions interfere with each other. Vitamin A may have an indirect negative effect on skeletal tissue, by regulating calcium levels and bone mineralization in ways that interfere with the normal function of vitamin D (28). Moreover, the correlation between RBP4 and the osteoclast index may be related to increases in inflammatory factors. For example, a variety of factors can stimulate the secretion of cytokines, such as interleukin 6 (IL-6) and tumour necrosis factor alpha (TNF-α) (9), which enhance the differentiation, maturation and activity of osteoclasts and increase the levels of free fatty acids. These conditions can promote bone resorption (30) and increase bone turnover, which then lead to an imbalance in bone formation and bone resorption processes.
Haptoglobin (Hp) is a highly abundant plasma glycoprotein. Its main function is to combine with free haemoglobin (Hb) to form stable Hp–Hb complexes. Mediated by the scavenger receptor CD163, these complexes are rapidly degraded by mononuclear phagocytes to protect DNA and tissues from oxidative damage (31, 32). Hp also regulates angiogenesis and arterial remodelling (33). These activities may contribute to HO, because revascularization is important to HO formation (34). In addition, a bioinformatics analysis of Hp showed that Hp is important in the molecular regulation of inflammation (35, 36). This finding suggests that Hp may play an important role in the inflammatory process of fracture healing, which is similar to the process of HO formation. A series of studies by Stevens et al. (37) showed that IL-1 and TNF-α could indirectly promote the expression and activity of Hp by stimulating IL-6 synthesis. In turn, Hp could inhibit the activities of cyclooxygenase and lipoxygenase, and thus inhibit the synthesis of inflammatory factors, such as leukotrienes and prostacyclin (38). Recent studies have found that prostaglandin E2 could prevent osteoblast differentiation (39). Presumably, Hp might interfere with the formation of HO through this pathway. In addition, Hp prevented the destruction of hyaluronic acid (HA), mediated by oxygen-derived free radicals, by forming HA-Hp complexes (40). This activity may also be linked to HO formation, as it has been reported that free radical scavengers could prevent formation of HO (41).
Limitation
This study has some limitations. First, it was designed as a case-control study; therefore, the results can only show a positive correlation between TBI-HO and low expression levels of Gc, HP and RBP4; they cannot indicate whether a causal relationship exists. Prospective studies are needed to clarify the relationship between TBI-HO and these factors. Secondly, the small size of this study might have limited the detection of some differences between groups. In addition, we did not simultaneously monitor the body’s vitamin status or the levels of inflammatory factors associated with bone metabolism; thus, many confounding factors may have affected the results or contributed to the lack of convincing results in this study.
This study showed that 3 proteins were expressed at a low level in the HO group. Because of the limitations of a case-control study, it is not possible to infer that low expression of protein is the origin or result of HO. This issue requires further in-depth research through prospective cohort study. If these biomarkers can diagnose HO early, then corresponding preventive measures could be taken to reduce or delay the occurrence of HO, reduce complications and disabilities, and improve quality of life in patients with TBI.
Conclusion
This study is the first to discover biomarkers for TBI-HO through the use of comparative proteomics. These results may contribute to increased understanding of the pathogenesis of TBI-HO. Moreover, these findings suggest that Gc, HP and RBP4 may be potential biomarkers for HO.


 Click to show fullsize
Click to show fullsize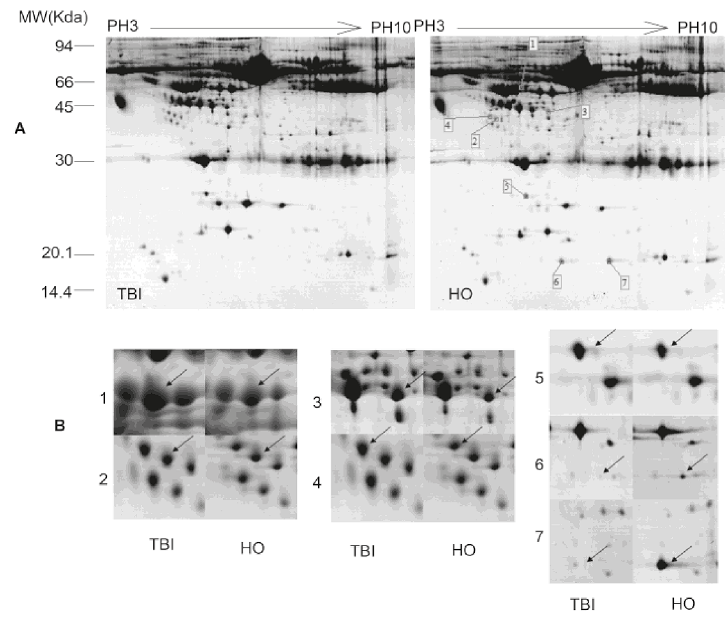 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize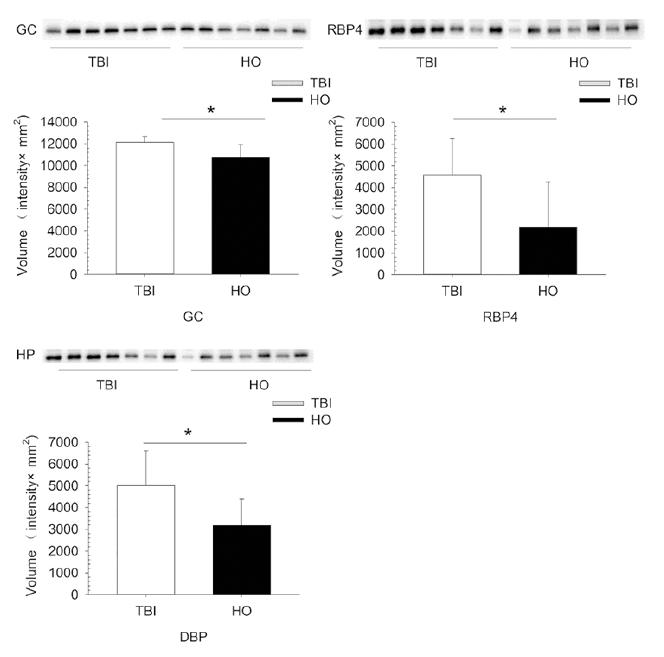 Click to show fullsize
Click to show fullsize