
From the 1Department of Rehabilitation Medicine, Royal Melbourne Hospital, Parkville, 2Department of Medicine (Royal Melbourne Hospital), University of Melbourne, Parkville, and 3Australian Rehabilitation Research Centre, Royal Melbourne Hospital, Parkville, Victoria, Australia
Objective: To evaluate the effectiveness and feasibility of an intensive technology-assisted inpatient enriched environmental programme for upper limb function.
Methods: Patients consecutively admitted to the rehabilitation unit randomly allocated to an intervention (enriched environmental programme, n = 46)) or a control group (usual ward activity, n = 46). Assessments were performed at baseline (T0), discharge (T1) and 3 months (T2) using validated measures.
Results: At T1, the enriched environmental group showed significant improvement in upper limb func-tion, compared with the control group: Action Research Arm Test (ARAT) “Total” (p = 0.002), and “Grip”, “Pinch” and “Gross” subscales (p < 0.05 for all), with small effect size = 0.04–0.16. Most participants in the enriched environmental group had clinically significant improvement > 5.7 points on the ARAT “Total” compared with the control group (83% vs 44%, p < 0.001). Participants in the enriched environmental group were more involved in various forms of activities during waking hours. At T2, despite no significant between-group difference in ARAT scores, the majority of participants in the enriched environmental group maintained the improvement (> 5.7 points) on ARAT “Total” compared with the control group (91% vs 61%, p = 0.001). Both groups improved in other measures at both T1 and T2.
Conclusion: An enriched environmental programme was feasible and effective in improving upper limb function and increasing the activity of patients during their inpatient subacute care.
Key words: enriched environment; rehabilitation; upper limb; function.
Accepted Oct 29, 2019; Epub ahead of print Nov 7, 2019
J Rehabil Med 2020; 52: jrm00003
Correspondence address: Bhasker Amatya, Department of Rehabilitation Medicine, Royal Melbourne Hospital, 34–54 Poplar Road, Parkville, Victoria 3052, Australia. E-mail: bhasker.amatya@mh.org.au
Upper limb deficits are common in people with neurological conditions. However, in practice, rehabilitation of the upper limb is frequently ignored and the amount of practice of upper limb tasks in rehabilitation settings is inadequate. Apart from their planned therapy sessions, patients in rehabilitation wards spend most of their waking hours inactive and relatively isolated. This study showed that taking part in an “environmental enrichment programme”, which provided the opportunity for patients to engage in additional activities of their choice during their waking hours in the wards, was beneficial to improve upper limb function.
Upper limb (UL) deficits frequently cause activity limitations in people with neurological conditions, such as stroke (1), multiple sclerosis (MS) (2) and traumatic brain injury (TBI) (3), which negatively impact on activities of daily living (ADL), leisure and vocational activities (4). These place significant clinical and economic burden on patients, family/caregivers and the healthcare system (5). It is estimated that 30–60% of stroke survivors have residual functional impairment of their paretic arm and hand after traditional rehabilitation (1).
Functional recovery of the paretic UL in neurological conditions continues to be one of the greatest challenges faced by rehabilitation professionals. Evidence suggests that appropriate rehabilitation involving use of the paralysed limbs induces reorganization of the undamaged cortical areas and leads to functional recovery (6). Published clinical trials have shown a better motor outcome, with various sensorimotor programmes, such as repetitive intensive mobilization, forced use of the paretic limb, or constraint-induced movement therapy, biofeedback, functional electrical stimulation and others (7, 8). One study demonstrated that a technology-assisted repetitive hand exercise programme (6 weeks) improved hand function, cognitive function and overall quality of life (QoL) in persons with stroke and other neurological disorders (9). Furthermore, clinical practice guidelines strongly recommend regular practice of tasks for UL rehabilitation (10, 11). However, in practice, rehabilitation of the UL is frequently ignored (12) and the amount of practice of UL tasks in rehabilitation settings is not adequate to drive the neural reorganization needed to promote functional improvement (13).
Environmental enrichment (EE) refers to an intervention designed to facilitate physical (motor and sensory), cognitive and social activity by provision of equipment and organization of a stimulating environment (14). The intervention is based on the concept that exposure to such environments encourages patients to be more active, without any therapist input (15). There is clear evidence that patients in rehabilitation wards, apart from their scheduled therapy sessions, spend most of their waking hours physically inactive and relatively isolated (16–20). Previous studies suggest that engagement in higher levels of therapeutically-based physical activity is associated with better physical function (21, 22) and greater independence (23), and a lack of such an environment may lead to post-acute cognitive and neural decline (24). Beneficial effects of EE and physical activities have been shown in a wide variety of animal models of brain disorders; these include cognitive enhancement, delayed disease onset, enhanced cellular plasticity and associated molecular processes (25). Our previous randomized controlled trial (RCT, n = 103 participants) demonstrated that an EE programme led to significant improvement in the functional and cognitive ability of inpatient neurological cohorts compared with routine ward activity programmes (26). Another prospective study (n = 29) evaluating an EE and activity programme in a stroke rehabilitation unit showed that patients in the EE programme were almost twice as likely (1.7 times) to be engaged in cognitive activities, 1.2 times more likely to engage in social activities, and 0.7 times as likely to be inactive and alone, compared with their counterparts in a non-enriched environment (15).
There is strong consensus amongst rehabilitation professionals about the need for an increase in the amount and intensity of practice of UL tasks following any neurological insult, especially during inpatient rehabilitation, as there are limited opportunities for patients to continue UL rehabilitation in the community. Questions have been raised as to whether the rehabilitation environment is conducive to their recovery, as therapy provided for UL impairment is often sub-optimal in frequency and intensity due to limited resources (9). To our knowledge, there is no published study to date that specifically explores a technology-assisted EE programme for UL dysfunction in patients in neurorehabilitation units. The primary aim of this study was to evaluate the effectiveness of an intensive technology-assisted inpatient EE programme on UL function compared with usual ward activities in a publicly funded neurorehabilitation unit. A secondary aim was to evaluate the feasibility of such a programme. We hypothesized that patients who participated in the EE programme would show significant improvement in UL function, self-efficacy/engagement, better self-management and participation (cognitive function, social interaction, QoL) compared with those performing usual/routine activities only.
Setting and study population
This study was a prospective RCT conducted between January 2017 and July 2018 at the 40-bed inpatient rehabilitation unit of the Royal Melbourne Hospital (RMH), a tertiary referral centre in Victoria, Australia. The study was approved by the Melbourne Health Human Research Ethics Committee (HREC number 2016.241). All patients with neurological conditions consecutively admitted to the rehabilitation ward underwent comprehensive clinical assessments (including cognitive and functional ability), specific care needs and goal setting by the treating medical, nursing and allied health staff. Those who met the following inclusion criteria were eligible to participate in the study: age over 18 years; assessed by a rehabilitation physician at admission for UL impairments; able to communicate and understand English; able and willing to participate in the intervention and provide informed consent. Patients were excluded if they were medically unstable, had significant musculo-tendinous or bony restrictions or severe spasticity, severe cognitive deficits (such as in post-traumatic amnesia) or unstable psychiatric issues (schizophrenia) and/or behaviour problems (agitation/aggression) and severe global communication problems (severe receptive dysphasia) that precluded participation in the programme.
Randomization
All eligible participants who agreed to participate and provided written consent were assıgned a study identification number and underwent a baseline structured interview (T0) conducted by an independent medical practitioner (not involved in the randomization) using standardized instruments (see Measures, below). An a priori computer-generated randomization sequence was used to allocate patients based on the serial numbers (1–100), either to the control (routine rehabilitation care and ward activities) or treatment groups (technology-assisted EE programme) by an independent project coordinator. Blinding the participants to group assignment was not possible. Participants were able to withdraw from the study at any time and were not re-enrolled later.
Intervention
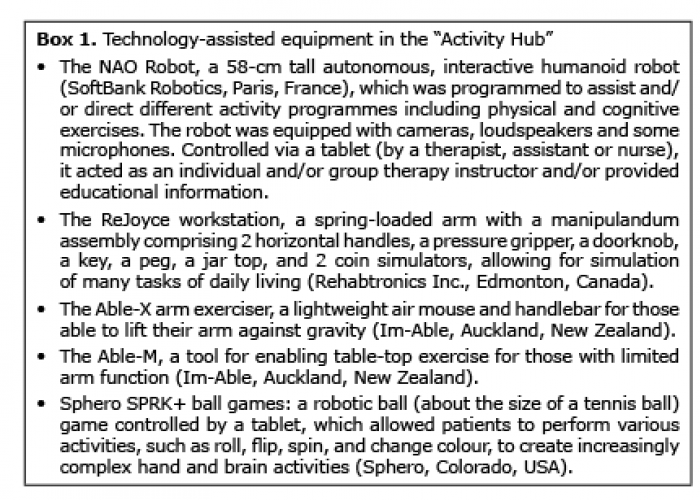
The EE intervention was provided in an area separate to the ward, called the “Activity Hub” (described below) (26). The “Activity Hub”, apart from providing different EE activities (such as library, music, board games, puzzles, painting, woodwork, gardening, etc.), has several workstations with technology-assisted equipment and activities, which are appropriate for patients with varying levels of severity of arm and hand impairment. Participants allocated to the intervention group were offered access to individual and/or group (with maximum of 5 participants per group) technology-assisted UL activities programmes, from Day 1 until discharge (based on patients’ need) (Box 1). The EE intervention comprised an additional 2-h activity session (physical and cognitive) provided daily (Monday to Friday), along with their daily therapy and ward activities, based on participant’s need and team consensus. Each session was supervised by an occupational therapist (OT) and an allied health assistant, who were independent of those providing routine rehabilitation therapies on the ward.
Based on individual requirements, treatment focused on UL function, including reaching in different directions, pronation/supination, and grasp and release. The programme included: a group exercise programme (20 min) directed by an interactive, programmed humanoid robot (NAO robot) and different UL specific exercise devices, i.e. Able-M and Able-X devices the ReJoyce and Sphere2 rolling balls (Box 1). The tasks and repetitions were recorded by the game software. Participants practiced the tasks independently, with some guidance from the therapist or assistant when necessary. Any other therapy received was recorded on a standardized case report form following consultation with the therapists involved. A priori compliance with the intervention programme was set at attendance for >80% of treatment sessions.
Box. 1
Control group
Participants assigned to the control group received usual ward-based activities (such as television, radio, reading materials, internet, Skype, games and wood workshop etc.). They were allowed to be freely involved in any activities consistent with current rehabilitation practice, but did not have access to the EE programme.
Assessments
All assessments, using a face-to-face structured interview technique, were completed by independent assessors (2 physicians, 1 research officer) who were not part of the “Activity Hub” teams, and were blinded to the participants’ treatment group. The assessments were administered at admission (T0), discharge from the ward (T1) and 3-month post-discharge (T2) using standardized instruments (see Measures, below). These assessments took approximately 30 min. The assessors did not prompt patients, but provided assistance for those who have difficulty completing the questionnaires. The assessors were trained in cognitive and functional ability assessments and received a further 2-day training session to ensure consistency in assessment and data collection. They did not share information about participants or assessments and received separate and different clinical record forms at each interview.
Current practice in the rehabilitation ward also included “nurse rounding”, where the allocated nurse checked hourly on their patients outside therapy time, to ensure they were not in pain, had access to equipment, etc., and documented patient’s activity at the time (physical, cognitive activities or inactive). In addition, all treating therapists provided patients with a daily schedule in 30-min blocks for their physical, occupational or speech therapy programme on a weekly basis. There were designated protected mealtimes for all patients on the service. This information was further systematically collated throughout the working week by an independent research assistant, using an existing log, nurse care plans and therapy journals.
The study comprised the following phases:
Initial assessment (at admission) (T0). All patient assessments were conducted within 24 h of admission to the service. This included routinely collected information for an individualized rehabilitation programme based on clinical need, such as: demographics (age, sex, marital status, education level, employment), disease-related information (diagnosis, rehabilitation subgroup, symptoms), medications and co-morbidities. Any patient concerns or comments were also captured in an open-ended questionnaire.
Assessment at discharge from neurorehabilitation unit (T1). The same tools used at T0 were utilized. Activity logs for both groups were collated, along with participants’ satisfaction with hospital stay. Adverse events during rehabilitation (such as falls, injury during treatment, etc.) were also noted.
Assessment at 3 months following discharge (T2). Independent research officers followed all participants who completed both T0 and T1 interviews in the outpatient clinic. The information obtained was similar to the T1 assessment.
All assessments were secured and filed and opened only at the time of data entry into a separate database by an independent data entry officer. Data were anonymized by use of a study identification code.
Outcome measures
Valid and reliable outcome measures were used, which represented different constructs in the International Classification of Functioning, Disability and Health (ICF) for “impairment”, “activity” and “participation” (27).
Measure for impairment.
The Neurological Impairment Scale (NIS) (version 8) (28) was used to assess the neurological impairments. The NIS comprises 17 items (each rated 0–2 or 0–3, giving a total score range of 0–50). It records severity of functional impairment across 13 domains mapped onto the ICF.
Measures for activity.
The Action Research Arm Test (ARAT) was used to assess active functional arm movement. It consists of 19 items in 4 subsections: grasp, grip, pinch, and gross movement (large-scale movements of the whole arm) with a maximum total score of 57.
The Functional Independence Measure (FIM) (29) was used to assess functional ability in 18 categories: Motor (13 items) assessing level of function in 4 subscales: Self-care, Transfers, Locomotion and Sphincter control; and Cognition (5 items). Participants were rated on each item on a scale of 1 to 7 (1 = total assistance, 4 = requires physical assistance, 5 = needs supervision, 6 = modified independence, 7 = independent) by trained staff.
The Multidimensional Health Locus of Control (MHLC) (30) was used to measure the locus of control, which refers to personal mastery beliefs and reflects an individual’s belief about the extent to which they are able to control or influence outcomes. This scale contained 18 items scored using a 6-point Likert response format, ranging from strongly disagree (1) to strongly agree (6).
The Rosenberg Self-Esteem Scale (RSES) (31) measured a positive or negative orientation toward oneself, an overall evaluation of one’s worth or value. This 10-item scale was scored on a 4-point Likert scale, ranging from strongly agree to strongly disagree.
Measures for participation.
The Montreal Cognitive Assessment (MoCA) (32) assessed cognitive impairment. The MoCA is a 30-point test (16 items and 11 categories) assessing multiple cognitive domains: short-term memory recall task, visuospatial abilities, executive function, attention, concentration memory, language and orientation to time and place. A score ≥ 26 indicates normal cognition.
The Euro-Quality of life (EQ-5D) (33) assessed the overall QoL in 5 health dimensions: mobility, self-care, daily activity, pain/discomfort, and anxiety/depression, and a sixth item assessed on a visual analogue scale (VAS). Responses to each of these 5 dimensions were divided into 3 ordinal levels (coded: no problems = 1; some/moderate problems = 2; severe or extreme problems = 3). Participants also rated their current overall health on a VAS from 0 (the worst health state they can imagine) to 100 (the best health state they can imagine).
Statistical methods
The primary outcome for this study was defined as the impact of the technology-assisted EE activities programme on ımprovement in patient UL functional outcomes, measured by the ARAT scale. An overall sample of 52 partıcıpants (26 partıcıpants ın each arm, assuming a 5% drop-out rate) was required to provıde 80% power to detect a minimal clinically important difference (MCID) of 5.7 points in ARAT score from baseline to post-intervention between intervention and control groups (2-sided α = 0.05) (34).
The Shapiro-Wilk test was used to check whether patients’ clinical and instrumental data were normally distributed. Baseline demographics and disease characteristics were compared between groups using independent t-tests, χ2 test and Mann–Whitney tests. The Shapiro-Wilk test was used to check whether clinical and instrumental data could be analysed with parametric statistical methods. A series of independent group t-tests or Wılcoxon rank tests for numeric data and χ2 test or Fısher’s exact test for categorıcal data (based on the collected data qualıty) compared change in the outcome measures scores over time [baseline (T0) – post-intervention (T1) and baseline (T0) – 3-month follow-up (T2)] for the control and intervention groups for all global and health status outcome scales. Clinically important changes were estimated as effect sizes against Cohen’s criteria for partial eta squared (η2) (0.01 = small, 0.06 = medium, 0.14 = large effect) (35). A p-value <0.05 was considered statistically significant. All analyses were completed with no adjustment for multiple comparisons using the IBM SPSS Statistics Package Version 21 (Chicago, IL, USA).
A total of 416 consecutive patients admitted to the neurorehabilitation unit were screened for eligibility over a 16-month recruitment period. Of the 156 patients assessed as eligible for study participation, 92 provided written consent and were randomly assigned either to the intervention (n = 46) or the control (n = 46) groups. During the study, 6 participants (3 in each group) were lost to follow-up, as they were either uncontactable or deceased (Fig. 1). The mean duration of the enriched programme was 11 days (range 9–21 days). There was 96% compliance with the treatment programme, as per the a priori compliance definition. No adverse events were reported.
Fig. 1. Flow chart of study recruitment process.
Sociodemographic and clinical characteristics
Sociodemographic and clinical details of the participants at baseline are shown in Table I. The majority of participants were male (n = 55, 60%) and Caucasian (n = 76, 82.6%) with a mean age of 63.3 ± 16.4 (range 22.2–94.3) years. The main diagnosis of participants in both groups was stroke (n = 75, 81.5%), followed by MS and brain tumours. There were no statistically significant differences between the groups in sociodemographic or clinical characteristics at baseline. However, there were more participants with lower limb impairment who required assisted transfers in the control group than in the intervention group. The study sample presented with a significant number of comorbidities, predominantly hypertension and diabetes. The majority of participants in both groups were reported to have some cognitive issues, fatigue and pain, and most required a walking aid (Table I).
Table I. Socio-demographic characteristics of participants (n = 92)
Main outcomes
Short-term effects (at discharge T1). At discharge, there was a significant between-group difference in favour of the intervention group, in UL function improvement, measured by ARAT “Total” (mean difference (MD) = 10.6, 95% confidence interval (95% CI) –17.1, –4.1, p = 0.002, with small effect size (η2) = 0.11), and “Grip”, “Pinch” and “Gross” subscales (p < 0.05 for all) with small magnitude η2 = 0.04–0.16). Most (82.6%) EE group participants had an improvement of more than the MCID (> 5.7 points) on the ARAT, compared with only 43.5% of participants in the control group (p < 0.001) (Fig. 2). Compared with the control group, the intervention group also showed significant improvement in activities: FIM motor: “sphincter” (p = 0.019, η2 = 0.06) and “mobility” (p = 0.011, η2 = 0.07) subscales and FIM total cognition scale (p = 0.010, η2= 0.07); and participation: EQ-5D “overall health” subscale (p = 0.012, η2 = 0.07). Both groups improved in other scales of impairments, activity and participation in the shorter-term; however, these were not statistically significant between the groups. (Table II).
Fig. 2. Percentage of participants with change in Minimal Clinically Important Difference (> 5.7 points in mean) in Action Research Arm Test (ARAT) at different assessment time-points.
Long-term effects (at 3-month follow-up T2). At 3-month follow-up, there was no significant difference between the intervention and control groups in ARAT “Total” and other subscales. However, the majority (90.7%) of the EE group participants maintained the improvement of > 5.7 points (MCID) on ARAT “Total” scale compared with only 60.5% of participants in the control group (p = 0.001) (Fig. 2). Compared with the control group, a statistically significant difference was maintained in favour of the intervention group in the activity outcomes: FIM “Motor total” (p = 0.008, η2 = 0.08), “sphincter” ( p = 0.001, η2 = 0.12) and “mobility” subscale (p = 0.003, η2 = 0.10). Interestingly, participants in the intervention group reported significant improvement in EQ-5D “Mobility” subscore (p = 0.009, η2 = 0.08). No between- group difference was noted for the UL functional scores and the other subscales, including QoL and overall health of participants (Table II).
Table II. Summary of per protocol analysis of outcomes
Long-term effects (at 3-month follow-up T2). At 3-month follow-up, there was no significant difference between the intervention and control groups in ARAT “Total” and other subscales. However, the majority (90.7%) of the EE group participants maintained the improvement of > 5.7 points (MCID) on ARAT “Total” scale compared with only 60.5% of participants in the control group (p = 0.001) (Fig. 2). Compared with the control group, a statistically significant difference was maintained in favour of the intervention group in the activity outcomes: FIM “Motor total” (p = 0.008, η2 = 0.08), “sphincter” ( p = 0.001, η2 = 0.12) and “mobility” subscale (p = 0.003, η2 = 0.10). Interestingly, participants in the intervention group reported significant improvement in EQ-5D “Mobility” subscore (p = 0.009, η2 = 0.08). No between- group difference was noted for the UL functional scores and the other subscales, including QoL and overall health of participants (Table II).
Subgroup analysis – stroke
The main diagnosis of the majority of participants (n = 75, 82%) in both groups was stroke. At discharge, in sub-group analyses of stroke participants, overall UL function improved significantly in the intervention group compared with the control group: ARAT “total”, “Grasp”, “Grip”, “Pinch” and “Gross” subscales (p < 0.05 for all). However, this was not maintained at the 3-month follow-up in both groups. Estimated difference in scores between intervention and control groups was significantly in favour of the intervention group with stroke in FIM “sphincter” subscale at both T1 (p = 0.023) and T2 (p = 0.003); and mobility subscales at T2 (p = 0.035). At both assessment time points (T1 and T2) those in the intervention group indicated improvement in their overall health (EQ-5D “overall health” (p < 0.05). No difference between groups was noted for other subscales (Table III).
Table III. Estimated difference scores of outcomes variables between the intervention and control groups on stroke patients
Participants’ involvement in the activities
Compared with the control group, participants in the intervention group were more likely to be involved in some type of daily activity during observed waking hours in the ward outside therapy time (mean 4.1 ± 2.1 vs 3.0 ± 1.4 times/day, MD –1.1, 95% CI –1.8 to –0.3, p = 0.006). Specifically, intervention group participants were engaged significantly more in physical and cognitive activities (p < 0.001 for both). Furthermore, participants in the intervention group spent less of their day inactive or sleeping than the control group; however, this difference was not statistically significant (p > 0.05) (Table IV, Fig. 3).
Table IV. Total activities performed daily by the participants in waking hours during inpatient stay*
Fig. 3. Between-group comparisons of participants’ mean daily activity in ward during waking hours.
Participants’ satisfaction with the programme
More than two-thirds of the participants (n = 38, 82.6%) were satisfied with the programme, and 91.3% indicated that they would recommend the service to others. The majority (83.8%) reported that the programme helped them to better or somewhat better manage their condition, 84.8% reported their activities had improved and 91.3% reported that they were coping better since they received the service. Ninety-six percent were satisfied with the staff and 81.3% were satisfied with the content of the programme.
To our knowledge this study was first to examine the efficacy of a technology-assisted EE programme for UL functional activities, within an interdisciplinary rehabilitation service model for inpatients with neurological conditions. This RCT found that such a programme was feasible for implementation in busy inpatient rehabilitation settings, and was a resource-efficient method for improving inpatient rehabilitation experience and outcomes. The findings demonstrate a beneficial effect of EE in improving UL function of the affected arm measured by the ARAT, specifically in the grip, pinch and grasp functions at discharge (post-implementation). The improvement (mean change over 10 points) was almost twice the level that is considered to represent a MCID of > 5.7 points. More than two-thirds (83%) of the intervention group participants had clinically significant improvement (> 5.7 points) compared with less than half (44%) of the participants in the control group. This might have translated to participants in the intervention group being more likely to be engaged in activity during waking hours in the ward than those in the control group. However, most of these improvements were not sustained at 3-month follow-up. At T2, the majority of the intervention group maintained the improvement > 5.7 points on the ARAT scale compared with the control group (91% vs 61%). These findings were similar for the sub-group analysis of persons with stroke. Both non-parametric and parametric analyses showed very similar results. The programme was well-tolerated by participants, and more than 90% reported satisfaction.
The overall beneficial effects of EE in this study are consistent with previous studies of EE programmes (15, 26, 36, 37). In our previous RCT (26), we reported favourable impact of the “Activity Hub” on functional and cognitive functions (such as depression, anxiety, stress); coping and self-management skills in an inpatient neurological cohort. In this study, we utilized additional inexpensive user-friendly devices (such as NAO robot, Sphero SPRK+ ball games), specifically targeting use of UL function to motivate and encourage patients to use their affected arm wherever possible. These innovative devices are relatively new and have not yet been fully evaluated in the EE setting. Furthermore, another study (9) evaluated the use of UL exercise devices (computer game based) (ReJoyce, Able-X, Able-M) in a medically supervised “Hand Hub” programme within an ambulatory neurological setting, and was shown to be feasible with good clinical outcomes (9).
In contrast to our previous trial (26), this study did not find significant between-group difference in improvement in overall physical function (apart from UL function) and cognitive function. Both the intervention and control groups showed significant improvement in their functional activities and cognitive functions assessed using the FIM (Motor-and Cognitive subscale), MoCA, MHLC, RSEC, demonstrating the efficacy of inpatient interdisciplinary rehabilitation programme. No between-group difference was found for most of these scales, which may be due to the selection of the patient group, variability in demographic and clinical characteristics, and content and intensity of physical and social components of rehabilitation programme. Variability of age and duration of exposure to EE have been shown to affect the outcome of enriched housing conditions in animal models (38). However, UL functions tended to be significantly improved in the intervention group, demonstrating that repetitive and extra treatment for UL had additional benefit at least during their inpatient stay. UL function is fundamental for daily activities, which has positive correlation with the QoL of patients. Furthermore, this study also demonstrated that the EE programme was effective in increasing daily activities and reducing time spent inactive and alone in waking hours in the ward.
The current study used a wide range of measures (such as FIM, ARAT) representing impairment, activity and participation. It is questionable that an effect of intervention on these different constructs of the ICF would have been missed, as many of the selected outcome measures, such as FIM, ARAT showed a celling effect. This is consistent with other studies using similar measures (26, 39, 40). As expected, the general trend was that all participants improved over time after a comprehensive rehabilitation programme. Although the UL function improvements were similar in both groups at 3-month follow-up, there might have been a difference in the daily use of the hand and arm that we were not able to address and which was beyond the scope of this study. However, the improvement in UL function might have reflected in the overall improvement in the functional scores (FIM, RES) and overall health (EQ-5D). Although the intervention group attained an additional 1–2 h of activity time specifically focused on UL functions, the possibility of different amounts of UL training being received by the control group cannot be ruled out, because the inpatient rehabilitation programme is individualized based on the individual needs. We were also not able to record the intensity, treatment modalities and amount of time devoted specifically to UL training within the prescribed treatment schedules. However, the comprehensive rehabilitation programme offered standard treatment, consistent with current management guidelines, hence; it is unlikely to have provided sufficient variation in therapy between groups.
Study limitations
This study has some limitations. First, it was a single-centre study with a limited number of selected participants, who volunteered to participate in the study. Secondly, as the study was conducted at the ward level, blinding of the participants was not possible, hence some contamination cannot be ruled out. Furthermore, the intervention group participants had up to 2 h of extra activity under the supervision of the healthcare professionals, which may have been reflected in improvement in their performance and behaviour (Hawthorne effect). This might raise the question of the generalizability of the findings to other populations. The number and type of activity tasks in the “Acti-vity Hub” were different amongst the participants, as participants were encouraged to choose their own activities. However, the majority of the participants participated in robot-assisted UL group-therapy. Capturing the activity log every hour daily was challenging and labour-intensive, as participants were involved in various programmes and other ward activities. However, activity levels were recorded throughout the day across usual waking hours for all participants irrespective of their group allocation by blinded assessors. We were not able to gather activity duration, daily activity log during weekends (Saturday and Sunday) and post-discharge, as this was not feasible and was beyond the scope of this study. Furthermore, no strict definition of activity (physical, cognitive, social) was implied and all forms of purposeful activities were recorded using a structured form (15). The methodological limitations of this study indicate the need for a larger multi-centre RCT to establish the role of EE in improving patient-centred outcomes.
Conclusion
The “Activity-Hub” EE programme improved capacity in the provision of rehabilitation therapy and UL activities for people with neurological disability by providing additional activities. This innovative programme enhanced the quality of acute rehabilitation by addressing problems (both physical and cognition) of critical importance to patients, making inpatient rehabilitation more efficient. The findings suggest that the EE programme increased the amount of time involved in therapeutic activities, i.e. reducing time spent inactive, and improved physical (UL) and overall patients’ QoL. Participant UL function after the EE programme only improved during the inpatient stay and tended not to be sustained after discharge or in-home settings where such facilities are not available. This is important and needs exploring in further research. The programme increased participant engagement and provided oppor-tunities for socialization, interaction with their peers to improve self-efficacy, coping and self-management skills. Furthermore, it also provided a platform for participants for interaction with healthcare professionals, which helped them to increase knowledge and enhance self-confidence/self-esteem, potentially leading to improved QoL. Another unique aspect of this study is that it demonstrated the importance of UL training, which receives less attention in most rehabilitation settings. Future research is required to confirm the findings through the incorporation of EE programme in community settings with a larger sample size.
The authors are grateful to all participants in this study and thank the staff of the rehabilitation ward of the Royal Park Campus, Royal Melbourne Hospital. In particular, the authors thank Loren Oscari and Dimitrios Tsavios for patient assessments and data entry.
Financial disclosure
This review was supported from internal resources of the Rehabilitation Department, Royal Melbourne Hospital, Australia. No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors or upon any organization with which the authors are associated.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize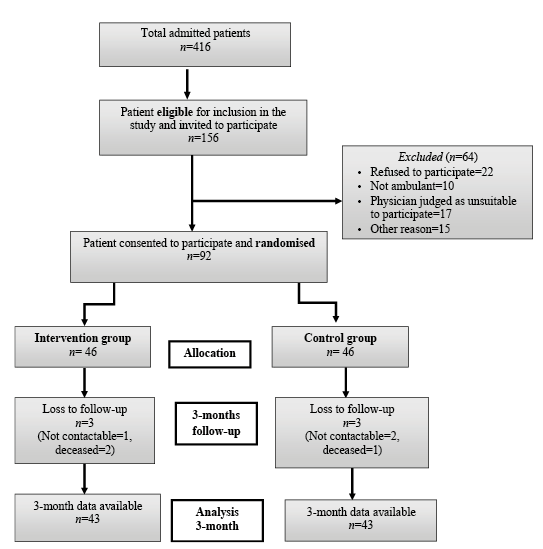 Click to show fullsize
Click to show fullsize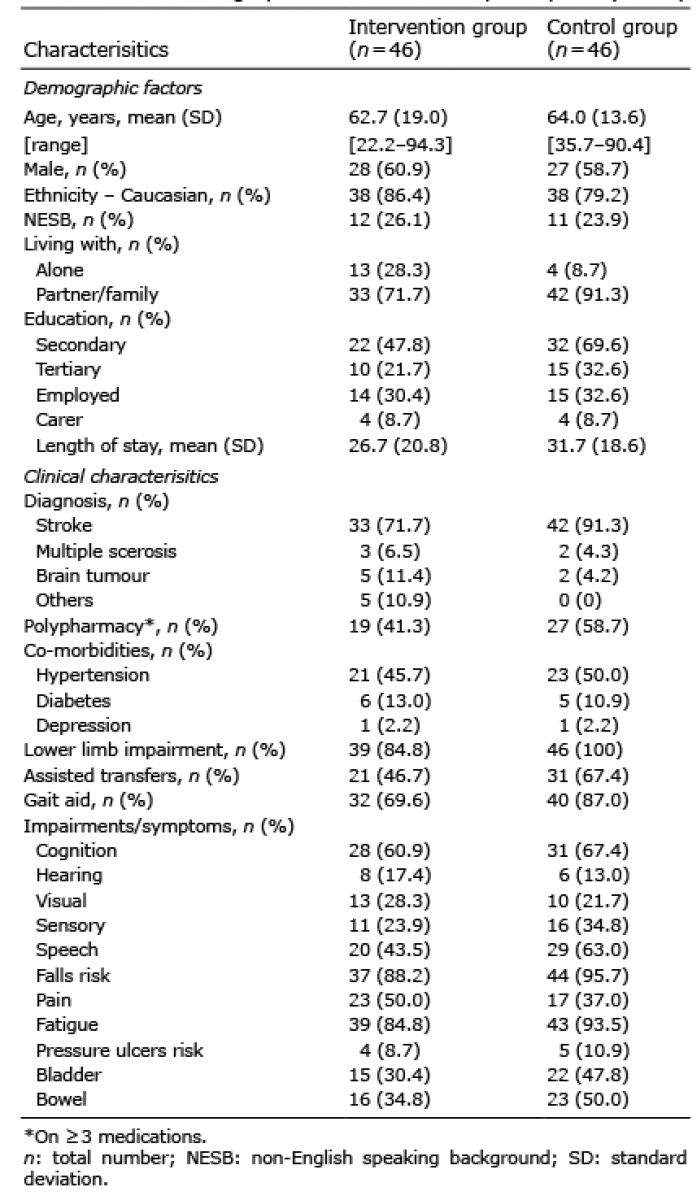 Click to show fullsize
Click to show fullsize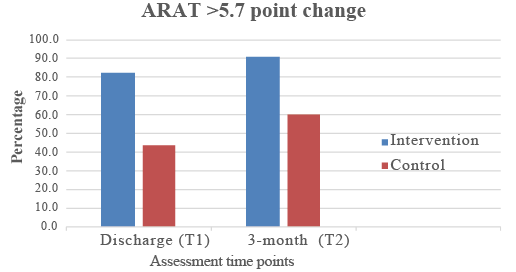 Click to show fullsize
Click to show fullsize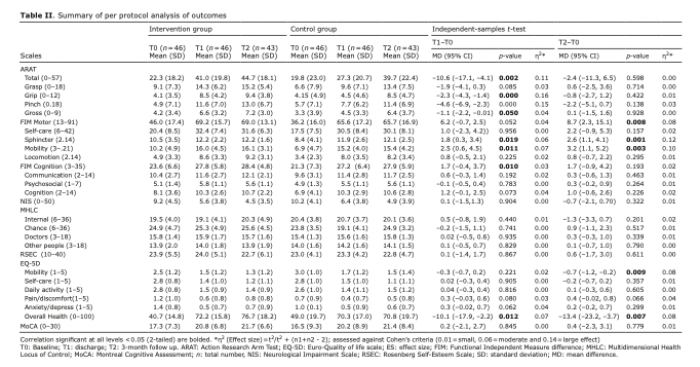 Click to show fullsize
Click to show fullsize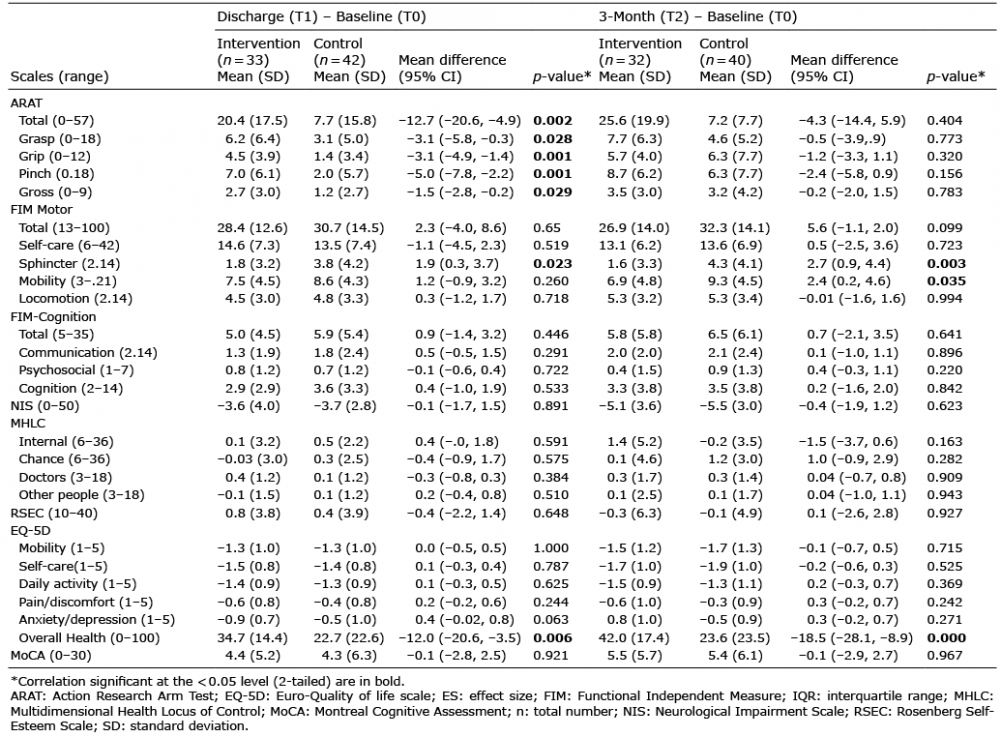 Click to show fullsize
Click to show fullsize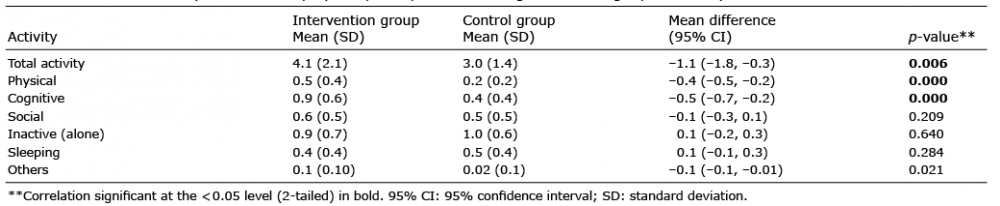 Click to show fullsize
Click to show fullsize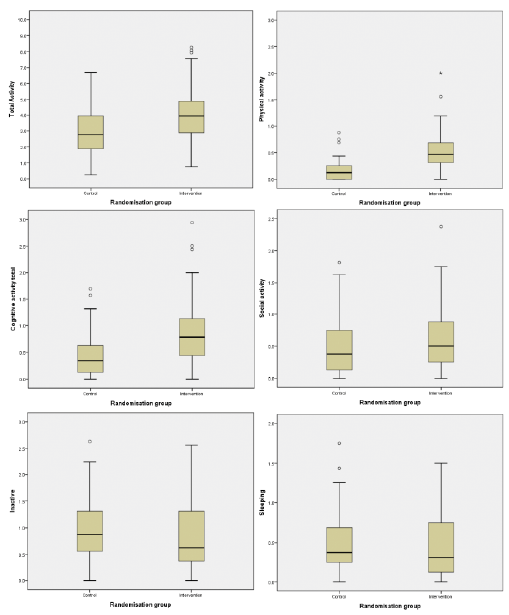 Click to show fullsize
Click to show fullsize