
From the 1Department of Physical Medicine and Rehabilitation, Haeundae Paik Hospital, University of Inje College of Medicine, Busan, Korea, 2Department of Physical Medicine and Rehabilitation, Lille University Medical Centre, Lille, France, 3Department of Rehabilitation Medicine, Royal Melbourne Hospital, 4Department of Medicine (Royal Melbourne Hospital), University of Melbourne, 5Australian Rehabilitation Research Centre, Royal Melbourne Hospital, Parkville and 6School of Public Health and Preventive Medicine, Monash University, Victoria, Australia. *These authors contributed equally to this publication
Objective: To evaluate evidence from published systematic reviews of clinical trials to determine the effectiveness of repetitive transcranial magnetic stimulation (rTMS) in stroke population.
Methods: The Cochrane Library, MEDLINE, CINAHL, EMBASE, and PubMed were searched for systematic reviews up to 15 January 2019. Three authors independently screened the reviews and assessed the methodological quality, using Assessment of Multiple Systematic Reviews (AMSTAR) appraisal tool. Quality of evidence for outcomes evaluated within the reviews was appraised with Grade of Recommendation, Assessment, Development and Evaluation (GRADE) tool.
Results: Twelve reviews (n = 9,117 participants) evaluated the effectiveness of rTMS on motor and non-motor (aphasia, depression, dysphagia and cognition) functions. The rTMS protocols applied and outcomes measured were diverse amongst the selected reviews. The findings suggest beneficial effect of rTMS with: “moderate quality” evidence for dysphagia and hemineglect, “low to moderate quality” evidence for motor function (upper limb function, daily activities), and “low quality” evidence for aphasia and post-stroke depression.
Conclusion: Despite widespread use of rTMS, high-quality evidence for its routine use for the treatment of stroke survivors is lacking. Further studies are required to establish differential roles of various protocols and long-term effects of rTMS in the stroke population.
Key words: stroke; transcranial magnetic stimulation; rehabilitation; systematic review.
Accepted Dec 6, 2019; Epub ahead of print Dec 18, 2019
J Rehabil Med 2020; 52: jrm00015
Correspondence address: Bhasker Amatya, Department of Rehabilitation Medicine, Royal Melbourne Hospital, 34–54 Poplar Road, Parkville, Victoria, Australia. E-mail: bhasker.amatya@mh.org.au
Stroke causes significant disability and morbidity. Currently, a range of rehabilitation interventions to manipulate or induce brain plasticity, including repetitive trans-cranial magnetic stimulation (rTMS) are used for stroke care. There is a growing body of research in this area, with several systematic reviews evaluating efficacy and safety of rTMS for various clinical outcomes. This review systematically evaluates evidence from published systematic reviews of clinical trials to determine the effectiveness of rTMS in people with stroke to guide treating clinicians. The included reviews used varied rTMS protocols and outcome measures. The findings suggest limited high-quality evidence for improved motor and non-motor functions following stroke; hence, routine clinical use of rTMS is yet to be established.
Stroke is a leading cause of long-term neurological disability in adults worldwide, with an estimated 15 million strokes reported annually (1, 2). It frequently causes impairments resulting in long-term debilitating effects (3). Current advances in the medical management of stroke have improved survival rates significantly, and highlight the need for optimal, comprehensive acute and longer-term management of motor and non-motor impairments, which contribute to disability.
Despite spontaneous motor recovery after stroke, at 3 months approximately 70% of stroke survivors continue to have restrictions in functional tasks and activities of daily living (ADLs) due to motor/sensory deficits, incoordination and spasticity (4, 5). During recovery after stroke, abnormal neuronal activity causes disruption in regular interhemispheric communication (6, 7), commonly in the motor system (8). Cognitive impairments (such as post-stroke depression; PSD) are common (reported in almost 30% of patients) (9). Significantly higher rates of PSD and anxiety are reported in chronic stages of stroke recovery, compared with the general population (10). Further, hemispatial neglect (range 13–82%) (11) leads to poor functional motor recovery (12), increased falls risk and caregiver burden (13). Swallowing problems (50–80%) (14), increased length of hospital stay, additional health service utilization, complications and worse outcomes (15). Furthermore, mortality rate significantly increases by 2.6-fold in patients with post-stroke dysphagia compared with their counterparts without dysphagia (16). These impairments contribute to longer-term morbidity and mortality, restrictions in ADLs, and decreased quality of life (QoL) (17).
Currently, a range of rehabilitation interventions are trialled in the management of stroke. Many alternative and adjunct therapeutic techniques to manipulate or induce brain plasticity, including repetitive trans-cranial magnetic stimulation (rTMS), are used to enhance conventional rehabilitation therapies (18). rTMS is a non-invasive neuro-modulatory therapeutic intervention used to promote/enhance efficacy of rehabilitation after stroke (19) by restoring the disrupted equilibrium and inter-hemispheric communication to rebalance interhemispheric competition (20). It delivers electrical current to modulate cortical neuronal excitability (5) at the stimulation site (21). Delivering a series of magnetic stimuli to targeted brain areas induces inhibitory effects on motor cortical excitability with low-frequency (LF) (≤ 1 Hz) or promotes cortical excitability with high-frequency (HF) (≥ 3 Hz). After stroke, it is postulated that suppression of the undamaged contra-lesional motor cortex by rTMS or increasing the excitability of the damaged hemisphere cortex promotes functional recovery (22). Due to these unique features, the use of rTMS has increased rapidly as a potential rehabilitation tool for stroke patients to enhance functional and psychological recovery (23). However, evidence supporting its routine use for post-stroke impairments is limited (18, 24).
Various systematic reviews have evaluated the effectiveness and safety of rTMS for various functional and psychological outcomes in persons following stroke (9, 18, 21, 25–27). However, published reviews vary in scope, methodology and quality, with different and, at times, diverse findings and conclusions about the effectiveness of rTMS. Further, some review findings overlap with each other. Therapeutic values, including benefit and harm, associated with rTMS, including efficacious approaches, timing, and intensity need to be established. An overview of systematic reviews is a new approach to synthesize high-quality evidence across the same or very similar interventions, to summarize treatment effect in a much broader concept (28). The aim of this review, therefore, is to systematically evaluate evidence from published systematic reviews of clinical trials to determine the effectiveness of rTMS in people with stroke, in order to guide treating clinicians.
The Cochrane Library database (including Database of Abstracts and Reviews of Effectiveness), MEDLINE, CINAHL, EMBASE, and PubMed were comprehensively searched for systematic reviews evaluating the efficacy of rTMS interventions for various post-stroke impairments until 15 January 2019. The combination of multiple searches for 2 themes of stroke and transcranial magnetic stimulation (non-invasive stimulation) was used for the search strategy. The keywords used to search for studies are listed in Appendix SI1.
A comprehensive multi-pronged methodology was employed. All systematic reviews, meta-analyses registered in these databases that reported a systematic electronic search of literature for a defined period, were included. Bibliographies of pertinent articles and relevant journals were manually searched for additional references. Authors and known experts in this area were contacted as required. Grey literature search was performed using various internet search engines and websites including: System for Information on Grey Literature in Europe, New York Academy of Medicine Grey Literature Collection, National Quality Measures Clearinghouse, and Google Scholar. Systematic reviews on rTMS involving other medical conditions, where data were specifically provided for stroke, were also included. Furthermore, reviews comparing other non-invasive stimulation, such as transcranial direct current stimulation (tDCS), with rTMS, where separate subgroup analysis on the rTMS was included. The exclusion criteria included: reviews conducted in paediatric population (< 18 years old); those evaluating the efficacy of interventional rTMS combined with other measures of rehabilitation, pharmacological, surgical intervention; reviews using TMS to assess functional aspects and structure of the brain; non-interventional TMS protocols; non-English reviews; narrative reviews; theses; and reviews listed only in conference proceedings.
Study selection and data extraction
Three authors (WK, CR, PH) independently screened all potential abstracts and titles of reviews for inclusion and appropriateness, based on the selection criteria. Each study was evaluated independently, and the full-text article was obtained for assessment to determine whether the review met the inclusion/exclusion criteria. Any disagreement regarding the possible inclusion/exclusion of any individual review was resolved by discussion with other reviewers (BA, FK) and by a final group consensus. Data extraction was conducted by 3 authors (WK, CR, PH) independently, using a standard pro forma. The information obtained from all reviews included: publication and search date, objectives, characteristics of included studies and study subjects, intervention procedures (intensity, duration, etc.) and comparators, findings/patient outcomes in the review, and limitations. Any discrepancies were resolved by final group consensus re-evaluating the review.
Assessment of the methodological quality of included studies
Three reviewers (WK, CR, PH) independently assessed the methodological quality of each included review, using the Assessment of Multiple Systematic Reviews (AMSTAR) appraisal tool (Appendix SII1) (29). This critical appraisal tool, with 11 assessment items, has acceptable inter-rater agreement, construct validity and feasibility (29, 30). The Grade of Recommendation, Assessment, Development and Evaluation (GRADE) tool was used to assess quality of evidence for each outcome evaluated within the included reviews on a 4-point scale (high, moderate, low and very low quality) (31). First, an a priori ranking of “high” for randomized controlled trials (RCTs), and “low” for non-randomized controlled trials was assigned. Then, initial grading was either downgraded because of the risk of bias, the inconsistency, the indirectness of evidence or the imprecision of the publication bias; or upgraded the initial grading because of a large effect size and consistency in the findings. Finally, the grade was assigned “very low” if assessment was that the true effect was likely to be substantially different from the estimated effect. Any discrepancies were resolved by a final consensus amongst all reviewers.
Study selection
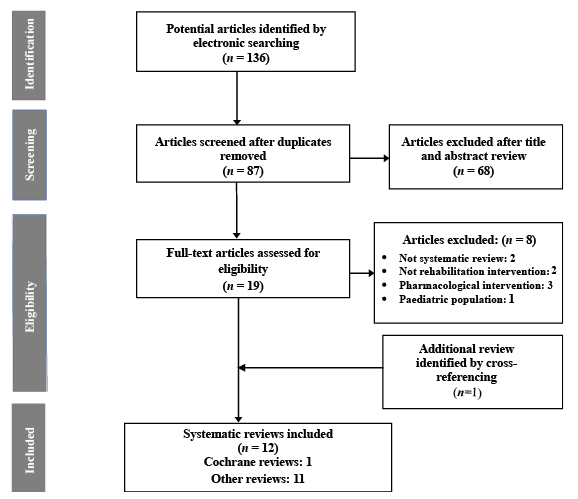
The electronic search strategy identified a total of 136 systematic reviews evaluating brain stimulation interventions in persons with stroke. After removing duplicates, 87 reviews met the abstract inclusion criteria. The main reasons for exclusion of reviews included: non-systematic reviews, valuation of other non-invasive brain stimulation (such as tDCS), and no specific sub-group data of patients with stroke. Full texts of these articles were retrieved, and all reviewers performed the final selection. Further, one review was identified from a manual search of bibliographies of relevant articles. Overall, 12 systematic reviews with a total of 9,117 subjects evaluating the effect of rTMS on motor and non-motor functions after stroke were included. Fig. 1 shows the flow diagram of the reviews selection process (Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PRISMA).
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram showing the selection of reviews.
Description of included systematic reviews
There was marked heterogeneity amongst the included reviews in terms of: included primary studies, stroke patient groups, rTMS protocols and the outcomes measured. The characteristics of included systematic reviews are reported in Table I.
Table I. Characteristics of included systematic reviews
Table I. cont.
Participants. Twelve systematic reviews with 9,117 adult participants with post-stroke impairments following ischaemic and/or haemorrhagic strokes in acute and chronic post-stroke phase were included. Six systematic reviews (n = 6,317 participants) (18, 21, 23, 24, 27, 32) evaluated the effectiveness of rTMS on motor and functional outcomes; 3 reviews evaluated (n = 1,916) (9, 24, 26) post-stroke depression outcomes, and 2 reviews each evaluated aphasia (n = 157) (24, 33), cognitive impairment (n = 301) (24, 34) and dysphagia (n = 255) (25, 35).
Primary study design. Most primary studies included were RCTs (192 of 235 studies), conducted between January 1980 and December 2016. There was marked variability amongst the studies with regard to the rTMS protocols used. Nine of the 12 included systematic reviews (21, 24–27, 32–35) performed meta-analyses, and the other 3 provided only qualitative description of findings due to heterogeneous data (9, 18, 23). Hao et al. (24) conducted 4 sub-group meta-analyses: on ADLs (2 RCTs, n = 183), motor function (4 RCTs, n = 73), post-stroke depression (2 RCTs, n = 92) and cognition (2 RCTs, n = 75). Similarly, Zhang et al. (27) performed 6 sub-group meta-analyses on: effect duration (38 RCTs, n = 979), stroke duration (16 RCTs, n = 399), rTMS frequency (31 RCTs, n = 866), theta burst stimulation (TBS) mode (9 RCTs, n = 125), lesion location (27 RCTs, n = 750) and number of sessions (25 RCTs, n = not provided).
rTMS protocols in the included studies. The rTMS protocol applied to motor cortex varied amongst the studies: with excitatory stimulation performed on the affected hemisphere (with lesion) to increase the efficacy of remaining cells (facilitation), inhibitory stimulation on the unaffected hemisphere (inhibition) to decrease the inhibitory connections from the non-lesioned hemisphere to the lesioned one, or both stimulations combined on both hemispheres (bilateral) (36). Frequency of stimulations used by the studies ranged from 0.5 to 50 Hz at 60–130% resting motor threshold (RMT). Stimulating pulses also varied from 40 to 10,000. The total number of rTMS session ranged from 1 to 28, with duration ranging from 10 to 20 min. The control interventions varied, comparing sham rTMS alone or with some additional therapies (e.g. physiotherapy, occupational therapy, acupuncture, medications, etc.).
Outcomes evaluated. The outcomes evaluated across the included reviews focused on 5 main domains: motor, aphasia, depression, dysphagia and cognition. The outcome measures to objectively determine the possible effect of rTMS on both functional and non-functional outcomes differed amongst studies, including motor function (muscle strength/force, symptom management (spasticity, pain, etc.), ADLs; psychological outcomes, etc. The majority of primary studies within the included reviews evaluated clinical and functional motor outcomes, mainly upper limb function. Other primary outcomes assessed were mixed and depended on the impairment domain evaluated. (Table I). The study assessment points also varied: the majority tested the possible effect of rTMS during the intervention and immediately post-intervention; and few assessed the longer term impact.
Quality assessment of the included reviews
Two reviewers (CR, PH) rated the quality of each included review using the AMSTAR tool. The kappa level of agreement between both authors for AMSTAR assessment was 0.91. The overall mean AMSTAR methodological quality score for included systematic reviews was 7.3 and ranged from 2 to 10 out of 11. Two reviews were rated as “low-” quality (AMSTAR scores = 0–4), 5 were rated “moderate-” quality (AMSTAR score s = 5–8), and 5 “high-” quality (AMSTAR scores = 9–11) (Table II).
All reviews, except 1 (25), had published an a priori protocol. All reviews, except 2 (18, 23), performed a comprehensive literature search of medical science databases. Two reviews (9, 22) did not include a grey literature search. All reviews, except 2 (18, 23), assessed the scientific quality of the primary studies using validated tools: 4 used PEDro, 3 used the Cochrane risk of bias tool, 1 review each used GRADE, Downs and Black tool, and the Revised CONSORT Statement. Only 2 reviews (24, 33) explicitly listed the excluded studies. None of the reviews stated the sources of funding for each of the included primary studies (Table II).
Table II. Quality assessment of included reviews
Effects of intervention
As mentioned above, the scope and measured outcomes amongst the included reviews varied. Overall quality of evidence for the use of rTMS was assessed using the GRADE assessment tool (Table III) and summary of impact of the rTMS on specific outcome domain categories are shown in Table IV. The existing best-evidence synthesis for rTMS for the management of post-stroke impairments based on outcomes is summarized below and in Table I.
Table III. GRADE* assessment of included studies
Table IV. Summary of impact of outcomes based on different impairments
Motor function
Six reviews (n = 138 RCTs, 38 non-RCTs; 6,317 participants) evaluated various motor outcomes (18, 21, 23, 24, 27, 32). The overall findings suggest that there is “low-” to “moderate-” quality evidence for the beneficial effect of rTMS on any motor function evaluated. Graef et al. (21) investigated rTMS (inhibition over the unaffected hemisphere (UH) and facilitation over the affected hemisphere (AH)) combined with upper-limb training. The authors did not find any positive effect on upper limb function and/or spasticity (standard mean difference (SMD) = 0.03, 95% confidence interval (95% CI) = –0.25 to 0.32, p = 0.82). Ludemann-Podubecka et al. (23) reported limited positive effect on affected hand motor recovery after inhibitory rTMS over the UH and bilateral rTMS, but were unable to recommend its routine use. Kang et al. (32) found that rTMS alone, or in combination with motor training, facilitated force production capabilities (effect size (ES) = 0.66, 95% CI = 0.45–0.86, p < 0.0001). Dionisio et al. (18) also reported significant improvements in functional and clinical capabilities after rTMS (inhibition over the UH and facilitation over the AH). Similarly, Zhang et al. (27) found significant improvements in upper limb function after rTMS, both for short-term effect (SMD = 0.43, 95% CI = 0.30–0.56, p < 0.001) and long-term effect (SMD = 0.49, 95% CI = –0.29 to 0.68, p < 0.001). In contrast, Hao et al. (24) did not find any significant improvement in functional scores after rTMS (inhibition over the UH and facilitation over the AH) on functional outcomes (Barthel Index (BI), SMD = 15.92, 95% CI = –2.11 to 3.95, p = 0.084) or on other motor function (SMD = 0.51, 95% CI = –0.99 to 2.01, p = 0.51).
Aphasia. Two reviews (n = 5 RCTs, 4 non-RCTs; 157 participants) evaluated the efficacy of rTMS on various aphasia outcomes (24, 33). The overall findings suggest some beneficial effect of rTMS on patients with post-stroke aphasia. Hao et al. (24) (n = 1 RCT, 14 participants) reported a significant improvement on the Aachen Aphasia Test total score (SMD = 19.8, p = 0.002) after inhibitory rTMS over the UH. Similarly, Shah-Basak et al. (33) in another review found overall improvement in language assessment (SMD = 0.448, 95% CI = 0.23 to 0.66, p < 0.001) after rTMS applied over non-lesion hemisphere or bilateral.
Post-stroke depression. Three reviews (n = 26 RCTs, one non-RCTs; 1,916 participants) evaluated the effectiveness of rTMS on depression outcomes, using the Hamilton Depression Rating Scale (HDRS) (9, 24, 26). Overall findings indicate, “low-” quality evidence for beneficial effect of rTMS on post-stroke depression outcomes. McIntyre et al. (9) (n = 1 RCT, 40 participants) found limited benefit on depression in the short-term after rTMS (inhibition over the UH and facilitation over the AH); whereas Hao et al. (24) (n = 2 RCTs, 92 participants) did not find any decrease in the HDRS score (bilateral low frequency rTMS) (SMD = –0.12, 95% CI = –13.84 to 13.59, p = 0.99). Shen et al. (26) found improvement in the PSD ((HDRS, mean difference (MD) = –6.09, p < 0.001)); response rates ((odd ratio (OR) = 3.46, p < 0.001)); remission rates (OR 0.99, p < 0.001); National Institutes of Health Stroke Scale, MD = –2.74, p < 0.001).
Dysphagia. Two reviews (25, 35) (n = 10 RCTs, 255 participants) evaluated efficacy of rTMS on various dysphagia outcomes in persons following stroke. The overall findings suggest that there is “moderate-” quality evidence for the beneficial effect of rTMS on patients with post-stroke dysphagia. Liao et al. (25) reported a positive effect of rTMS (over the UH and bilateral) on post-stroke dysphagia symptoms (SMD = 1.24, 95% CI = 0.67–1.81, p < 0.0001). Similar findings of a beneficial effect of rTMS on dysphagia outcomes in the shorter term were reported in another review (SMD 0.56, 95% CI = 0.04–1.09, p = 0.03) (35).
Cognition. Two reviews (n = 12 RCTs, 301 participants) evaluated the effects of rTMS on cognitive outcomes in person with stroke (24, 34). The overall findings indicate a “moderate-” quality evidence for beneficial effect of rTMS on cognitive function (such as hemispatial neglect, mental state, etc.). Salazar et al. (34) found positive effects of rTMS combined with other cognitive rehabilitation interventions in the line bisection test and the modified BI (SMD = –2.16, 95% CI = –3.00 to –1.33, p < 0.0001). Hao et al. (24) (n = 2 RCTs, 75 participants) showed that low-frequency rTMS did not have any significant effect on MMSE scores (SMD = 1.87, 95% CI = –5.93 to 9.68, p = 0.64).
This review systematically analysed evidence from published systematic reviews to date, for the effectiveness of rTMS on motor and non-motor functions in persons following stroke. The findings indicate that, although rTMS is widely trialled in this population, there is still lack of high-quality evidence for its routine use in clinical practice. The overall findings of this review of the use of rTMS in persons with stroke suggest:
“Moderate-” quality of evidence for improved post-stroke dysphagia and to reduce hemineglect.
“Low-” to “moderate-” quality of evidence for enhanced motor function (upper limb function, ADLs).
“Low-” quality of evidence for reduction in post-stroke depression and aphasia.
There was heterogeneity amongst the included reviews, even in those evaluating similar outcomes. The methodological quality of the included systematic reviews varied, with only 5 out of 12 rated as of “high” methodological quality (AMSTAR score) (30). Likewise, evidence for the use of rTMS targeting different stroke-related outcomes in the included reviews was diverse. This is mainly due to variation in operational procedures of rTMS (duration, intensity, etc.), outcome measurement tools, control intervention protocols and length of follow-up. Therefore, pooling data for quantitative analyses was not possible, and a best-evidence synthesis was described using qualitative analyses. For some outcomes evaluated, there were few primary studies within the included reviews, most with significant methodological limitations. Overall evidence for some of the studies was downgraded from actual evidence reported by authors, due to imprecision and inconsistency of findings, use of different outcome measures and inclusion of non-RCTs with poor methodology quality, precluding meta-analysis.
To our knowledge, this is first review to systematically appraise published systematic reviews to evaluate the effectiveness of rTMS for various stroke-related impairments in motor and non-motor domains. This approach of synthesizing findings of systematic reviews enables the comparison of results from multiple reviews, thereby providing a comprehensive evidence-based summary on evident outcomes. Recently, Leon Ruiz et al. published a narrative review of current evidence of rTMS in stroke neurorehabilitation, based on clinical practice guidelines and published recommendations (37). In comparison to our findings, the authors of this review reported beneficial effect of rTMS in treating stroke complications, including motor disorders, aphasia, dysarthria, oropharyngeal dysphagia, depression, and perceptual-cognitive deficits. However, consistent with our findings, these authors suggested further well-designed clinical trials with larger sample size with a higher level of evidence for proper implementation of rTMS use in stroke (37). Other published clinical practice guidelines on rTMS do not report recommendations specific to post-stroke population (38, 39).
The mechanisms underlying the effects of rTMS applied over the motor cortex are described in the literature (40). Non-invasive brain stimulation, such as rTMS over the motor cortex, induces changes, not only in the target motor area, but also in many cortico-subcortical and spinal structures, resulting in excessive interhemispheric inhibition from the non-lesional hemisphere after stroke (38, 39). This has led to exploration of possible therapeutic effects of rTMS with diverse protocols (facilitation, inhibition or combined), reflecting the range and number of studies identified in this review. Despite established guidelines (38, 39), standardized protocols are yet to be employed, with individual studies using varying range of protocols (rTMS frequency stimulations range 0.5–50 Hz, stimulating pulses 40–10,000, rTMS sessions 1–28, with duration ranging from 10 to 20 min) and characteristics of stimulation protocol (number of sessions, duration, intensity). Further, the outcome measures used and assessment time-points also differed. The measures used were specific to upper-limb function and ADLs. Objective methods, such as functional magnetic resonance imaging (MRI), neurophysiology, etc. were rarely used, despite their higher accuracy than clinical measures regarding subtle changes. The characteristics of participants were heterogeneous amongst the studies regarding the characteristics of stroke (type, lesion location and area, time since stroke, other comorbidities, age, etc.), which may have resulted in variability in findings. Further research is required into the confounding effects of adjunct therapies, including routine rehabilitation program, coupled with rTMS intervention.
Study limitations
Some limitations in methodology and the completeness of retrieved literature must be considered. Despite the comprehensive search employed, this review encompassed published literature written in English in specific health science databases, and only the bibliography of relevant articles was scrutinized. This may have introduced a selection and reference bias. However, extensive comprehensive searching, using broad search terms in most prominent databases, was used, and experts and prominent stroke-related organizations’ websites and the websites of experts and of prominent stroke-related organizations were explored to identify relevant studies. Widely used validated tools to assess methodology (AMSTAR) and quality of evidence (GRADE) of included studies were used. The accuracy of assessor’s assessments cannot be guaranteed; however, the selection of studies and quality assessments were independently performed by 3 authors, and further group consensus was achieved. Despite significant heterogeneity among the included reviews, with high variability in rTMS protocols and number of participants, we were able to categorize the effect of intervention on only 5 domains (motor function, aphasia, dysphagia, depression, cognition). These issues limit the generalizability of our findings. It was not possible to evaluate safety related to rTMS, as report of adverse events in the included reviews was incomplete or missing. The associated costs and/or economic benefit of rTMS were not reported in any review. Many included reviews had search dates upto 3 years prior to our systematic review, so we may have missed some recent studies which were not included in these review. Hence, the findings of this review should be interpreted with caution.
Conclusion
The management of persons following stroke is complex and challenging. Non-invasive brain stimulation techniques, including rTMS, are widely used, despite a lack of high-quality evidence for improved motor and non-motor functions in stroke survivors. Some positive effect of rTMS were noted for outcomes (dysphagia, hemineglect, aphasia and depression), but its routine use cannot yet be recommended. Further studies in larger cohorts with robust methodology are required for differential roles of various rTMS protocols and longer-term after-effects of rTMS in stroke. Future studies should take into account patient characteristics, rTMS stimulation parameters, stroke type and duration since stroke, due to the significance of the critical period after stroke for neuropathic recovery.
This review was supported from internal resources of the Rehabilitation Department, Royal Melbourne Hospital, Royal Park Campus, Melbourne, Australia.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize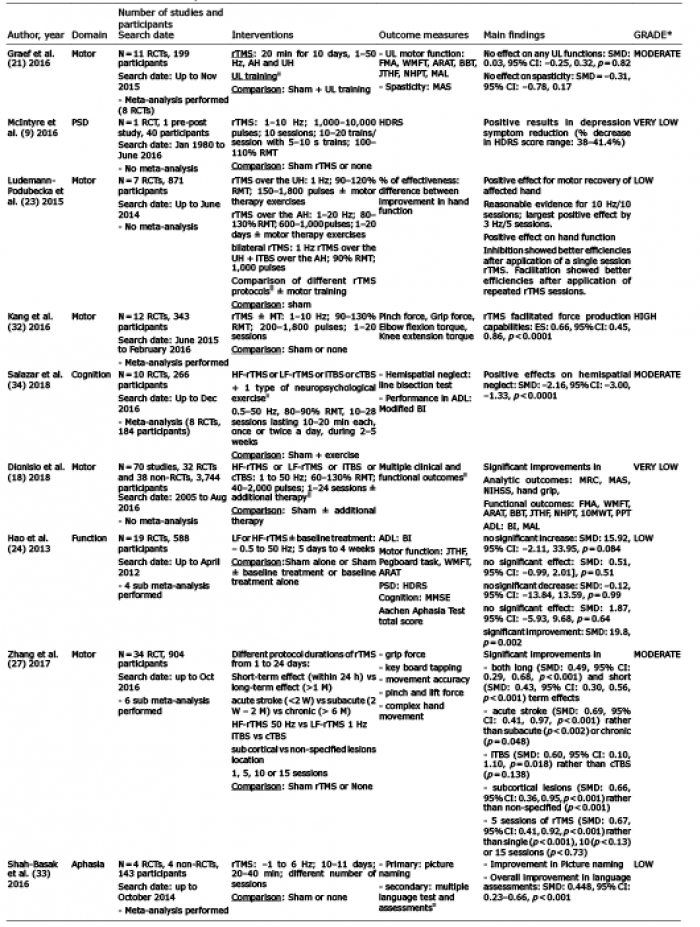 Click to show fullsize
Click to show fullsize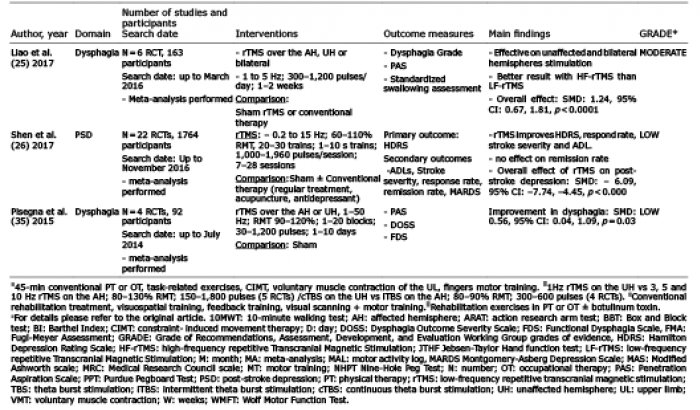 Click to show fullsize
Click to show fullsize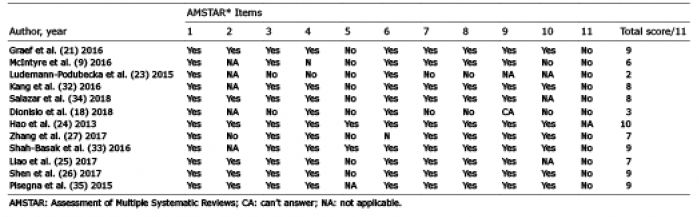 Click to show fullsize
Click to show fullsize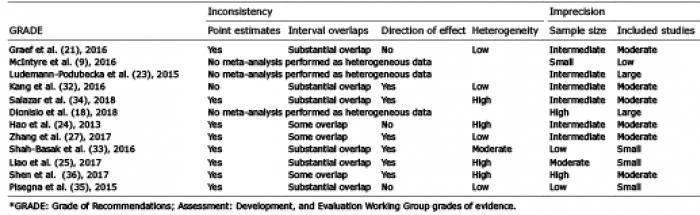 Click to show fullsize
Click to show fullsize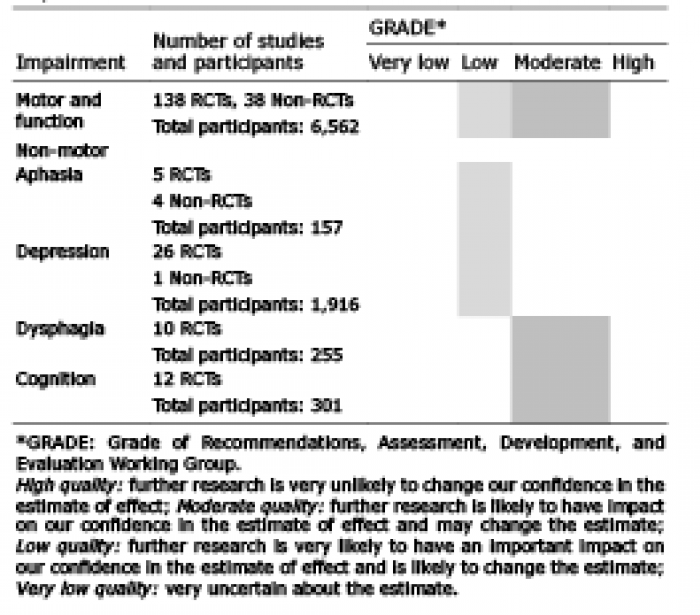 Click to show fullsize
Click to show fullsize