
From the 1Department of Rehabilitation Medicine, Hannover Medical School, Hanover, Germany, 2Department of Mental and Physical Health and Preventive Medicine, University of Campania “Luigi Vanvitelli”, Naples, Italy, 3University of Bielefeld, School of Public Health, Bielefeld, Germany and 4Physical and Rehabilitation Medicine, University Hospitals Leuven, Leuven, Belgium
Objective: To develop a revised version of the International Classification of Service Organization in Rehabilitation (ICSO-R).
Design: Qualitative study.
Methods: The revision was based on testing the first version of the ICSO-R; 2 discussion rounds invited by the ICSO-R working group of the Standardized Rehabilitation Reporting Subcommittee of the World Health Organization Liaison committee of the International Society of Physical and Rehabilitation Medicine, and a call for corrections from a group of international experts.
Results: The resulting ICSO-R 2.0 version is composed of 2 dimensions (formerly 3); the Provider dimension and the Service delivery dimension. The categories of the Funding dimension from the first version of ICSO-R were incorporated into each of the other dimensions. The Provider dimension now consists of 9 categories and the Service delivery dimension consists of 14 categories. Subcategories have been added to 7 categories: governance/leadership, funding of provider, target groups, location of service delivery, setting, rehabilitation team, and funding of service delivery.
Conclusion: This updated version of ICSO-R provides a prerequisite for rehabilitation service organization assessment and implementation projects, reporting of contextual influences in clinical trials and many other aspects. In addition, ICSO-R 2.0 can be used for several purposes, e.g. to analyse and compare the provision of rehabilitation services in health systems and to support the quality management of rehabilitation services. However, the development of value sets for each (sub)category and further validation studies are still needed.
Key words: health-related rehabilitation; service organization; rehabilitation; health system; health service; classification.
Accepted Oct 30, 2019; Epub ahead of print Nov 13, 2019
J Rehabil Med 2020; 52: jrm00004
Correspondence address: Boya Nugraha, Department of Rehabilitation Medicine, Hannover Medical School, Carl-Neuberg-Str.1, 30627-Hannover, Germany. E-mail: boya.nugraha@gmail.com
Rehabilitation services should be available worldwide for every person who has problems with functioning. Thus, rehabilitation services must be organized at all levels of healthcare, from the community, through primary care to general and specialized hospitals. Rehabilitation services are needed along the continuum of care: from acute, through post-acute to the chronic phase. In order to plan these services a classification system is needed to describe, in a uniform way, the different types of services and their characteristics. The second version of the International Classification System for Service Organization in Rehabilitation (ICSO-R 2.0), described in this paper, comprises 9 categories describing the provider of the service and 14 categories concerning service delivery. ICSO-R 2.0 will enable improved description of available service organization and facilitate the identification of rehabilitation service provision worldwide. Thus, the updated ICSO-R 2.0 will benefit all persons in need.
Rehabilitation is one of the 5 major health strategies (1). From a historical point of view and in light of demographic shifts and trends in epidemiology, rehabilitation can be regarded as the health strategy of the 21st century (2). This implies that rehabilitation is required for persons who have disabling health conditions, as a consequence of severe disease, trauma, surgery, chronic progressive disease or the effects of ageing (2, 3).
From the perspective of the health system, rehabilitation should be one of the services provided as a matter of course within health systems worldwide (4). Rehabilitation services should be available for every person in need (5), and rehabilitation is an integral part of Universal Health Coverage (6). In its recommendations “Rehabilitation in Health Systems” (1) the World Health Organization (WHO) stresses that rehabilitation services must be implemented both in hospitals and in the community. There is also a consensus that rehabilitation must include acute, post-acute and long-term services, as well as services at the primary, secondary and tertiary level of healthcare (1, 7).
However, there is no uniform understanding of what constitutes a (qualified) rehabilitation service and of a framework to describe rehabilitation services at an organizational level in a standardized way. Such descriptions are essential for the many purposes listed here:
The first version of the ICSO-R provided a set of dimensions and categories to describe and compare service organization in health-related rehabilitation services at the regional, national and international level. It included 3 dimensions, comprising a total of 20 categories (11). These dimensions were:
The first proposal for dimensions of the ICSO-R (11) was tested at European and national levels (10, 15–17). In addition, a couple of unpublished applications of the first version of the ICSO-R were conducted in different settings and countries. Some of the issues arising in the application of ICSO-R within these projects were:
In conclusion, it was obvious that there was a need for revision of the ICSO-R. Thus, the ICSO-R working group of the International Society of Physical and Rehabilitation Medicine (ISPRM) took the initiative to develop a revised version. This paper presents the results of a revised version of the ICSO-R, namely ICSO-R 2.0, which was developed through an iterative testing, consultation and expert consensus process.
The revision of the proposed dimensions and categories of the ICSO-R, as published by Gutenbrunner et al. (13), was based on the following steps:
In addition, the recommendations of a working group of the Norwegian Research Centre for Habilitation and Rehabilitation Models and Services (CHARM), who tested the ICSO-R in Norway (16), were taken into account. They suggested, for example, differentiating between funding of the provider and the service itself. Finally, the results of an initial testing of the ICSO-R in Malaysia were integrated (10).
The ICSO-R working group developed a revised version by discussing every dimension and category on the background of the different comments received during the process described above. They also added a description for every domain and category, as well as inclusions and exclusions (following the style of the International Classification of Functioning, Disability and Health (ICF) (18).
The draft version (ICSO-R 2.0ß) was sent to 12 experts in the field of Rehabilitation Medicine and Rehabilitation Systems Analysis for comments. This group of experts also included native English speakers who were asked for language corrections. Ten persons responded, giving a total of 80 comments and proposals. Each of these comments was discussed one by one by the group of authors, and either included, adopted, or rejected based on supportive arguments. In some cases, new solutions were developed, integrating the expert’s proposals and the wording of the ICSO-R 2.0ß version. Interference with other categories was cross-checked. In case of unclear terminology a further term-specific literature search was performed or other experts (e.g. from the field of economy and management) were consulted. The resulting version was sent to another native English speaker for a further round of language correction.
The development of value sets and recommendations for measures and scales were not included at this stage, and will be addressed in a follow-up project.
3.1. Short and extended list of dimensions, categories and subcategories
Like the first version, ICSO-R 2.0 also consists of 2 levels: dimensions and categories (and subcategories). The third level, value sets, remains to be developed.
The main difference from the first version, which included 3 dimensions, is that ICSO-R 2.0 comprises only 2 dimensions: Provider and Service delivery.
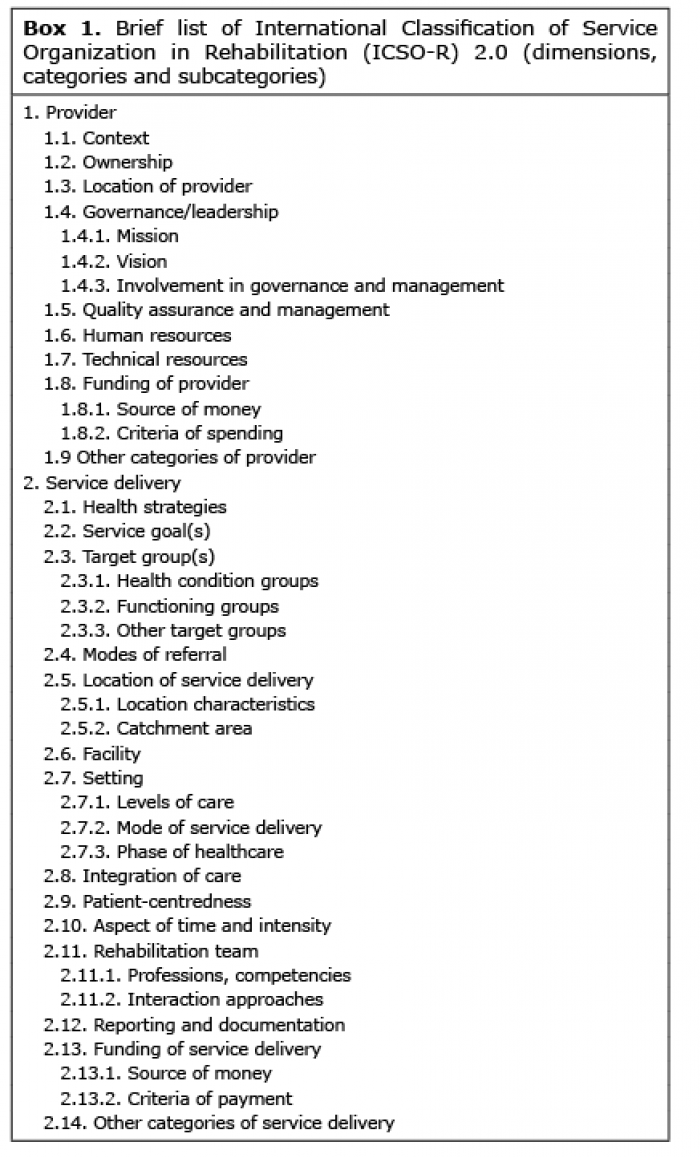
This is due to the decision to incorporate the categories that were included in the former dimension of “Funding” into each of the other dimensions. The Provider dimension now comprises 9 categories and the Service delivery dimension comprises 14 categories. Subcategories have been added to 7 categories (2 in the Provider dimension and 5 in the Service delivery dimension) (Box 1). For all dimensions, categories, and subcategories, a general description, as well as inclusions and exclusions were included. ICSO-R 2.0ß, with its new dimensions, categories and subcategories, as well as the explanations, inclusions and exclusions, are as follows:
Box 1. Brief list of International Classification of Service Organization in Rehabilitation (ICSO-R) 2.0 (dimensions, categories and subcategories)
1. Provider dimension
Organizational units with the primary goal to provide rehabilitation services
Inclusions: Rehabilitation departments of larger hospitals, units within larger multi-purpose departments, stand-alone rehabilitation units (rehabilitation clinics and centres, single practices), and rehabilitation services provided in the community.
Exclusions: Hospitals or other organizational units that do not provide rehabilitation services as primary goal.
1.1. Context
Context describes whether the provider is independent or embedded in a parent or larger organization and how the context is organized.
Inclusions: Independent unit, hospital, university, community, network of organizations, or another umbrella organization.
Exclusions: Ownership (1.2), location of provider (1.3).
1.2. Ownership
Legal and contextual characteristics of the owning entity.
Inclusions: Public body (e.g. government, administration), private non-profit organization (e.g. non-governmental organization (NGO), charity organization), private for-profit organization (owned by shareholders or private investor/s), or combination of owning entities (public-private partnership).Exclusions: Governance /leadership (1.4), mission (1.4.1), vision (1.4.2), involvement in governance and management (1.4.3), facility (2.6), setting (2.7).
1.3. Location
Place where the provider is located.
Inclusions: Place of legal registration of the provider (city, country).
Exclusions: Location of service delivery (2.5).
1.4. Governance/leadership
Political, economic, and administrative authority in the management of the provider.
Inclusions: Mission (1.4.1), vision (1.4.2), involvement in governance and management (1.4.3), advocacy for support, resources and funding (both Provider and Service delivery level).
Exclusions: Context (1.1), ownership (1.2).
1.4.1. Mission
Statement that specifies an organization’s purpose and reason for being, outlining what the provider wants to do now or concentrates on at present. Inclusions: Goals of the provider beyond the service delivery (e.g. education, training, research), advocacy for support, resources and funding. Exclusions: Vision (1.4.2), involvement in governance and management (1.4.3), service goals (2.2), target group(s) (2.3).
1.4.2. Vision
Statement that answers the questions “where are we going?” and “what can we achieve?”; outlining what the provider wants to do in the future.
Inclusions: Long-term goals and directions; aspects of core values and culture.
Exclusions: Mission (1.4.1), involvement in governance and management (1.4.3).
1.4.3. Involvement in governance and management
People and bodies involved in the decision-making process.
Inclusions: Medical and/or economic leaders and/or elected bodies and/or others; formal involvement of users or user groups in governing bodies.
Exclusions: Quality assurance and management (1.5); patient-centeredness (2.9).
1.5. Quality assurance and management
Activities and programmes, promoted by the owner or provider, intended to assure or improve the quality of service delivery.
Inclusions: Assessment or evaluation of the quality of service delivery, identification of problems or shortcomings in service delivery, designing activities to overcome these deficiencies, and follow-up monitoring to ensure effectiveness of corrective steps; any systematic way to pursue quality assurance activities (internal and external), including accreditation/certification, audit; appointed quality manager; single interventions with the explicit aim to improve structure/process/outcome quality.
Exclusions: Any non-systematic (i.e. occasional, non-planned) approach.
1.6. Human resources
Spectrum of staff/personnel (different types of health professionals, administrative staff, technical staff, researcher, and other personnel) within the provider. Inclusions: full-time-equivalents of staff, affiliated and supportive staff, regular volunteers.
Exclusions: retired personnel, volunteers not involved on a regular basis, family or informal caregivers, competencies of the rehabilitation team (2.11).
1.7. Technical resources
Equipment and infrastructure available for service delivery.
Inclusions: Diagnostic, therapeutic and assistive devices, data processing and communication devices, and other affiliated technical resources; reporting and documentation platform.
Exclusions: Facility (2.6).
1.8. Funding of provider
Financial resources and criteria of spending for indirect funding of the provider.
Inclusions: Source of money (1.8.1), criteria of spending (1.8.2).
Exclusions: Funding of service delivery (2.13).
1.8.1. Source of money
Organization(s) providing money for indirect funding.
Inclusions: Government, community, investor(s), charity or other organization(s), insurance company, foundations, others.
Exclusions: Criteria of spending (1.8.2), source of money for service delivery (2.13.1).
1.8.2. Criteria of spending
Rules and regulations for spending of the funded money.
Inclusions: Budgets for human and technical resources, infrastructures, consumables, and goods. Exclusions: Criteria of payment for service delivery (2.13.2).
1.9. Other categories of provider.
2. Service delivery dimension
Offer of set of products (interventions, procedures, devices, pharmaceuticals and other goods, etc.) to a specified group of persons (patients, informal caregivers and/or other users or clients) aiming at achieving or maintaining optimal functioning (rehabilitation) within an organizational context (provider).
Inclusions: Characteristics of service delivery, such as health strategies (2.1), service goals (2.2), target group(s) (2.3), modes of referral (2.4), location of service delivery (2.5), facility (2.6), setting (2.7), integration of care (2.8), patient-centeredness (2.9), aspect of time and intensity (2.10), rehabilitation team (2.11), reporting and documentation (2.12), funding of service delivery (2.13).
Exclusions: Provider (1); direct intervention or application of a treatment.
2.1. Health strategies
Other health strategies in addition to rehabilitation strategy, to achieve and maintain the health, including functioning of a group of persons with rehabilitation needs.
Inclusions: promotion (promotive strategy), prevention (preventive strategy), treatment (curative strategy), maintenance (supportive strategy), palliation (palliative strategy), and/or other health strategies. Exclusions: Service goals (2.2), target group(s) (2.3).
2.2. Service goals
Objectives or purposes that a rehabilitation service envisions, plans and commits to achieve; the desired or possible outcomes of the service delivered. Inclusions: Recovery, improvement of health status, optimizing functioning (e.g. improvement of self-care, return to normal life, return to home, return-to-work) or other service goals.
Exclusions: Individual patient’s goals; mission (1.4.1).
2.3. Target group(s)
Groups of people with rehabilitation needs and their caregivers for which the service is delivered. Inclusions: Patients with any or specific health condition(s), persons with any or specific impairment, activity limitations and/or participation restrictions, and other target group(s), such as age-related groups, formal or informal caregivers.
Exclusions: Students, residents, researchers.
2.3.1. Health condition
Groups of people with a defined health condition for which rehabilitation services are provided. Inclusions: Stroke, traumatic brain injury (TBI), multiple sclerosis (MS), spinal cord injury (SCI), limb loss, low back pain, and others.
Exclusions: Functioning (2.3.2), other target groups (2.3.3).
2.3.2. Functioning
Groups of people with defined functioning problems for which rehabilitation services are provided.
Inclusions: Gait, balance, spasticity, vocational, car driving, cognition, and others.
Exclusions: Health condition (2.3.1), other target groups (2.3.3).
2.3.3. Other target groups
Specific groups of people for which rehabilitation services are provided.
Inclusions: Groups of people with rehabilitation needs: children, elderly people, athletes, musicians, refugees, ethnic groups, workers, and others.
Exclusions: Health condition (2.3.1), functioning (2.3.2).
2.4. Modes of referral
How the user accesses the service.
Inclusions: Direct access (patients’ self-referral), referral by health professionals, health services, or other persons or organizations.
Exclusions: Criteria of payment (2.13.2) or other financial aspects of accessibility; facility (2.6) including physical accessibility; reservation/registration process.
2.5. Location of service delivery
Location characteristics of the place and the catchment area of service delivery.
Inclusions: Rural area, urban area, community, centralized, decentralized (affiliated services, home of users, e-communication networks).
Exclusions: Address.
2.5.1. Location characteristics
Location characteristics of the place where the service is delivered.
Inclusions: Rural area, urban area, community, centralized, decentralized (affiliated services, home of users, e-communication networks).
Exclusions: Catchment area (2.5.2).
2.5.2. Catchment area
The area where most of the patients come from. Inclusions: Population, geographical area, administrative area.
Exclusions: Location characteristics (2.5.1).
2.6. Facility
Facilities of service delivery.
Inclusions: Building, and other aspects of facilities, such as laboratories, diagnostic and therapy rooms, beds, etc., catering and laundry services, physical accessibility.
Exclusions: Location of provider (1.3), location of service delivery (2.5).
2.7. Setting
Levels of care, mode of service delivery, and phase of healthcare under which rehabilitation interventions take place.
Inclusions: levels of care (2.7.1); mode of service delivery (2.7.2); phase of healthcare (2.7.3).
Exclusions: Location of provider (1.3), location of service delivery (2.5).
2.7.1. Levels of care
The degree of specialization of care provided by rehabilitation health professionals.
Inclusions: Primary, secondary, and tertiary levels of specialization.
Exclusions: Mode of service delivery (2.7.2), phase of healthcare (2.7.3), aspects of time and intensity (2.10).
2.7.2. Mode of service delivery
The way services are delivered to the users.
Inclusions: Inpatients, outpatients, day hospital/day service, home and community, tele-rehabilitation, or any other setting for service delivery.
Exclusions: Levels of care (2.7.1), phase of healthcare (2.7.3).
2.7.3. Phase of healthcare
Types of rehabilitation services responding to patients needs in different phases of their health conditions.
Inclusions: Habilitation, pre-habilitation, acute rehabilitation care, sub-acute rehabilitation care, post-acute rehabilitation care and long-term/chronic rehabilitation care.
Exclusions: Levels of care (2.7.1), mode of service delivery (2.7.2).
2.8. Integration of care
The management of delivering rehabilitation services in conjunction with other health services so that people receive timely, comprehensive and well-coordinated care, according to their needs and across different levels (vertical integration) and along the continuum of care (horizontal integration).
Inclusions: Continuum of care, admission and discharge planning, collaboration of health professionals, shared electronic patients’ records.
Exclusions: Modes of referral (2.4), setting (2.7), levels of care (2.7.1), mode of service delivery (2.7.2), phase of healthcare (2.7.3), patient-centredness (2.9), rehabilitation team (2.11).
2.9. Patient-centredness
Rehabilitation tailored on the person’s needs and provided in partnership with them, their families and communities.
Inclusions: Shared decision-making, individual rehabilitation plan, patient, family or other caregiver’s education and empowerment, patient family or other caregiver’s integration in the rehabilitation process, involvement of peer counsellors, involvement of patients as prosumers.
Exclusions: Service goals (2.2), modes of referral (2.4), setting (2.7), integration of care (2.8), aspects of time and intensity (2.10).
2.10. Aspects of time and intensity
Time schedule of service provision and interventions.
Inclusions: Length of stay or treatment period, intermittent vs continuous treatments, duration of single treatments, number and duration of treatment sessions, and total duration of treatment, service hours.
Exclusions: Any aspects of time related to service organization, such as years since funding of the organization, phase of healthcare (2.7.3).
2.11. Rehabilitation team
Professions and competencies of rehabilitation team members; team structure and methods of team communication.
Inclusions: Health and health-related professionals delivering services to the users (patients), peer counsellors, and others, multi-professional team composition, interdisciplinary way of working, etc., patients as part of the rehabilitation team and team supervision, counselling, etc.
Exclusions: Administrative staff, technical and maintenance staff (exception: rehabilitation engineers), cleaning staff.
2.11.1. Professions, competencies
Range of competencies of health and health-related professionals or appropriately skilled non-professionals involved in the rehabilitation team, delivering services to the users, and competencies necessary to deliver rehabilitation interventions.
Inclusions: Knowledge, skills, experience, types of professions of team members (Physicians, PRM specialists, Physiotherapist, Occupational Therapists, Speech and Language Therapists, Prosthetist & Orthotists, Nurse, Social Workers, Psychologists, Community-based rehabilitation workers, and other professionals interacting with the patient/user).
Exclusions: Professionals who have no or only administrative contact with patients (e.g. manager, administrative staff).
2.11.2. Interaction approaches
Team interaction and methods of team organization and communication pathways.
Inclusions: Multi-professional team, inter-professional team, team supervision, counselling etc., meetings of the whole team, team integrated education and training, immediate or delegated team involvement.
Exclusions: Interrelation with staff outside rehabilitation team, patient-centredness (2.9), reporting and documentation (2.12).
2.12. Reporting and documentation
Health and functioning parameters in individual patient records.
Inclusions: Content of patient records (including dimensions such as ICF domains with consideration of established clinical assessment schedules, ICD domains), reporting of outcomes, methods of documentation (e.g. electronic records, paper documents). Exclusions: Quality assurance and management (1.5), service goals (2.2), service organization related outcomes, such as economic data, working times, use of resources, etc.
2.13. Funding of service delivery
Payment for service delivery (diagnostics, treatments, etc.).
Inclusions: Characteristics of service delivery funding, such as source of money (2.13.1) and criteria of payment (2.13.2).
Exclusions: Funding of provider (1.8).
2.13.1. Source of money
Origin of funding of operating budget.
Inclusions: State funding, health insurance, other insurances, charity organizations, out of pocket (paid by users’ money) and other sources and modalities of payment (e.g. barter, donations). Exclusions: Funding of provider (1.8); criteria of payment (2.13.2).
2.13.2. Criteria of payment
Rules and regulations for payment of service delivery.
Inclusions: Institutional funding, diagnosis related group-system, day-based payment, fee for single service, episode of care, fixed budget or other, other. Exclusions: Funding of provider (1.8); source of money (2.13.1).
2.14. Other categories of service delivery
3.2. Principles of changes in structure of ICSO-R 2.0
Fig. 1 shows the interrelation of classifications relevant for rehabilitation at the macro-, meso- and micro-level of health systems (left) and the contents of the ICSO-R 2.0 dimensions (right). It clarifies that ICSO-R is designed to describe or classify rehabilitation services at the meso-level of health systems. Thus, it does not cover aspects of the health system at the macro-level, such as health service delivery, health workforce, health information systems, access to essential medicines, health systems financing, or leadership and governance. These are described in the WHO Health System building blocks or tools describing the provision of rehabilitation in health systems, such as the WHO tool “Systematic Assessment of Rehabilitation Situation (STARS)” (19) or the Rehabilitation Service Assessment tool (RSAT) published by Gutenbrunner & Nugraha (9). Another important interface is with the micro-level of service delivery. Here, the International Classification of Health Interventions (20), the WHO International Classifications of Diseases (ICD) and the International Classification of Functioning, Disability and Health (ICF) as well as defined rehabilitation programmes are relevant. Thus, to obtain a complete picture, different classifications must be used; however, the ICSO-R closes a relevant gap between the macro- and micro-level of health systems in rehabilitation.
Fig. 1. Overview of the interrelation of classifications relevant to rehabilitation at the macro-, meso- and micro-level of health systems (left) and the contents of the International Classification of Service Organization in Rehabilitation version 2.0 (ICSO-R 2.0) dimensions (right). STARS: Systematic Assessment of Rehabilitation Situation; ICHI: International Classification of Health intervention; ICD: International Statistical Classification of Diseases and Related Health problems; ICF: International Classification of Functioning, Disability and Health.
An important clarification in the use of the ICSO-R is that a single provider may deliver different services (e.g. a single department that delivers in-patient and out-patient services or specialized programmes for different target groups; see Fig. 2). Another aspect demonstrated in the Fig. 2 is that the “Provider” dimension includes the owner of a service organization and the unit that delivers services. Here too, a single owner may have more than one unit (department) and one department can be owned by more than one organization.
Fig. 2. Interrelation between ownership (ICSOR 2.0 category: context), service delivering department (ICSO-R 2.0 dimension: Provider) and services (ICSO-R 2.0 dimension: Service delivery).
Short explanations, inclusions and exclusions were added to all all dimensions, categories and subcategories. This follows the standard of the ICF (18). In addition, the inclusions and exclusions are not necessarily complete or exhaustive. The intention behind adding explanations, inclusions and exclusions was to help the users of ICSO-R 2.0 to better understand the dimension, categories and subcategories and to facilitate its use.
3.3. Changes in dimensions, categories and subcategories
The following paragraphs discuss the major changes from the first version of ICSO-R to the updated version, ICSO-R 2.0. This includes changes in the dimensions, the introduction of new categories and subcategories, and the shift of categories to other dimensions. Minor changes in wording and other corrections are not discussed. A comparison of ICSO-R and ICSO-R 2.0 categories is shown in Table I to allow for better orientation of how dimension and categories shifted from one position to another within a dimension. Table I can also be used to link the 2 versions when comparing studies performed using one of the versions.
One of the major changes from the first version of ICSO-R is that the 2 categories from the Funding domain were split into 2 different aspects of financing: one was placed under the Provider domain and describes the funding of the provider itself (see Fig. 3). This includes the funding source, which could be a government, a private investor or other, as well as the criteria for how to spend the money (e.g. budgets for technical equipment and human resources). This type of payment is described in the literature as “indirect funding” (21). The other aspect of funding is termed “direct funding” and includes payment for diagnostic measures, treatments or other services that could be paid by insurance, by the users themselves or by other sources. Here, too, the source(s) of money and the criteria for payment are independent subcategories. This was placed under the Service delivery domain. This resulted in the independent dimension of “Funding” being dissolved in the updated version of the ICSO-R. At the same time, financial aspects are described more clearly in ICSO-R 2.0. The reason for this change was that users of the ICSO-R had difficulty describing the funding process unambiguously, because in many countries investment in building up and maintaining the service facilities differs from the payment of delivered services (e.g. payment for treatments).
Table I. Comparison of dimension, categories and subcategories between the first and second versions of the International Classification of Service Organization in Rehabilitation (ICSO-R)
Fig. 3. Explanation of the new categories of the domain “Funding” and placement into the “Provider” and “Service delivery” dimensions.
The following additional categories and subcategories have been introduced into ICSO-R 2.0 after testing the first version, intensive discussion within the ICSO-R working group and a Delphi consultation with external experts:
a) Governance and leadership with the subcategories “mission”, “vision” and “involvement in governance and management”. This category was added because governance and leadership are important factors in describing an organization and can influence service delivery and outcomes (22). It also is a link to the macro-level of health systems, as leadership and governance are relevant building blocks of the health system (23). Besides the vision and mission of an organization as an important factor, the question is who is included in governance and leadership. Relevant factors could be the inclusion of team members or user groups.
b) Quality assurance and management. These are regarded as important factors in a service organization (25, 26). Quality assurance and management includes risk management and is connected with quality of structures and processes. It reduces the frequency of mistakes and defects and increases the safety of a service. Nowadays it is a mandatory factor in health service delivery in many countries (25–27).
c) Modes of referral. This is an important factor in the accessibility of a service. Modes of referral not only affects user groups, but is also relevant to understanding specific characteristics of the outcomes of a service. In many areas of the world, access to rehabilitation services is conditional on rules of the health legislation or criteria set by health and other insurance. Rules and standards of referral may be barriers to, or facilitators of, access to a service
d) Location of service delivery with the subcategories “location characteristics” and “catchment area”. It is important to understand the characteristics of the place where a rehabilitation service is located (28). Questions could be whether it is a rural or urban area, whether it is connected to public transport, and whether there are any barriers to access. These characteristics of a service can also be barriers or facilitators into which categories of environmental factors, such as healthcare institutions in the ICF, can be classified (18). Therefore, the catchment area of clients (including its population characteristics) is included in ICSO-R 2.0.
e) Setting. The setting aspect of rehabilitation services is characterized by 3 subcategories:
f) Integration of care. This category is related to the delivery of rehabilitation services that could be isolated or provided in conjunction with other health services. This would influence whether people receive timely, comprehensive and well-coordinated care. It includes coordination across different levels (so-called vertical integration) and along the continuum of care (horizontal integration).
g) Patient-centredness. There is broad consensus that rehabilitation services and programmes should be delivered in a patient-centred way (29, 30). This includes that rehabilitation goals are in line with the patient’s individual needs and expectations and the interventions are tailored on the person’s needs, and preferences are taken into account (30). This requires a defined rehabilitation plan with clear and realistic outcomes, milestones and the regular assessment of goal attainment. It should be based on shared decision-making and the integration of families, rehabilitation team, and other caregivers. In this case patients can be involved in the rehabilitation process as prosumers.
h) Rehabilitation team with the subcategories “professions, competencies”, “interaction”. Similar to the above-mentioned category, rehabilitation service delivery from multiprofessional teams is seen as a crucial factor of good rehabilitation outcomes (31). This requires an appropriate range of competencies, as well as good interaction and methods of team organization and communication pathways (32).
i) Reporting and documentation. This is relevant for treatment processes and its outcomes. These include ICD and ICF domains. The European framework corresponding to the clinical assessment schedule can also be used (33). Reporting and documentation is also related to goal setting, team work and quality assurance. For this reason, a respective category has been added. The category “facility” was shifted from the Provider dimension to Service delivery dimension. Furthermore, in the category “target groups” subcategories have been added in order to differentiate between diseases and factors of functioning that both need to be recognized in setting up rehabilitation goals and tailor interventional programmes. In addition, other aspects for groups of people with specific rehabilitation needs have been added (e.g. children, elderly people, athletes, musicians, refugees).
Subcategories have been added to the category “setting” in order to be more specific in the descriptions of the setting of rehabilitation services. These subcategories are “level of care”, “mode of service delivery” and “phases of healthcare”.
The term “Mode of production” has been replaced by “Mode of service delivery” (and integrated in the category “setting”). The reason was that this term could not be intuitively understood by the majority of users. Thus, the change will increase user friendliness and precision of outcomes for the uses of ICSO-R.
This paper presents ICSO-R 2.0, an updated version of ICSO-R, based on the various inputs received. ICSO-R 2.0 can be used as a framework to describe and compare rehabilitation services and how they are organized worldwide.
The concept of a common standardized international approach to classify/describe rehabilitation services at the organizational level corresponds to different developments and initiatives. From the health policy perspective, there is a need to provide guidance for countries on how to further develop their health systems (23), of which rehabilitation is a major pillar (5). Here, we need to develop guidance as to which rehabilitation institutions should be set up or adapted in order to meet important needs in the population. Such guidance must be based on a rehabilitation service needs assessment at the population level, so that the development or accommodation of rehabilitation services is directly related to service needs of the population in the respective countries. Also, it is crucial to have a standardized document of existing and prototype (also in terms of the minimal standard) service organizations. For planning purposes, it also seems appropriate to compile information on the cost-effectiveness of the different services, relating information on implementation and operating costs to patient-related functioning outcomes.
Taking a step back, from a health information or policy perspective, it is essential to know what kind of institutions and services are already provided in a country or defined region, and to be able to make inter-regional comparisons or comparisons over time periods in order to report changes. From a research perspective, it is essential to be able to relate the contextual factors of the setting (which can be understood as an environmental factor in the ICF (18)) to patient outcomes. The importance of contextual factors has been strongly asserted in the development, evaluation and implementation of complex interventions (12, 34) and is already listed in the respective proposal of reporting guidelines in terms of the characteristics of the setting of the intervention (35). Taking a further step back, for health services research, which often uses service variation as a point of departure, it is essential to relate the characteristics of context to the outcome of a service, as exemplified in the context + mechanism = outcome (CMO) model (36).
The use of a standardized reporting system for rehabilitation service organization may support the approach to develop rehabilitation quality management assessment (11). Together with the use of the ICF, service organization characteristics will be described more objectively.
Much has been done to develop ICSO-R 2.0, as described in the Introduction. The ICSO-R is based on an explicit definition of rehabilitation services (15). In a forthcoming publication we will compare the dimensions of ICSO-R 2.0, especially its basis in the meso-level of care, to other health classifications. We have put forward a first proposal of the ICSO-R (14) to facilitate the discussion. Various papers report experiences with the application of ICSO-R (16, 17), which were all considered in developing ICSO-R 2.0.
This methodological approach to the development of ICSO-R 2.0 has some limitations. Although we were eager to provide a sound argument by grounding our work in a conceptual framework, many steps depended on expert judgement and groups of experts that undoubtedly have a bias towards European or Western societies. We attempted attenuate this bias by the explicit inclusion of partners from low- and middle-income countries (LMICs) in case studies and in our discussion, but we foresee the need for further adaption of the ICSO-R, especially when it comes to developing the respective value sets for the different categories (see below), when tested in LMICs. Also, the methodological approach cannot rule out that we may have missed important categories of distinctions that account for substantial variation in service provision and outcome, which might reflect the underdeveloped health services research status in rehabilitation with regard to meso-level perspectives. Therefore, the “other categories”, in the dimensions of both Provider and Service delivery, is provided to facilitate such cases.
There are still many problems to resolve before ICSO-R can fulfil its promises. A next step will be to develop value sets for every category, i.e. to provide a meaningful, cross-culturally applicable, but also simple and unequivocal, way of operationalization of every aspect depicted in ICSO-R. The work of Roe et al. (17) provides valuable information for this project. Here, the different professions, competencies, traditions and available instruments and concepts must be taken into account. This version then has to be tested in different parts of the world and different healthcare systems.
A pragmatic approach to characterizing types of rehabilitation service has been developed by the Section of Physical and Rehabilitation Medicine of the European Union of Medical Specialists (UEMS-PRM-Section) in a multistage consensus process (11). This contains 14 classes of services that are characterized by different dimensions, including phase of rehabilitation care (acute, post-acute, and lifelong), specialization (general vs specialized rehabilitation), goals (vocational, social assistance) and location (community, health resorts). Using ICSO-R, these types can be described as category types (or phases) of healthcare (2.7.3), target groups (2.3), service goals (2.2) and location of service delivery (2.5). Future projects might integrate the service typology and classification approach.
Conclusion
Strengthening of health-related rehabilitation worldwide has been progressively introduced and implemented after the launch of the United Nations Convention on the Rights of People with Disabilities (UN-CRPD) in 2006 (37), the World Report on Disability in 2011 (5), the Global Disability Action Plan 2014–2021: Better Health for all People with Disability in 2014 (3) and the most recent published documents in 2017: Rehabilitation 2030 and Recommendation of Rehabilitation in Health Systems (1, 4). This should be supported by providing access to good-quality health rehabilitation services for all persons with rehabilitation needs, as it is also included in Universal Health Coverage. As there is no standardized tool to describe rehabilitation services, the ICSO-R has been developed to fill the gap of rehabilitation in the health system, particularly at the meso-level. It aims to systematically describe rehabilitation services at the organizational level.
As discussed above, ICSO-R 2.0 has been further developed to revise the previous version to make it easier to understand, more user friendly and to better differentiate among the dimensions and categories. ICSO-R 2.0 can be used for several purposes. From health systems and scientific perspectives, it should be suitable for:
The ICSO-R 2.0 can also be used for many others purposes. Several further steps are required to develop the current version of ICSO-R 2.0 further, including:
1. developing value sets and measures;
2. developing examples of usage and training material; and
3. developing minimum reporting standards for service organizations in clinical trials.
The authors thank all of the experts who reviewed and made great comments for the development of ICSO-R 2.0: Martin Ahualli, Jerome Bickenbach, Andrew Cole, Julia Patrick Engkasan, Kurtis Hoppe, Jolanta Kujawa, John Melvin, Sasa Moslavac, Kuno Schedler, Melissa Selb and Gerold Stucki.


 Click to show fullsize
Click to show fullsize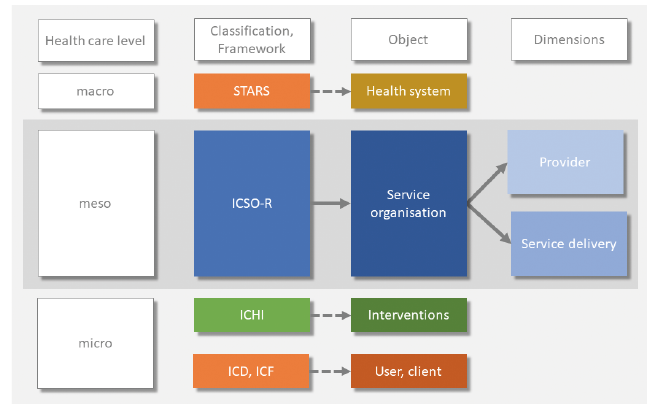 Click to show fullsize
Click to show fullsize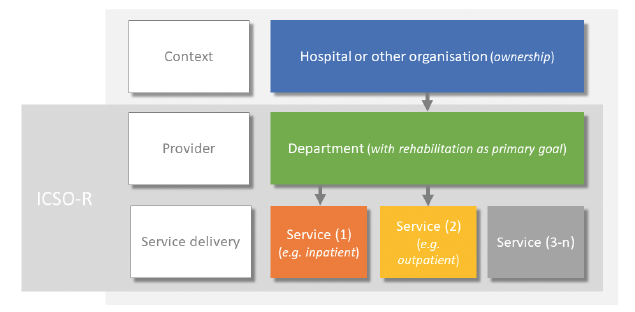 Click to show fullsize
Click to show fullsize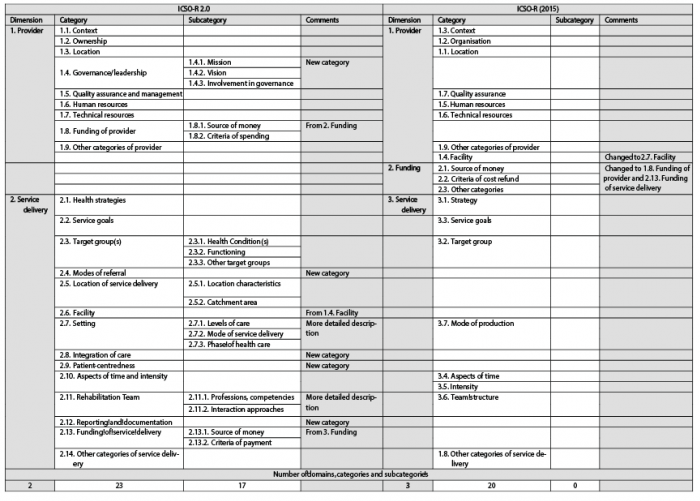 Click to show fullsize
Click to show fullsize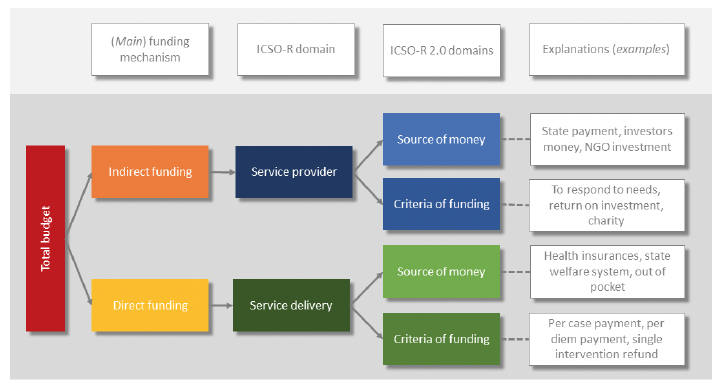 Click to show fullsize
Click to show fullsize