
From the 1Swedish University of Agricultural Sciences (SLU), Department of Work Sciences, Business Economics and Environmental Psychology (AEM), Alnarp, 2Lund University, Department of Health Sciences, 3Lund University, Department of Clinical Sciences Lund, Neurology, Lund, 4Skåne University Hospital, Department of Neurology and Rehabilitation Medicine, and 5Lund University, Department of Clinical Sciences Lund, Orthopaedics, Lund, 6Skåne University Hospital and 7Skåne University Hospital, Data Analytics and Register Centrum, Region Skåne, Sweden
Objective: To determine whether nature-based rehabilitation, as an add-on to standard care, has a long-term influence on post-stroke fatigue, perceived value of everyday occupations, disability, health-related quality of life, anxiety, and depression at follow-up 8 and 14 months after randomization.
Design: Single-blinded, 2-armed, randomized controlled trial.
Methods: Stroke survivors, identified through routine 3-month follow-up visit (sub-acute) or medical records (chronic stroke > 1 year previously), were randomized to standard care + nature-based rehabilitation (intervention group) or standard care alone (control group). Blinded evaluations were conducted at follow-up 8 and 14 months after randomization, for the following outcomes: post-stroke fatigue (Mental Fatigue Scale; MFS), perceived value of everyday occupations (Occupational value instrument with pre-defined items), disability (modified Rankin Scale; mRS), health-related quality of life (Euro-QoL-5 Demension Questionnaire), anxiety (Hospital Anxiety and Depression Scale; HAD) and depression (HAD).
Results: Approximately one-quarter of the screened patients were eligible for inclusion in the study; of these, half agreed to participate; a final total of 101 patients were randomized (mean age 67 years, 60% female). The patients with sub-acute stroke were highly compliant with the intervention. The participants in both the intervention and control groups improved, However, no statistically significant differences in improvement were found between the intervention and control groups for any of the outcome measures. Fatigue decreased to a value below the suggested cut-off for mental fatigue (< 10.5) in the intervention group, but not in the control group.
Conclusion: Nature-based rehabilitation is feasible and well tolerated. A larger randomized controlled trial is warranted.
Key words: horticultural therapy; everyday occupation; quality of life.
Accept Jan 20, 2020; Epub ahead of print Feb 7, 2020
J Rehabil Med 2020; 52: jrm00020
Correspondence address: Anna María Pálsdóttir, Swedish University of Agricultural Sciences (SLU), Department of Work Sciences, Business Economics and Environmental Psychology (AEM), 23053 Alnarp, Sweden. E-mail: Anna.maria.palsdottir@slu.se
We have performed the first randomized controlled study on a nature-based intervention for patients with post stroke fatigue. Nature Based Interventions are performed in outdoor environment especially suitable/adopted for supporting treatment and rehabilitation programs. A total of 101 patients were randomized into a two-armed study: 1) treatment as usual, and 2) nature-based intervention. There were no statistical differences confirmed between the treatments, which may be partly explained by several methodological issues. However, participants showed good compliance with the nature-based intervention; thus, this study contributes with new knowledge to the field of stroke rehabilitation and is ground for further studies on how nature can support recovery from post-stroke fatigue.
Fatigue is common in the early phase of recovery after stroke (reported by 23–75% of people) (1) and continues to affect daily life in the chronic phase after stroke (termed “post-stroke fatigue”; PSF). PSF affects the individual’s everyday life (2), functioning, and can negatively interfere with rehabilitation (1, 3). However, there is insufficient evidence regarding the efficacy of any non-pharmacological intervention for PSF (4–7).
A person’s environment plays an essential role in enhancing the neurological recovery of functioning (8). This is especially the case for an enriched environment, which, compared with standard housing conditions, offers greater possibilities for social and physical stimulation and interaction (9). An enriched environment can promote functional recovery after stroke when combined with multi-sensory stimulation in the rehabilitation setting (10, 11).
Nature-based rehabilitation (NBR) offers both an enriched environment and multiple sensory stimuli
through meaningful nature-based occupations. The NBR setting can include environments, such as designed healing gardens or natural settings, in which the elements of nature dominate over built structures (12–15). NBR has been used for different target groups, with good results regarding general health and well-being (16). NBR could be beneficial as an add-on treatment for individuals recovering from acquired brain injury (17) and improve their physical and psychological function after stroke (18). However, there are few studies on NBR and stroke recovery (17).
The aim of this randomized controlled trial (RCT) was to determine whether NBR, as add-on to standard care, has a long-term effect on post-stroke fatigue, the perceived value of everyday occupations, disability, health-related quality of life (HRQoL), anxiety and depression at follow-up 8 and 14 months after randomization.
Study design
The study design was a single-blinded, 2-armed, RCT (Clinical Trials.gov Identifier: NCT02435043). Patients were enrolled between February 2013 and August 2014. Blinded evaluation by an occupational therapist (OT) was conducted 8 and 14 months after randomization. The final follow-up was completed in November 2015. The study was approved by the regional ethics committee in Lund, Sweden (Dnr 2012/352). All participants provided written informed consent to participate in the trial.
Participants and recruitment
Inclusion criteria were: patients in the sub-acute phase after stroke (3 months after stroke) and patients in the chronic phase (at least 1 year after stroke). Patients, 50–80 years old, who had been admitted to Skåne University Hospital (SUS) at the acute stroke stage; and who were living in Malmö, the third largest city in Sweden, or in nearby smaller municipalities; who were independent in personal activities of daily living (ADL), and reported PSF affecting their daily lives, were invited to participate in the study.
Exclusion criteria were: patients with dementia; severe aphasia; not fluent in Swedish; and/or those with severe comorbidities.
Patients in the sub-acute phase were identified through a routine 3-month follow-up at SUS in Malmö. A stroke nurse interviewed all potential participants by phone (first assessment for eligibility) and then performed a more detailed phone or face-to-face screening assessment (second assessment for eligibility) of the individuals from the first assessment who matched the study criteria.
Patients in the chronic phase were identified through reviewing the medical records of all patients who had being hospitalized due to a stroke during 2011 at SUS in Malmö. A stroke nurse or an OT interviewed all potential participants by phone (second assessment for eligibility) and invited those individuals who matched the study criteria to participate in the study.
A final assessment of eligibility for all patients, in both the subacute and chronic phases, was performed by a physician specialized in stroke (H.P.-R.).
All participants provided written informed consent.
Baseline examination
Baseline examinations were performed by a stroke physician (H.P.-R.), who asked about significant comorbidities and determined the National Institute of Health Stroke Scale (NIHSS) score (19), followed by assessments by an OT, including the Montreal Cognitive Assessment (MoCA) (20) and all outcome measurements to be included in the follow-up assessments (as described below).
Randomization
After completion of the baseline examination, the stroke physician (H.P.-R.) allocated the participants randomly to control or intervention groups by using opaque envelopes. The computational preparation of the adapted block randomization lists was performed using SPSS Software (IBM SPSS Statistics for Windows, Version 22.0.: IBM Corp., Armonk, NY, USA). Patients in the sub-acute and chronic phases were randomized separately.
Intervention
Patients randomized to the intervention underwent a 10-week NBR programme in groups of up to 8 patients, at Alnarp Rehabilitation Garden. Alnarp is located in the countryside, with the longest distance from any patient’s home being approximately 25 km and the shortest 10 km. The 2-hectare garden contains places for work, rest and contemplation (doing and being) and is divided into 2 major areas: the Nature Area (informal and non-cultivated) and the Cultivation and Gardening Area (formal and cultivated). It is further sub-divided into different garden rooms, each designed with special properties for supporting restorative activities or facilitating meaningful horticulture and garden activities (14). There are 2 greenhouses in the garden, one large (100 m2) and one smaller (50 m2).
The NBR programme was grounded in horticultural therapy, supported by a multimodal rehabilitation team that utilized the garden/nature for multi-sensory stimulation for physical, emotional and cognitive stimulation (12). The programme started within 2 weeks after randomization, with continuous admission, and was scheduled for 2 days a week, with each session lasting 3.5 h.
The intervention programme was managed by the OT and horticulturalist, along with the psychotherapist and physiotherapist, who joined the garden sessions. The aim of the intervention was to facilitate rest and mental recovery in an enriched garden environment together with garden and horticultural occupations. All occupations were performed outside, except when the weather was not favourable, during which time the programme was performed in the large greenhouse.
Each day had the same basic structure, with 4 themed sessions: (i) morning gathering with a cup of herbal tea, allowing participants to feel at ease after travelling from their homes; (ii) physical activities, such as a garden walk, tricycling, or “on the spot” exercises, which were held indoors in the greenhouses when the weather was not favourable; (iii) garden and horticultural occupation, in a group or on their own, or “just being” (i.e. mental recovery on their own enjoying the garden); and (iv) gathering for “closure for the day”, with some light refreshments harvested from the garden, fresh or preserved. The last session also allowed participants the opportunity to reflect on their own processes in relation to the NBR.
The participants were considered to have completed the intervention if they had participated for 8 weeks or more. Incomplete intervention was defined as a participation rate of more than 5 weeks, but fewer than 8 weeks, while a participation rate of 5 weeks or fewer was considered “non-intervention”.
Standard care
Standard care after stroke in Sweden is highly individualized, depending on patients’ needs and characteristics, and even on the local organization. It can comprise, for example, physiotherapy and or occupational therapy, and interventions addressing mental health at the primary care level, speech therapy and/or comprehensive outpatient stroke rehabilitation by an interdisciplinary team at the specialist level. Not all patients with mild strokes have access to rehabilitation.
Follow-up assessments 8 and 14 months after randomization
All follow-up assessments were performed by a single OT with extensive experience in stroke care and assessment. The OT was blinded to the allocation of the participants.
Outcome measurements
The primary outcomes in the study were PSF, measured as the total score of Mental Fatigue Scale (MFS), and perceived value of everyday occupations, measured as the total scores for each dimension of Occupational value instrument with pre-defined items (Oval-pd), 8 months after randomization. The secondary outcomes were PSF and perceived value of everyday occupation 14 months after randomization and disability (modified Rankin Scale; mRS), anxiety (Hospital Anxiety and Depression Scale; HAD), depression (HAD) and HRQoL (Euro-QoL-5 Demension Questionnaire (EQ-5D) 3L), 8 and 14 months after randomization.
MFS (21, 22) is a 15-item self-assessment multidimensional questionnaire developed to measure mental fatigue in individuals with neurological disorders, such as stroke and traumatic brain injury. The questionnaire has 15 items that concern issues such as fatigue in general, sensitivity to stress, sleeping disorders, concentration difficulties, sensitivity to sensory stimuli (e.g. sound, smell). Ratings of each described item are based on duration, frequency and intensity, and can vary between 0 and 3 (where 0 = normal function; and 3 = maximum symptoms). A total score is calculated. The healthy population is reported as having a total score of <5, where a MFS score >10 indicates mental fatigue (22).
Oval-pd measures the perceived value of everyday occupations (23). This self-assessment instrument consists of 26 statements on the perceived value of everyday occupations that the participant has performed during the last month. For each statement, 4 response alternative are given: not at all, rather seldom, rather often, and very often. The instrument is composed of 3 core dimensions: concrete, symbolic, and self-reward value, and has high validity and reliability (23). The total scores for each dimension are calculated.
The mRS measures degree of disability or dependence and is the most widely used clinical outcome measure in RCTs in stroke (24). The scale runs from 0 to 6, from absence of symptoms to death. Disability is rated: 1, not significant; 2, slight; 3, moderate; 4, moderately severe; and 5, severe.
The EQ-5D 3L is a generic, widely used questionnaire on HRQoL, consisting of 5 questions covering: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Three alternative responses are provided: no problem, minor problem, and total problem. Based on the categorical answers, a 5-digit number is settled and a total score is determined, by using a tariff (25). The total score can have values between –0.59 and 1.0, where 1.0 corresponds to full health. This study used the UK tariff (26).
The HAD is a widely used screening questionnaire for depression and anxiety. Scores (0–21) for depression and anxiety are calculated, respectively. The different values are grouped into categories as follows: 0–7, no depression/anxiety; 8–10, risk of depression/anxiety; and ≥ 11, possible depression/anxiety (27).
Sample size
PSF in stroke survivors is well described, but as the effect of the NBR intervention is unknown we were not able to calculate a sample size for this trial. Thus, no power calculations were carried out, and the study was instead limited by the period of funding.
Statistical analyses
Outcome variables were analysed according to the intention-to-treat principle, i.e. all randomized and correctly included patients were included in the statistical analysis. All variables were summarized, including mean/median and minimum and maximum values. The change in outcomes was compared between groups using the Wilcoxon rank-sum test and within groups using the Wilcoxon signed-rank test. Missing data were not imputed. The results were considered statistically significant when p < 0.05. Statistical analyses were performed separately for each sub-group (sub-acute and chronic) and for both groups together.
Participants
An initial total of 851 potential participants (374 sub-acute phase, 477 chronic phase) were identified. After the first assessment for eligibility, 345 (183 sub-acute, 162 chronic) possible participants were contacted for a second screening assessment.
Of these, 137 patients (35 sub-acute phase, 102 chronic phase) were excluded based on at least one exclusion criteria, while 208 patients (148 sub-acute phase and 60 chronic phase) fulfilled the inclusion criteria and were invited to participate in the study. Thereafter, 107 patients (75 sub-acute phase, 32 chronic phase) declined to participate, and a final total of 101 patients (73 sub-acute phase, 28 chronic phase) were included in the study (Fig. 1). Of these, 51 patients were randomized to the intervention group (37 sub-acute phase, 14 chronic phase) and 50 to the control group (36 sub-acute phase, 14 chronic phase).
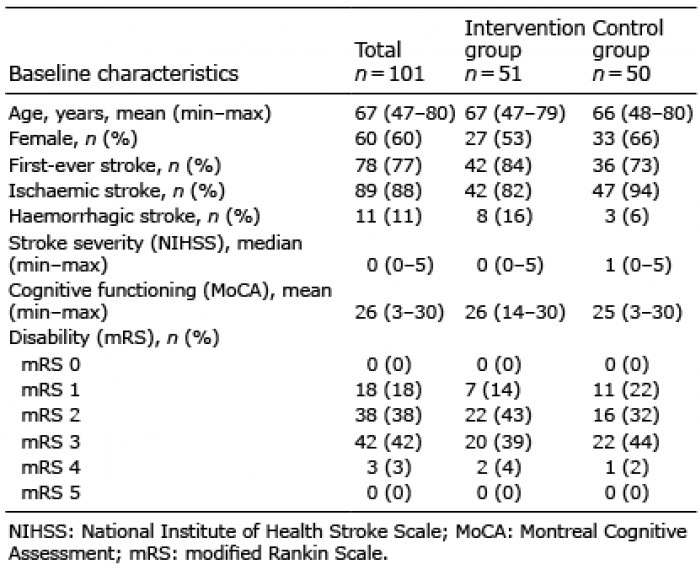
The characteristics of the study population are shown in Table I.
Table I. Characteristics of the study population at baseline
Fig. 1. Enrolment, allocation and randomization of patients for the RTC nature-based stroke rehabilitation.
Compliance with the intervention
Thirty-seven of the 51 participants completed the intervention. More patients in the sub-acute phase (78%) completed the intervention compared with those in the chronic phase (57%). Twenty percent (n = 10) of the patients in the intervention group did not complete the intervention or had a participation rate less than 5 weeks; thus, they are considered as not having participated in the intervention.
Common reasons reported for not wanting to participate were: feeling too tired, and feeling that the journey to and from the rehabilitation garden was tiring and affected their ability to engage in the rehabilitation programme, or that the rehabilitation programme would interfere with other activities; furthermore, some patients expressed that a tiring journey home could counteract the positive effect that had been achieved during the time in the garden.
Recruitment was more successful during the winter, because more individuals declined to participate during summer as they were already involved in outdoor activities, such as golf, gardening or other nature-based/related activities.
Attendance at follow-ups
Four participants died during the course of the study, all before the first follow-up (2 in the intervention group, 2 in the control group); and 9 participants dropped out, (1 in the intervention group, 8 in the control group).
Changes over time between the intervention and control groups
Results for the sub-acute and chronic phases were analysed both by group and together. As there were no differences, only the results of analysis of all participants together are presented here.
No significant differences in improvement were found between the two groups over time for MFS, mRS, HAD anxiety, HAD depression or EQ-5D. No significant differences in improvement were found between the two groups over time for Oval-pd concrete or Oval-pd self-rewarding, while Oval-pd symbolic reached significance at the second follow-up (Table II).
Table II. Differences between groups over time, between baseline and follow-up at 8 months (FU1) and 14 months (FU2) after randomization
Changes over time within groups
All patients, in both the intervention and control groups, improved over time, concerning PSF (MFS), disability (mRS), anxiety (HAD anxiety), and depression (HAD depression) (Table III).
In the MFS at baseline, 58% of all participants scored above the cut-off score of 10.5, suggesting the presence of mental fatigue. Patients in both the intervention group and control group improved between baseline and the first follow-up (8 months); the mean score of the intervention group was below 10.5 at follow-up, and the mean score of the control group was above the cut-off (Table III).
The mean mRS score (disability) improved between baseline and the first follow-up at 8 months in both groups, and between baseline and the second follow-up at 14 months in the intervention group, but not in the control group (Table III).
At baseline, both groups had a mean score for HAD anxiety between 7 and 8, indicating a “risk of anxiety”. HAD anxiety scores were lower at the first follow-up (8 months) compared with baseline in the intervention group, but not in the control group. HAD anxiety scores reached a range below 7, indicating “ no anxiety” in the intervention group at the first and second follow-ups, while the mean score of the control group remained above 7 at both follow-ups (Table III).
Table III. Changes within groups over time, between baseline and follow-up at 8 months (FU1) and 14 months (FU2) after randomization
Both groups had a mean score for HAD depression within the normal range at baseline. Furthermore, both groups’ depression scores were lower at the first follow-up (8 months) than at baseline (Table II).
There were no significant changes in EQ-5D score within any of the groups over time (Table II). There were no changes over time for any dimension of Oval-pd (data not shown).
In this clinical trial the addition of NBR did not result in improved outcomes for patients who experience PSF in comparison with standard care alone. However, the participants showed good compliance with NBR; thus, the study provides a solid foundation for future studies in the effect of NBR post-stroke.
There is a lack of evidence concerning interventions that can improve long-term outcomes for this patient group (3). The MFS score (PSF, primary outcome, where > 10.5 indicates the presence of significant fatigue) showed that a greater proportion of the intervention group reached < 10.5 compared with the control group. As for HAD, the anxiety score reached the normal range in the intervention group at 8 and 14 months, while the control group remained in the borderline abnormal range during the whole follow-up, indicating that NBR may have had some impact on PSF and anxiety.
The participants in both the intervention and control groups therefore improved over time, concerning fatigue, disability, and anxiety, but no statistically significant differences were found in the level of improvement between the intervention and control groups for any of the outcome measurements.
Feeling that travel to the rehabilitation garden would be too demanding was a common reason for not wanting to participate in the study. However, the fact that participants with sub-acute stroke were highly compliant with the intervention could indicate that the NBR programme was well accepted. Patients recovering from stroke enjoyed garden and horticultural activities as a part of their stroke rehabilitation offered at the hospital setting (28). Thus, NBR might be beneficial if implemented into regular rehabilitation settings where the patients would not need to travel far in order to participate in meaningful NBR activities (17, 28).
Improvement between baseline and 8 months was found for most of the outcome measurements in both the intervention and the control groups, while very little to no improvement was seen between 8 and 14 months. The initial improvement may be partially explained by spontaneous improvement in the sub-acute (3 months after stroke) group, as the results of the study are driven by the sub-acute group, which is much larger than the chronic group (data not shown). The study procedure, especially the baseline examination by the physician specialized in stroke and the OT, as well as the follow-up by the OT, may have had a positive impact on both groups and contributed to the improvement. As both groups improved, it may be difficult to show any additional effect of a specific additional treatment/intervention.
The study participants were recruited from an unselected total population of patients, having had a mild to moderate stroke. As in most RCTs in the field of rehabilitation (29), a large number of people were screened for participation, but few could finally be included. The reported reasons for not wanting to participate highlight important aspects to be taken into consideration while designing future rehabilitation programmes and studies, especially if targeting PSF. The rehabilitation facilities should be accessible with as little effort as possible. Furthermore, it is important to design outdoor environments that are suitable for NBR even in winter.
Methodological considerations
We chose to conduct a RCT because it is the method that provides the strongest scientific evidence. The randomization procedure was performed without problems. However RCTs, which are very well suited for testing easily standardized treatments, may be a blunt instrument for evaluating complex interventions, such as rehabilitation, in which multiple processes, outcomes and stakeholders interact (30); therefore, we also performed an interview study of the intervention group, for which the results will be presented elsewhere.
An intention to treat approach was used when analysing the results, which must be considered as a strength. All patients who were randomized at baseline were analysed based on this allocation.
We had planned to include at least twice as many participants, but we did not succeed in recruiting this number despite an extended inclusion period. The difficulties in recruiting participants to rehabilitation RCTs are well described (31); in our study, there were additional difficulties that have been discussed earlier in this paper. Even if the number of participants is rather large in the context of an RCT in rehabilitation, the relatively small sample size may have affected the results.
A limitation of this study is therefore that it is probably underpowered, thus no definitive conclusions can be drawn. Hence, more and larger sample size studies are needed, as well as longitudinal mixed method studies, in order to explore the possible benefits of NBR (17).
A strength of this study is the great efforts that were made to ensure blind follow-up. The OT was blinded to the participant’s group allocation throughout the duration of the study. All assessments were reviewed carefully before the study start to ensure that no questions would be asked during the follow-up that could encourage the participants to reveal whether they had participated in the NBR. The participants were instructed at baseline and before every follow-up not to reveal their allocation to the OT. Some participants did reveal their allocation during follow-up; however, we do not believe that this has affected the results.
The results of this study could indicate that the instruments we chose to study the primary and secondary outcomes may not be sufficiently sensitive to change.
Conclusion
This is the first randomized study of a nature-based intervention for patients with PSF. The patients with sub-acute stroke were highly compliant with the intervention indicating that NBR may be a possible rehabilitation alternative for some patients although no significant differences were found between the intervention and control groups in this possibly underpowered study. NBR should be implemented into rehabilitation settings close to patient’s home. Therefore the study provides a solid foundation for future studies in the field of NBR post stroke.
The authors thank Professor Patrik Grahn and Project Coordinator Sara Kyrö Wissler, at the Swedish University of Agricultural Sciences (SLU); Gerd Andersson, OT; Elisabeth Poromaa, RN; and Cecilia Johnsson, RN, Skåne University Hospital; Anna Geite, OT, and Anna Sundberg, garden engineer, Alnarp Rehabilitation Garden.
Fundings. The study was funded by Region Skåne county council; the Crafoord Research Fund and the Swedish Stroke Association. None of the funding bodies contributed to the design, collection or analysis, interpretation of data or writing of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize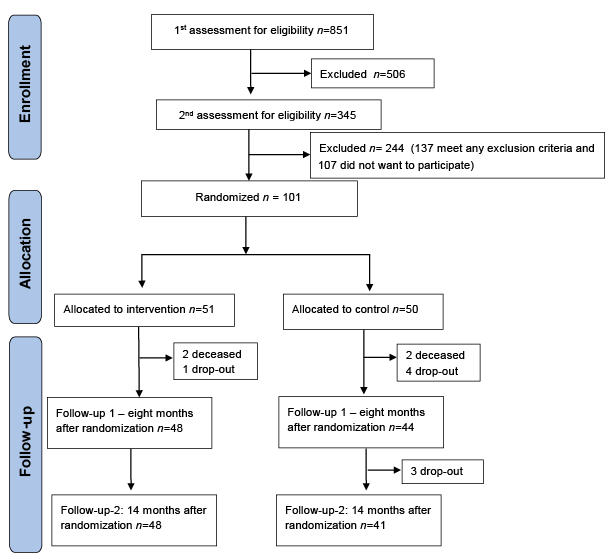 Click to show fullsize
Click to show fullsize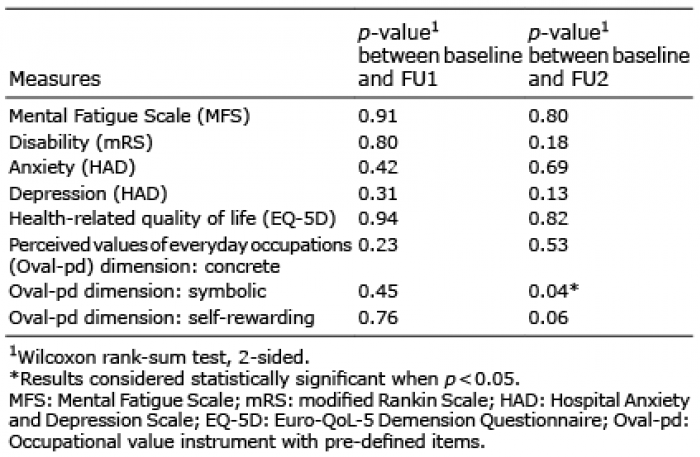 Click to show fullsize
Click to show fullsize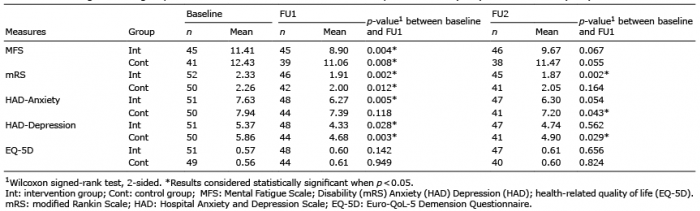 Click to show fullsize
Click to show fullsize