
From the 1Radboud University Medical Center, Donders Institute for Brain, Cognition and Behavior, Department of Rehabilitation, Nijmegen, The Netherlands, 2Charles Sturt University, School of Community Health, Albury, Australia, 3Radboud University Medical Center, Donders Institute for Brain, Cognition and Behavior, Department of Neurology, Nijmegen, The Netherlands, 4University of Sydney, Discipline of Occupational Therapy, Sydney, Australia and 5HAN University of Applied Sciences, Research Department of Neurorehabilitation, Nijmegen, The Netherlands
Objective: To explore the use of applied cognitive strategy behaviours during performance of daily activities in people with Parkinson’s disease.
Design: Quantitative cross-sectional design.
Methods: A total of 190 persons living at home with non-dementing Parkinson’s disease were videotaped while performing a self-chosen activity in their natural environment. The videotaped performance was scored using the “Perceive, Recall, Plan & Perform System of Task Analysis” to measure: (i) performance mastery; and (ii) effective use of 34 cognitive strategy behaviours covering: attention and sensory processing (Perceive), accessing task-related knowledge (Recall), response planning and evaluation (Plan) and performance control (Perform). Mean performance mastery and a hierarchy of least to most effective applied cognitive strategy behaviours were determined for the total group and for 2 sub-groups based on disease severity. A multi-faceted Rasch model was used for data analysis.
Results: Mean performance mastery was 56% (standard deviation 28%). Least efficient cognitive strategy behaviours were those used for planning, evaluating and controlling performance and most efficient strategies were those used for sensory discrimination and recalling factual information. More advanced disease indicated less efficient use of applied cognition.
Conclusion: The results suggest that the efficiency of applied cognitive strategy behaviours is compromised in a certain pattern in people with Parkinson’s disease, and that it declines with disease progression.
Key words: Parkinson’s disease; cognition; activities of daily living; observation; neurological rehabilitation; occupational therapy.
Accepted Dec 3, 2019: Epub ahead of print Dec 10, 2019
J Rehabil Med 2020; 52: jrm00010
Correspondence address: Ingrid Sturkenboom, Radboud University Medical Center, Department of Rehabilitation (931), PO Box 9101, 6500 HB Nijmegen, The Netherlands. E-mail: ingrid.sturkenboom@radboudumc.nl
When performing daily activities, people use internally generated cognitive strategies, or ways of thinking, to plan and execute appropriate actions. This is known as applied cognition. This article describes a study that sought to measure the efficiency of applied cognition of 190 persons with non-dementing Parkinson’s disease who were living at home. Participants were asked to perform a usual activity in their own homes. Their performance was videotaped and scored by assessors. The standardized observation instrument measured the effective use of 34 applied cognitive strategy behaviours. These behaviours represent 4 information-processing domains: attention and sensory processing (Perceive), accessing task-related knowledge (Recall), planning and evaluation (Plan), and performance control (Perform). The results indicated that applied cognitive strategies used to plan, evaluate and control performance were the least efficient. The most efficient were those used for sensory discrimination and recalling facts. The subgroup with the more advanced Parkinson’s disease had the least efficient use of applied cognition. The results may inform further development of suitable interventions to optimize activity performance.
Parkinson’s disease (PD) is the fastest growing degenerative neurological disorder. The number of persons with PD worldwide is expected to double by 2040, from 6.9 to 14.2 million (1). PD is a complex disease with a highly individualized pattern and progression of motor and non-motor symptoms. These symptoms have a significant impact on the ability of persons with PD to engage in meaningful daily activities. In particular, non-motor symptoms, such as cognitive impairments, have been found to be associated with reduced quality of life, higher caregiver burden and higher institutionalization (2).
When people perform daily activities, they use their cognitive capacity strategically (“applied cognition”) to process task-related sensory stimuli, recall task-related facts and procedures, and plan and monitor performance for the task at hand (3). For example, they use knowledge about the duration of the task to plan an appropriate pace of performance.
When cognition is used efficiently, the person is able to choose and apply the best strategy in the “here and now” to fit the particular task and context (3). The efficient use of applied cognition depends not only on existing cognitive capacity, but also on individual coping strategies and the characteristics of the task and contextual demands. In comparison with routine tasks, complex or novel tasks require increased use of higher order cognitive strategies.
People with PD have difficulty performing habitual daily tasks, requiring them to use higher level thinking strategies to carry out daily activities that were previously automatic (4, 5). At the same time, people with PD may experience cognitive deficits in executive functions, attention, processing speed, working memory and visuospatial functions (6). These cognitive deficits may compromise the availability, flexibility and speed, and thus the efficiency, of applied cognition during daily functioning.
Cognitive capacity, as measured by neuropsychological tests, may not sufficiently predict or explain actual performance in daily life (7). In order to evaluate the utility of cognition in daily life, it is important to obtain the experiences of people with PD in situ using performance-based measures (4). Research using performance-based measures indicates that cognitive impairment in PD impacts the ability to successfully perform complex activities (8). However, there are limited data about the particular cognitive strategies that pose the greatest barriers for activity performance, and how difficulties in applied cognition evolve during the course of the disease. Further insight into how cognition is used by people with PD may lead to the development of tailored interventions that target the thinking processes needed for task performance and, ultimately, the improvement or maintenance of daily functioning.
Therefore, the aim of this study was to explore the efficiency of applied cognitive strategies in people with non-dementing PD when they perform meaningful daily activities. Specifically, the study assessed the efficiency of applied cognition in the domains of sensory processing, recall, planning, and performance monitoring to ascertain: (i) those applied cognitive strategy behaviours that were observed as most to least efficient in people with PD; and (ii) the differences in efficiency of applied cognition between mild disease stage and moderate/severe disease stage.
This study employed a quantitative, cross-sectional design, using de-identified, secondary, baseline data from previous research, the Occupational Therapy in Parkinson’s disease study (OTiP study) (9, 10). The OTiP study had received ethical approval from the medical ethics committee of Arnhem-Nijmegen (NL27905.091.09/ABR27905) and participants had provided written consent before baseline assessment.
Participants
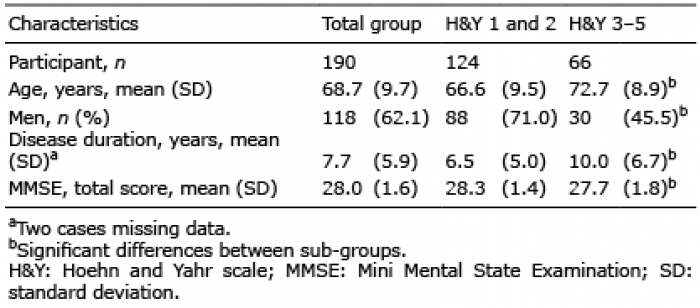
The study used baseline data of 190 of the 191 OTiP participants. One of the OTiP participants, for whom there was no baseline data for the measurement used in this secondary study, was excluded. Eligible participants for the OTiP study had been diagnosed with idiopathic PD by their own neurologists, lived at home and had reported difficulties in daily activities. People with a diagnosis of atypical parkinsonism, pre-dominant disabling co-morbidity or a Mini Mental State Examination score of less than 24 had been excluded. Disease severity was based on the commonly used Hoehn and Yahr Scale (H&Y) (11). This is a categorical scale, with stages 1 to 5 defined by advancing clinical motor features. Forty-six participants were in H&Y stage 1; 78 in stage 2; 59 in stage 3; 6 in stage 4; and 1 in stage 5. For the analysis, the participants were divided into 2 sub-groups of disease severity: mild stages of the disease (H&Y stages 1 and 2; n = 124) and moderate-to-severe stages of the disease (H&Y stages 3 to 5; n = 66). In Table I the demographics and baseline data relevant to this secondary study are presented for the total group and for the 2 sub-groups of disease severity.
The mild disease severity sub-group was significantly younger, had shorter disease duration and had a lower proportion of women compared to men than the sub-group of participants with moderate-to-severe disease.
Table I. Baseline characteristics
Measure
Efficiency of applied cognition was measured using the Perceive, Recall, Plan & Perform System of Task Analysis (PRPP assessment) (3). The PRPP assessment is a standardized, 2-stage, criterion-referenced and observation-based measure of the efficiency of applied cognitive strategies during activity performance.
Prior to the assessment, the client and therapist agree on a meaningful task to be observed and the performance criteria needed (the criterion). For example, for dressing, the criterion of person A may be that he/she has to do the whole task independently within 5 min; after the caregiver has helped the person to put on his/her trousers.
Stage one of the PRPP assessment involves a procedural task analysis in which the task is broken down into performance steps (e.g. switch on coffee machine) and subsequent rating to determine the total performance mastery. This is quantified in percentage of the steps of the activity that are performed error-free. The types of errors that can be rated per performance step are: accuracy error, repetition error, omission error and time error. The potential mastery range is 0–100%. A 100% mastery score reflects the performance of the task, as defined by the specific criterion (e.g. the criterion-referenced feature of the PRPP assessment).
Stage two assesses how effectively the person used each of 34 defined applied cognitive strategy behaviours (PRPP items) and identifies underlying cognitive reasons for reduced performance mastery identified in Stage one. The 34 items are divided into 4 information processing domains, termed quadrants. Each quadrant connects to a specific conceptual stage of information processing and includes strategies for: attention and sensory perception (Perceive quadrant); accessing task-related knowledge (Recall quadrant); response planning and evaluation (Plan quadrant); and performance initiating and monitoring (Perform quadrant). This is visualized in the central core of the PRPP conceptual processing model (Fig. 1).
The applied cognitive strategy behaviours associated with each quadrant and the underlying cognitive capacities, such as attention and memory form the PRPP items and are located on the outer ring of Fig. 1 (3). Each strategy behaviour, except “matches” is necessary to perform any goal-directed activity with 100% mastery. “Matches” refers to identifying 2 or more similar sensory images that are the same according to a specific sensory attribute required for the task, such as same colour, size, weight, shape, configuration, and sound. This strategy is needed only in tasks that demand this feature. For example, seeing if 2 pictures are the same when playing cards, or hearing that the sound you make is of the same pitch as the sound of other people when singing together in a choir.
Each PRPP item is rated on a 3-point scale, which indicates how effectively the person used the cognitive strategy behaviour to perform the task: effective use (score 3), questionable use or slow use (score 2); or ineffective use (score 1). “Matches” was scored as effectively used if it was not applicable in a task. All other items were always scored based on the observed efficiency of task performance.
Fig. 1. The Perceive, Recall, Plan and Perform (PRPP) System of Task Analysis Conceptual Model. Published with permission by Chapparo & Ranka (3).*greater than expected Outfit MnSq & z-score.
The PRPP assessment makes it possible to assess any goal-oriented functional task performance. The standardization lies in: (i) the specific definition of the PRPP item in observable behaviour; (ii) the observation procedure; and (iii) the assessment criteria for the actual task performance (3). To illustrate, Box 1 provides the definition of 1 PRPP item from each quadrant and an example of observed behaviour for that PRPP item.
The PRPP assessment can be administered by occupational therapists who have completed a 5-day postgraduate training on the instrument. The PRPP assessment has demonstrated acceptable reliability or validity when used with adults who have a similar neurocognitive disorder to PD, such as dementia (12) and traumatic brain injury (13, 14). In PD the reliability of the PRPP assessment is acceptable (15).
Data collection procedures
For the OTiP study, the Canadian Occupational Performance Measure (COPM) was administered at baseline in the participant’s home. The COPM is a semi-structured interview in which people identify, prioritize and score 3–5 problems they encounter in meaningful daily activities and participation.
Next, the participant was asked to select and perform 1 of the activity-based priorities mentioned in the COPM. The choice depended partly on what was feasible in the available context and time. The care partner could be involved in the discussion about what activity to perform, but this was not necessary. As a result, the type and duration of the participants’ activities were diverse. Examples include functional mobility (e.g. bed mobility, transfers, cycling, driving), showering and dressing, house cleaning or laundry, food or beverage preparation (hot or cold), using a computer or telephone, handwriting, gardening, small repairs and leisure (e.g. painting, making jewellery, playing an organ). After selecting the activity, the criterion was verified (e.g. what clothes to put on in the activity of dressing).
The participants performed the activity in the way they usually do, i.e. with no modifications to the task or material. The observation took place during their ON medication state (up to 2 h after medication intake). The activity performance was videotaped by the OTiP assessor. Each video was later observed and scored by a PRPP assessment-trained rater. For this study, raters had received an additional calibration session with attention on the criterion and Parkinson-specific behaviour related to items of Stage two. In total, there were 8 raters, each of whom rated between 7 and 62 participants. Raters had received information about the task performed, but had no information about the person, the task or the context other than what was visible on the video.
Data analysis
The mean (standard deviation; SD) total activity performance mastery was calculated using descriptive analysis. The raw data of stage 2 of the PRPP assessment were analysed using FACETS 3.71.4 (Rasch measurement software; Linacre, 2007) (16). Rasch models are a subclass of item response theory; are a relatively recent development in psychometric research, encompassing a group of methods and models for assessing model-data fit and thus evaluating reliability and validity of tests and questionnaires. Rasch measurement helps to construct instruments that carefully compute “measures” of human performance. Rasch modelling enables ordinal-level scales (e.g. rating scales, such as the PRPP assessment) to be converted to interval-level scales on a unidimensional continuum. These interval-scaled measures can then be used more accurately with parametric statistical tests (14, 17).
For this analysis, a 4-faceted Rasch model was generated with facets measuring patients, PRPP items, tasks performed and the raters. Measures for each facet are represented on a single common line from negative to positive infinity, which represents the underlying unidimensional construct of information processing. The Rasch calibrated hierarchy of 34 PRPP items was generated following the procedure outlined by Bond & Fox (17), and described the hierarchical ordering of PRPP items from least to most effectively used for people with PD. A more detailed description of PRPP Rasch analysis is provided by Nott & Chapparo (14).
Prior to generation of the item hierarchy, each PRPP item was first examined for “fit” with the Rasch mathematical model, considering both infit and outfit, as mean square values and standardized z-scores. For clinical observations, a mean-square range of 0.5–1.7 is considered acceptable, with normalized z-score (18). Infit and outfit statistics are also reported in normalized form (z), where their expected value is 0, and standardized z values greater than +2 or less than –2 are generally interpreted as having less compatibility with the model than expected (p < 0.05). Negative values indicate less variation than modelled, while positive values indicate more variation than modelled (17). The latter are generally considered more problematic during interpretation.
Mis-fitting items were analysed through reference to raw data, checking all unexpected observations. Category thresholds were examined for order. Nil re-ordering was required.
Interaction plots were formed to analyse differences in efficiency of cognitive strategy application between the 2 disease severity sub-groups. In addition, the FACETS software generated a Rasch-calibrated PRPP item Total Score, which was exported to IBM© SPSS© Statistics Version 20.0. An independent samples t-test was conducted to evaluate statistical differences in PRPP item Total score between participants in these 2 disease severity groups. Group differences were considered statistically significant when p < 0.05. Cohen’s d calculations were performed to determine the effect size.
The mean level of procedural performance mastery for the total group of participants was 56% (SD 28); for the sub-group with mild PD 62% (SD 27) and for the sub-group moderate-to-severe PD 46% (SD 27).
Unidimensionality was evaluated by examining “fit” of the 34 PRPP items to the Rasch mathematical model, and 33/34 items demonstrated acceptable fit. One item (“matches”) demonstrated unacceptable fit due to a very large outfit mean square value (9.00) indicating more variation than modelled. Three additional items (“monitors”; “analyses”; “uses objects”) demonstrated marginal misfit. All 4 items demonstrated large outfit values; whereas infit values lay within acceptable thresholds. Outfit values are more influenced by performance outliers on PRPP items (i.e. people performing unexpectedly well on a difficult assessment item). The remaining 30 PRPP items demonstrated acceptable fit, indicating congruence with the underlying Rasch model (Table II).
Table II. Item fit statistics and measures
Examination of the Rasch generated hierarchy of PRPP items suggests a specific ordering from least to most effectively used in task performance, as outlined in Fig. 2. Item separation index = 1.88 with reliability index = 0.78.
Fig. 2. Rasch-generated hierarchy of Perceive Recall Plan Perform (PRPP) items from most efficient (bottom of the scale) to least efficient (top of the scale). CTX: contextualizes; ID: identifies.
The PRPP items applied most effectively by the participants were those cognitive strategy behaviours used to recall facts about objects and their use (“categorizes”, “recognizes”), to use language (“labels”), and to distinguish sensory features of the task (“matches”, “discriminates”). PRPP items requiring a higher order metacognitive function were less efficient, especially anticipating and responding to constraints (“sequences”, “identifies obstacles”, “chooses”, “organizes”), and evaluating task performance (“questions”, “analyses”, “judges”). The least efficient were applied cognitive strategy behaviours for ongoing programming and controlling of motor responses during task performance (“coordinates”, “flows”, “times”, “calibrates”, “adjusts”).
The graph of Rasch calibrated mean scores generated for each of the 34 PRPP items for the sub-groups with mild PD (H&Y 1–2) and moderate-to-severe PD (H&Y 3–5) is shown in Fig. 3. Two patterns emerged. First, applied cognitive strategy behaviours that were least efficient were found within the Plan and Perform quadrants. Secondly, there was a stepwise reduction in efficiency of applied cognitive strategy behaviours which showed the same pattern for the 2 severity groups.
Fig. 3. Interaction plot showing the difference between average scores obtained on all Perceive Recall Plan Perform (PRPP) items for each of the 2 sub-groups of Hoehn and Yahr (H&Y) stages. Context: contextualizes; ID: identifies.
The graph of Rasch calibrated mean scores generated for each of the 34 PRPP items for the sub-groups with mild PD (H&Y 1–2) and moderate-to-severe PD (H&Y 3–5) is shown in Fig. 3. Two patterns emerged. First, applied cognitive strategy behaviours that were least efficient were found within the Plan and Perform quadrants. Secondly, there was a stepwise reduction in efficiency of applied cognitive strategy behaviours which showed the same pattern for the 2 severity groups. The independent samples t-test showed a statistically significant mean difference in PRPP item Total Score between the sub-groups. The group with mild PD had a higher score (i.e. more effective use of applied cognitive strategy behaviours) than the group with moderate-to-severe PD (Table III). This difference achieved a moderate level effect size (Cohen’s d = 0.44).
Table III. Results of t-test and descriptive statistics for the Rasch-generated Perceive Recall Plan Perform (PRPP) item total score by disease severity. Higher mean indicates better performance
The findings from this study indicate that participants with PD experienced a reduction in task performance, accompanied by an underlying hierarchy in efficiency of applied cognitive strategy behaviours during performance of everyday tasks. Overall, cognitive strategy behaviours in the Plan and Perform quadrants were least efficient. Examination of the 2 disease severity sub-groups indicated a stepwise decrease in efficiency of cognitive strategy use with progressing disease.
Of the 4 PRPP processing quadrants, a number of items within the Perceive quadrant were most efficient. While participants in both severity groups were able to orient to basic sensory task-related stimuli and sustain attention for the duration of task performance, they demonstrated difficulty in rapidly shifting and re-focusing attention within parts of the task when required (“modulates”). This finding is consistent with previous research, which has described abnormal attention shifting behaviour in PD (19). Unexpectedly, cognitive strategy behaviours for searching and finding objects and materials needed for the task were slightly less efficient for the group of participants in the mild disease severity stage than for the group with moderate-to-severe disease severity. The PRPP items in the Recall quadrant depend on task-related working memory, such as recognizing and grouping objects by as demanded by the task. These results are supported by research that indicates that declarative memory (6) and recall of tool attributes (20) remain intact in people with non-dementing PD. In contrast, the least efficient PRPP item in this quadrant was recalling how the body should be used to meet the requirements of a task or situation (“uses body”). This may partly be explained by reported deficits in proprioceptive integration in PD (21) or by difficulty in adequately compensating for, or adapting impaired habitual movement patterns.
Within the Plan quadrant, many applied cognitive strategy behaviours requiring executive or higher thinking processes were compromised (22). Specifically, results indicated difficulty with strategies used to plan complex task performance, solve problems during task performance, and monitor and evaluate ongoing performance. These results support prior research that suggests that people with PD report problems with executive functions in daily life (23, 24).
Most of the applied cognitive strategy behaviours that scored lower on effective use during task performance in this cohort are found in the Perform quadrant, particularly those strategies used to monitor and regulate body use and motor responses. Participants demonstrated difficulties in conducting the task in a smooth manner (“flows”), persisting with actions in a coordinated manner, making motor adjustments (“calibrates”, “coordinates”, “adjusts”) and altering performance speed to conform to task requirements (“times”). Reduced automatic internal responses to control, time and continue motor performance are well-known problems in PD and relate to dysfunction in the basal ganglia (5, 25). To enhance movement, it is suggested that people with PD can use compensatory strategies that bypass the basal ganglia and tap into higher level attention strategies, sensory cueing and planning strategies (5, 26, 27). The results of this study show that this cohort has either not (yet) succeeded in adequately compensating for these motor problems in daily activity performance, or that the suggested compensatory strategies are reliant on the very thinking strategies compromised.
The second important finding of this study indicated that applied cognition was significantly less efficient for participants in moderate-to-severe stages of disease (H&Y 3–5) than for participants in milder stages (H&Y 1–2). The results showed that most applied cognitive strategy behaviours that were affected in the moderate-to-severe disease stages were already, but to lesser extent, impacted in mild disease stages. The relationship of increasing cognitive difficulties and increasing disability with advancing H&Y disease stage is consistent with prior research (28).
A small number of PRPP items demonstrated misfit with the Rasch model. Limited performance variations were seen for the items “monitors”; “analyses”; and “uses objects”, because a few participants performed these strategies better than expected. The large misfit of the item “matches” is due to a systematic rating bias. Since a lot of activities scored did not require this item, most participants received a score of 3. Therefore, a lack of variation in the data for this specific item explains this misfit. In future research the scoring for “matches”, if not required in the task, should be handled as not applicable without a score. This has been addressed in the latest clinical standardization manual (15).
A novelty of this study is that it evaluated applied cognition very close to real-life performance. The activities were self-selected and meaningful for the patient and the execution of task performance took place in the natural context. The PRPP assessment used in this study not only evaluates performance mastery, but also explains which applied cognitive strategy behaviours contribute to the type of errors made in the performance. In clinical practice, this approach to assessment offers an ecologically valid adjunct to traditional modes of assessment of cognitive capacity. It does not, however, substitute the need for evaluating the subjective account of daily functioning issues from the perspective of patients and caregivers, and which may be different from any objective assessment outcome (4, 7).
Much of the available research on cognitive rehabilitation includes studies on remedial cognitive training. These studies show that, although the trained cognitive tasks improve in the short term, improvements do not necessarily generalize to daily task performance (29, 30). The few cognitive rehabilitation studies that suggest short-term beneficial effects on daily life include components of strategy or transfer training (31–34). The outcome of improvement in daily functioning in these studies was assessed with patient-reported outcome measures. It would be of value to add a performance-based outcome measure assessing everyday task performance to future studies on cognitive rehabilitation. Specific studies on cognitive strategy training for people with PD are scarce and, to the best of our knowledge, there are no guidelines about which cognitive strategy-based intervention might be most beneficial to people with PD and at what stages of cognitive decline. This current study identified profiles of applied cognitive strategy behaviours that were impacting on functional performance in one cohort of people with PD. In clinical practice, the PRPP assessment can be used at any stage of the disease to generate an individual profile of cognitive strategy difficulties and strengths, and to tailor interventions that suit the cognitive capacity of the person with PD and their performance goals. Furthermore, with knowledge about how the course of the disease is likely to impact thinking strategies that impact future occupational performance, people with PD may be able to engage in cognitive strategy interventions that prepare them to preserve their level of daily functioning for as long as possible.
Study limitations
This explorative study has some limitations. First, the assessment protocol stipulated that the observation should take place in the ON medication state. However, for people with PD who have to deal with ON/OFF fluctuations, it is often more problematic to carry out activities is during their OFF state. Although this study showed clinically relevant performance limitations in the ON state, the outcomes may have been worse if performance had been observed in the OFF state. The clinical guidelines therefore recommend that the therapist assess a person with PD who has fluctuations in both the ON and OFF states in order to obtain a comprehensive evaluation of daily activity performance (35). Another limitation was that the subgroup of people with moderate-to-severe PD included significantly more women and was significantly older. The difference in age can be explained because the progression of the disease takes years and older age of onset of disease is associated with greater severity of motor and non-motor symptoms (36). Research has shown that ageing affects processing speed, working memory and spatial abilities in cognitive tests (37). However, it is unlikely that the age difference between the 2 groups explains the differences in effective use of applied cognitive strategy behaviours in this study, as participants had self-selected a familiar daily activity and there was no extra time pressure.
The fact that the subgroup with more advanced disease contained relatively more women is notable and may form a bias to the results. While sex differences in performance of cognitive tests have been demonstrated in research (38), no research was available that revealed similar differences in applied cognition in daily activities between men and women. This would be interesting to address in future research.
A further limitation was that the study sample did not include people with a MMSE score below 24. Considering the higher prevalence and severity of cognitive deficits in more advanced disease stage, the results of the subgroup with advanced disease stage, in particular, cannot be generalized. In order to gain a better understanding of the strengths and difficulties of applied cognition in daily activities in people with PD throughout the disease continuum, future research should include a larger group with a more advanced disease including people with more severe cognitive impairment (i.e. PD dementia).
A final limitation linked to this, is that we did not gather detailed information about cognitive capacity of participants using alternate measures to the PRPP assessment. Although cognitive capacity as measured in neuropsychological tests is not always directly associated with performance in daily life, it might be valuable in future research to explore how the PRPP items relate to cognitive deficits in PD as determined by other measures.
Conclusion
The results of this study suggest that the efficiency of applied cognitive strategy behaviours is compromised in people with non-dementing PD. In particular, applied cognition for planning and monitoring performance was less efficient than many sensory and recall operations. In addition, the results indicate that the effective use of applied cognitive strategy behaviours declines with disease progression. The results of this study can form a basis for the development of tailored interventions that target those applied cognitive strategy behaviours needed to successfully complete meaningful daily activities.
The authors thank the OTiP participants and the PRPP raters for their participation in the OTiP study.
The data collection (in the original OTiP study) was financially supported by Prinses Beatrix Spierfonds and Parkinson Vereniging (grant number WR0-029). No additional external funds were received for the design, analysis and authorship of this secondary study.
Conflicts of interest. Dr Chapparo is one of the developers of the PRPP System of Task analysis. Dr Chapparo and Dr Steultjens provide postgraduate training courses for occupational therapists on standardized use of the PRPP assessment in clinical practice. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize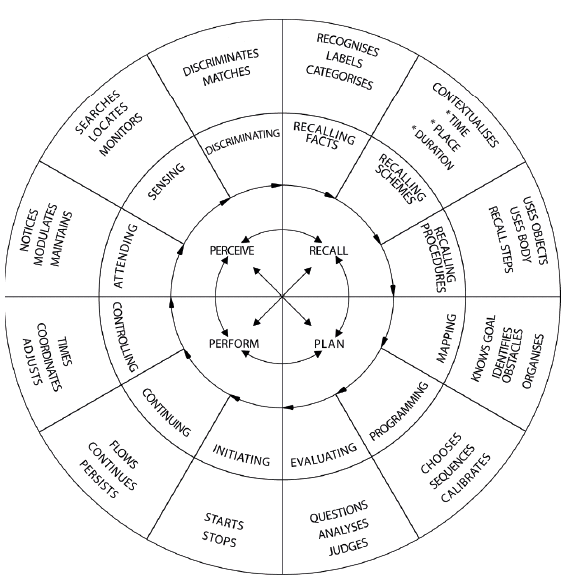 Click to show fullsize
Click to show fullsize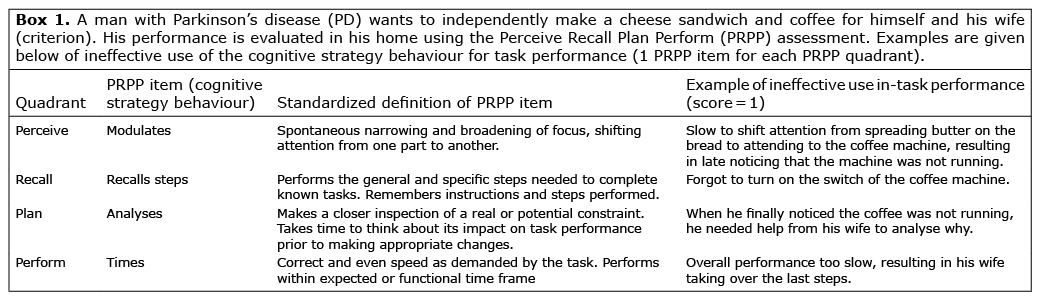 Click to show fullsize
Click to show fullsize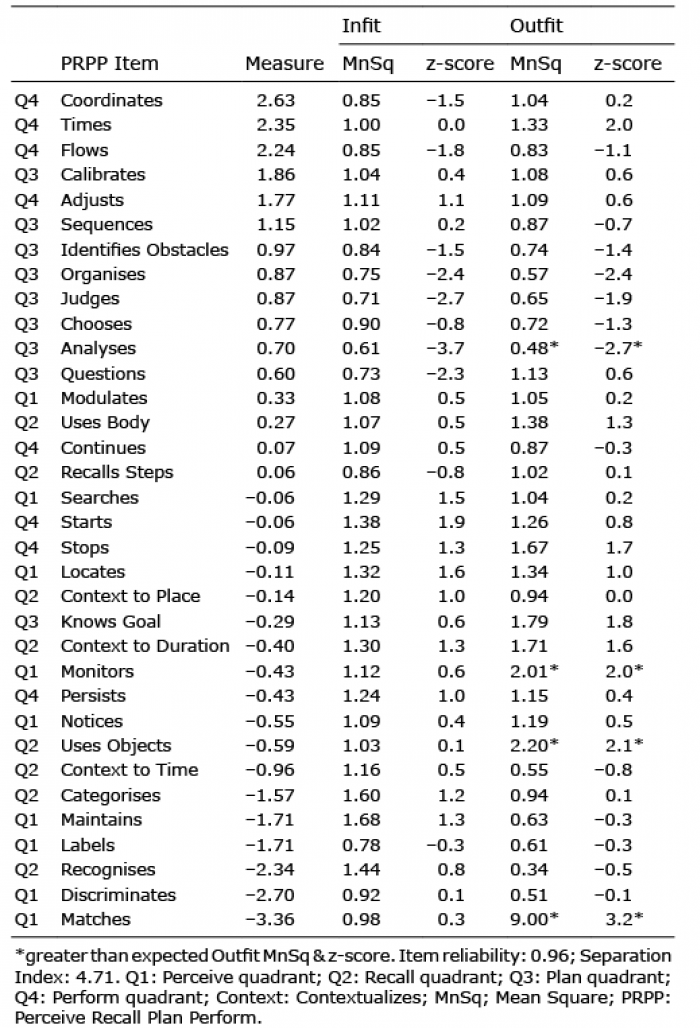 Click to show fullsize
Click to show fullsize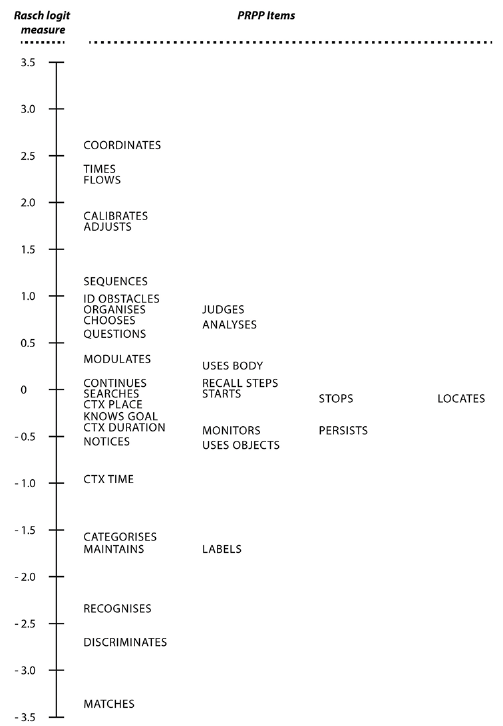 Click to show fullsize
Click to show fullsize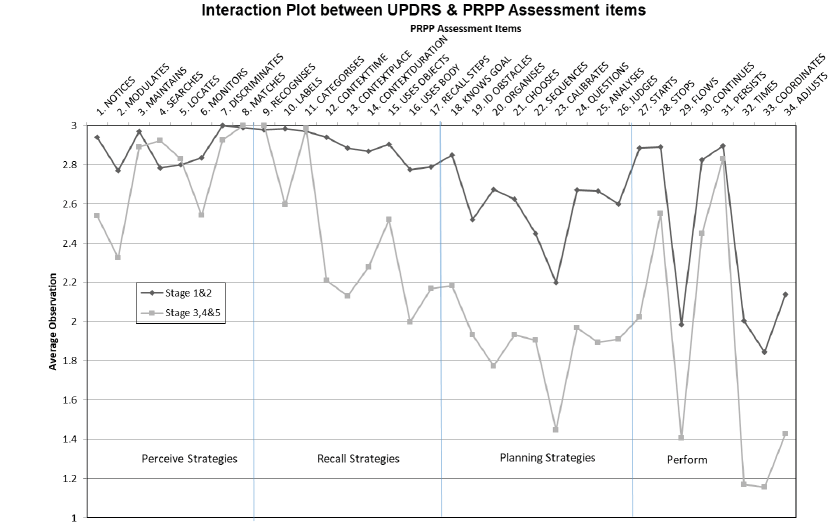 Click to show fullsize
Click to show fullsize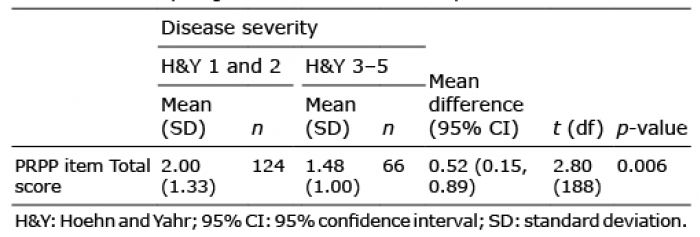 Click to show fullsize
Click to show fullsize