
From the 1Pan Am Clinic, Winnipeg, MB, Canada, 2Heartlands Hospital, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK, 3Sano Orthopedics, Overland Park, and 4University of Medicine and Biosciences, Kansas City, MO, USA and 4School of Science and Technology, Nottingham Trent University, Nottingham, UK. E-mail: asaithna@sanoorthopedics.com
Accepted Dec 10, 2019; Epub ahead of print Dec 17, 2019
We commend Bélanger et al. (1) on their article entitled “Accuracy of examination of the long head of the biceps tendon in the clinical setting: a systematic review”, and for highlighting concerns about the validity of orthopaedic special tests (OSTs). However, we respectfully disagree with the utilization of shoulder arthroscopy as an appropriate reference standard for determining the sensitivity and specificity of OSTs in the diagnosis of tendinopathy and/or partial tears of the long head of the biceps tendon (LHBT).
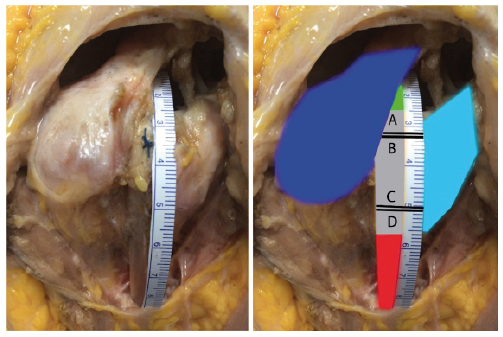
In 2015, Saithna et al. (2) challenged the concept that arthroscopy was an appropriate gold standard for the diagnosis of LHBT pathology and reported, along with other groups, that standard arthroscopic techniques fail to visualize a large proportion of this structure (3–6). In a subsequent systematic review (7), we evaluated whether the length of tendon that can be seen on arthro-scopy allows visualization of areas of predilection of pathology and sought to determine the rates of missed diagnoses at arthroscopy compared with an open approach. We demonstrated that standard arthroscopic techniques only allowed visualization of between 34% and 48% of the overall length of the LHBT. Mean maximum lengths of visualization reported in the literature are summarized and illustrated in Fig. 1.
Fig. 1. Anatomical specimen (right shoulder, viewed anterolaterally). (a) The long head of the biceps tendon (LHBT) is positioned in the bicipital groove. The suture was placed at glenohumeral arthroscopy to demonstrate the maximum length of tendon visualized in this individual specimen. (b) Infra- and supraspinatus (dark blue) and subscapularis (light blue). The LHBT is divided into 3 sections, as described by Denard et al. (9) (green 0–2.5 cm, grey 2.5–5.6 cm and red >5.6 cm). The 4 lines A, B, C and D demonstrate the mean maximum LHBT lengths visualized at arthroscopy in the studies reported by Gilmer et al. (4), Saithna et al. (6), Taylor et al. (5) and Festa et al. (3), respectively. [Modified from Jordan and Saithna, and published with permission from Elsevier] (7).
The failure to visualize a large proportion of LHBT length is a major limitation of arthroscopy because the incidence of pathological changes in distal “hidden” regions has been reported to be high. Moon et al. (8) studied a series of patients who underwent open subpectoral tenodesis at the time of rotator cuff repair. The authors categorized the LHB into the 3 zones, described by Denard et al. (9) (zone A, the proximal 2.5 cm of the tendon; zone B, between 2.5 and 5.6 cm; and zone C, distal to 5.6 cm). The authors reported that the prevalence of degenerative changes and tears was high in all zones, but of specific interest for those areas that are often not visualized (or incompletely visualized), the rate of these diagnoses was 100% in zone B and approximately 80% in zone C. It is therefore unsurprising that 30–50% of diagnoses (7) of LHBT pathology are missed at arthroscopy compared with an open approach. Our systematic review concluded that published sensitivity and specificity data for OSTs that were based on arthroscopy as the gold standard were invalid (7). However, we accept that the use of diagnostic arthroscopy has greater validity for other pathological processes involving the LHBT, such as superior labrum anterior to posterior (SLAP) lesions, dislocation and complete rupture.
We note the conclusion of Bélanger, that “high resolution ultrasound is reliable to diagnose suspected long head of biceps pathologies”. Although this may be the case for dislocation or complete rupture, it is unlikely to be the case for tendinopathy or partial tears, and therefore this message should be clarified. As mentioned previously, tendinopathy and partial tears frequently occur in distal regions of the tendon not visualized on arthroscopy. The majority of studies included by Bélanger et al. that evaluated the ability of high-resolution ultrasound to diagnose tendinopathy and partial tears used arthroscopy as a reference standard. However, because of the high risk of missed diagnoses with arthroscopy, the findings of the review related to this aspect must be interpreted with caution.
Our main aim in writing this letter is to highlight the limitations of arthroscopy in the diagnosis of LHBT pathology, particularly that it does not allow visualization of common sites of distal pathology, and that it is associated with a high rate of missed diagnoses. These limitations must be taken into account in interpreting the systematic review published by Bélanger et al. (1) in clinical practice, and in future studies seeking to evaluate the diagnostic value of OSTs.
The authors report the following potential conflict of interest or source of funding: A.S. receives consultancy fees from Arthrex. The other authors delare no conflicts of interest.
1Department of Physical Medicine and Rehabilitation (Physiatry), Centre Hospitalier Universitaire de Québec – Université Laval, Hôpital de l’Enfant-Jésus, Quebec City, QC, Canada, 2Center for Interdisciplinary Research in Rehabilitation and Social Integration and 3Center for Interdisciplinary Research in Rehabilitation and Social Integration and Department of Rehabilitation, Faculty of Medicine, Université Laval, Quebec City, QC, Canada. E-mail: Valerie.belanger.20@ulaval.ca.
We read the Letter to the Editor by Malik, Jordan and Saithna with interest, and thank them for their comments. According to the cadaveric study and retrospective review (n = 277) cited in their letter (5), 18% of long head of the biceps tendon (LHBT) pathologies are exclusively found in a hidden zone, called the “hidden bicipital tunnel” and cannot be visualized during diagnostic arthroscopy. In that respect, arthroscopy might not have the desired level of perfection for identifying LHBT tendinopathy or partial rupture, and its validity as a reference standard has been questioned (7). We fully agree with them, as tendinopathy and partial rupture of the LHBT can be missed by arthroscopic examination, specifically when the abnormality is found exclusively in the “hidden bicipital tunnel”.
Our review assessed the risk of bias of the original studies with the Quality Assessment Tool for Diagnostic Accuracy Studies (QUADAS-2 tool) (10) and developed review-specific guidance on how to assess the 4 QUADAS-2 items. With respect to this guiding principle, studies using arthroscopy as a reference standard for diagnosing tendinopathy or partial rupture were judged as “unclear” risk of bias for the item appraising the reference standard. Of the 30 studies included in our systematic review, we identified 6 primary studies where arthroscopy was used as a reference standard for diagnosing either tendinopathy or partial rupture (11–16). Five of them also had a blinding issue and were judged “high” risk (11–13, 15, 16), while 1 was deemed as “unclear” risk of bias (14).
We chose to keep these studies in our systematic review since they did not change the results of the meta-analyses or the conclusions of the study. For the accuracy of high-resolution ultrasound (HRUS) for diagnosing tendinopathy, 2 studies used arthroscopy (12, 13), while 1 study had magnetic resonance imaging (MRI) (17) as reference standard. Considering only the latter study, sensitivity and specificity were 1.00 and 0.88, respectively (Fig. 1), while, respectively, they ranged from 0.22 to 1.00 and 0.88 to 1.00, when considering all 3 studies.
For diagnosing any proximal tendon pathology except superior labrum anterior to posterior (SLAP) lesions, which included tendinopathy and partial rupture among other diagnoses, the palpation test, the Speed test, the uppercut test and the Yergason’s manoeuvre were compared with arthroscopy in 3 studies (14–16). As seen in Table I and Table II, the sensitivity and specificity are basically the same when including or excluding the studies that used arthroscopy as reference standard.
From the findings of our systematic review, HRUS is still considered a highly specific clinical tool for the diagnosis of dislocation, complete rupture and tendinopathy when the studies using arthroscopy as reference standard are excluded. The sensitivity is variable for dislocation and complete rupture, but high for tendinopathy. Hence, HRUS is a useful tool in order to confirm a suspected LHBT pathology, but might not be an adequate screening tool. OSTs still offer a poorer diagnostic value, with Yergason’s manoeuvre being the only test of value in order to confirm a suspected pathology (high specificity)
Table I. Overall orthopaedic special tests’ accuracy in characterization of the long head of the biceps tendon (LHBT) pathology except superior labrum anterior and posterior (SLAP) lesions: comparison between meta-analyses that include and those that exclude studies using arthroscopy as gold standard for the diagnosis of tendinopathy or partial tears
Table II. Variation of orthopaedic special tests’ accuracies from individual studies in characterization of the long head of the biceps tendon (LHBT) pathology except superior labrum anterior and posterior (SLAP) lesions, sensitivity, specificity
Gold standards are challenged in order to approach a reality that could never be reached, and today’s gold standards will be replaced by better ones in the future (18). Nowadays, open surgery might be a better reference in order to diagnose “hidden bicipital tunnel” LHBT tendinopathy and partial rupture. In the future, as we concluded in our article, researchers should minimize bias by using, among others, adequate reference standards.


 Click to show fullsize
Click to show fullsize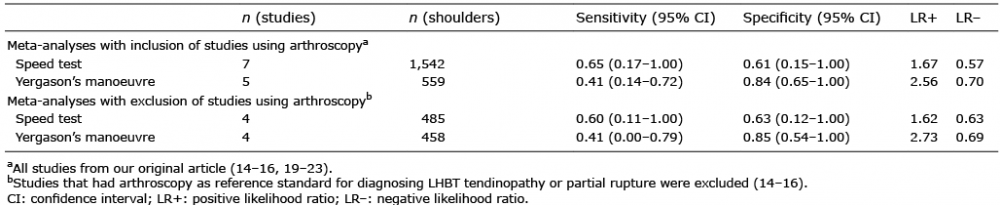 Click to show fullsize
Click to show fullsize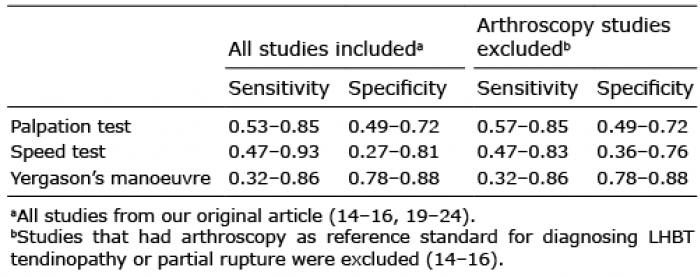 Click to show fullsize
Click to show fullsize