
From the 1Department of Physical Medicine and Rehabilitation, 2Department of Neurology, 3Department of Internal Medicine, Ibaraki Prefectural University of Health Sciences, Ibaraki, Japan
Objective: To investigate the relationship between changes in nutritional status and the functional outcome of adult post-stroke patients hospitalized for rehabilitation.
Design: A cross-sectional study.
Subjects: Post-stroke patients (n = 134) who were admitted to a convalescent rehabilitation ward.
Methods: On admission and discharge, the nutritional status of each subject was assessed using the “controlling nutritional status” system. Activities of daily living were assessed using the Functional Independence Measure (FIM). Patients were divided into 2 categories: (i) those whose nutritional status improved or remained normal during the rehabilitation; and (ii) all others.
Results: The median age of patients was 65.5 years. Although there were no significant differences between the 2 categories in most characteristics, the FIM efficiency was significantly higher (0.230 in the improved category and 0.133 in the other; p < 0.001). Multiple linear regression analysis showed that the improved category as a variable was independently associated with greater FIM efficiency (p < 0.001).
Conclusion: Improvement or maintenance of nutritional status was associated with better functional recovery in post-stroke rehabilitation in adult patients of all ages.
Key words: nutritional improvement; controlling nutritional status; stroke; post-stroke rehabilitation; functional recovery.
Accepted Jan 29, 2020; Epub ahead of print Feb 13, 2020
J Rehabil Med 2020; 52: jrm00028
Correspondence address: Hiroshi Kishimoto, Department of Physical Medicine and Rehabilitation, Ibaraki Prefectural University of Health Sciences, Ami town, Ibaraki, Japan. E-mail: kishimotoh@ipu.ac.jp
This study was conducted to investigate the relationship between functional recovery and nutritional status of adult post-stroke patients hospitalized for rehabilitation. Each patient’s nutritional status and activities of daily living were evaluated on admission and discharge. The 134 enrolled patients were divided into 2 categories: improved or normal nutrition and poor or decreased nutrition. Their functional recovery was better in the category with improved nutritional status. This study significantly augments the results of previous studies focussing on changes in nutritional status and post-stroke rehabilitation outcomes in patients aged >65 years by studying adult patients of all ages.
Convalescent rehabilitation wards, comparable with inpatient rehabilitation facilities (IRF) in North America and Europe, have been developed in Japan by the national medical insurance system since 2000, and have played important roles for patients in post-acute care with stroke, brain injury, hip fracture, spinal cord injury, and disuse of physical function (1). In these wards, numerous patients present with sarcopaenia or malnutrition, which is further associated with worse functional recovery (2, 3). Several studies have shown that nutritional improvement during post-stroke rehabilitation in these facilities correlates with the recovery of activities of daily living among patients with stroke (3, 4), although these investigations focused only on malnourished patients aged ≥ 65 years. However, recent research by the Global Burden of Disease Stroke Expert Group has shown that >30% of stroke incidence worldwide is experienced by patients between the ages of 20 and 64 years (5).
Considering this evidence regarding younger patients, combined with the fact that individuals are generally living longer, the aim of the current study was to examine the association between nutritional improvement and functional recovery during post-stroke rehabilitation among adult patients of all ages. Our metric for nutritional assessment was the Controlling Nutritional Status (CONUT) score (6), which is not limited to individuals aged ≥ 65 years.
Study design
A cross-sectional, retrospective single-centre study, based on data from consecutive patients admitted for post-stroke rehabilitation in the convalescent rehabilitation ward of our hospital, was conducted between April 2010 and March 2015. In this ward, a programme consisting of physical therapy (PT), occupational therapy (OT), and speech therapy (ST), which was tailored to each patient’s disability status, was implemented for approximately 150 min each day. The daily programme time allocation was 40–120 min for PT, 40–120 min for OT, and 0–60 min for ST. Patients with missing data on admission or before discharge, those discharged within 1 month, and those already disabled due to stroke were excluded from the study.
Data collection
Patient background characteristics, including age, sex, stroke type, presence of dysphagia, body mass index (BMI), serum creatinine level, and serum total cholesterol level, were obtained retrospectively from admission medical records. The presence or absence of dysphagia was determined by whether tube feeding or texture-modified meals according to swallowing ability were provided. Nutritional intake counts per day were estimated visually by registered dietitians and nurses, based on the consumption of daily meals once per week from week 1 to 5 after admission. The mean protein and energy intake of each patient was measured (as g or kcal/kg body weight/day).
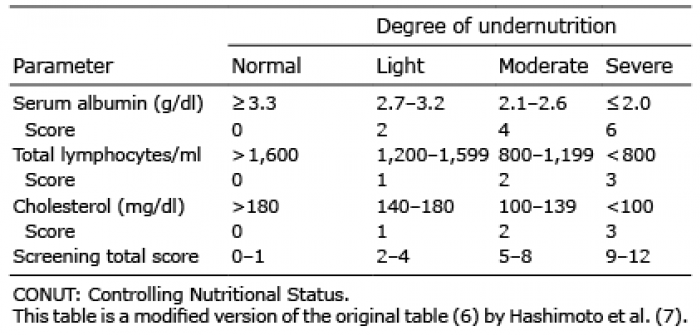
Nutritional status using the CONUT score was assessed on admission and just before discharge. Three parameters were used to calculate the CONUT score: serum albumin level; total cholesterol level; and total lymphocyte count. To better assess the nutritional status of the patients, the present study employed a modified form of the CONUT score that incorporated the corrections by Hashimoto et al. (7) (Table I). This new protocol considers the serum albumin level measured with the modified bromocresol purple method, as performed in our institution, rather than that obtained with the bromocresol green method used in the original work. Furthermore, patients were divided into 2 categories according to the change in CONUT score during rehabilitation: (i) a category with an improvement in CONUT score (IC); and (ii) a category with no improvement in CONUT score (NIC). Patients in whom the score improved (decreased) or remained as normal, i.e. CONUT score 0 or 1, were included in the IC group. Patients in whom the score aggravated (increased) or remained as malnourished, i.e. CONUT score ≥ 2, were included in the NIC group.
Table I. Assessment of undernutrition degree by Controlling Nutritional Status (CONUT) score
Outcome measures
The Functional Independence Measure (FIM) (8), assessed on admission and before discharge, was used as the outcome parameter. FIM efficiency, which was considered a primary outcome, was calculated by dividing the difference in FIM score between admission and discharge by the length of hospital stay.
Comparison of characteristics between included and excluded patients
To confirm differences in characteristics, data regarding age, sex, stroke type, FIM score, serum creatinine level, and serum total cholesterol level on admission, which were available for most of the excluded patients, were compared with those of included patients.
Sample size calculation
G*power 3 (9) was used to calculate the optimal number of samples in this study. In the multiple regression analysis, the sample size was calculated as 109, when α error probability was 0.05, 1–β error probability was 0.8, the number of explanatory variables was 8, and effect size f² was 0.15, assuming a medium (9) effect size. The number of patients included in the current study exceeds this sample size.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics (version 24, 2016, IBM Corporation). Normally distributed data were expressed as mean (standard deviation (SD)), whereas non-normally distributed data were expressed as median value and interquartile range (IQR). The Student’s t-test and Mann–Whitney U test were used to analyse the differences between both categories, as appropriate. Categorical data were expressed as incidences and percentages, with comparisons performed using Fisher’s exact test or the χ2 test, as appropriate. Multiple linear regression analysis was used to examine whether IC was independently associated with FIM efficiency. Multicollinearity was assessed using the variance inflation factor, and p-values < 0.05 were considered statistically significant.
Ethics
The present study was conducted according to the principles of the Declaration of Helsinki and was approved by the ethics committee at our institution. Because this is a retrospective study, an opt-out opportunity for recruitment was provided by announcing the research project in the hospital and via its webpage for 6 months. The eligible patients and their families could withdraw from the study at any time. Therefore, the need for written informed consent was waived.
During the study period, 439 patients were admitted for post-stroke rehabilitation to the convalescent rehabilitation ward in the hospital. The excluded patients were 267 who were not assessed for a CONUT score on admission and/or before discharge, 32 who were discharged within 1 month, and 6 who were already disabled due to a stroke. The remaining 134 patients (85 males; median age, 65.5 years; IQR, 57–74 years) were included in the study (Fig. 1). Of these, 65 (48.5%) patients were aged < 65 years.
Fig. 1. Study flowchart.
Table II shows the characteristics of the 134 patients on admission and the comparisons between the IC and NIC categories. Of the 134 patients, 82 (62.0%) were included in the IC category. Age, days from stroke onset, FIM score, CONUT score, BMI, serum creatinine level, and serum total cholesterol level on admission did not differ significantly between IC and NIC categories. Categorical data, such as sex, stroke type, or presence of dysphagia, did not differ between categories. There was no difference in total length of hospital stay or nutritional intake after admission. However, the FIM efficiency was significantly different between the 2 groups (p < 0.001).
Table II. Patients’ characteristics
Table III shows the results of the multivariate analysis of FIM efficiency following adjustment for confounding factors. Because the obtained variance inflation factor (VIF) values were all < 2, it was concluded that there was no significant multicollinearity among the independent regressors. These results showed that IC, as an explanatory variable, was independently associated with greater FIM efficiency. However, age, sex, dysphagia, CONUT score, FIM score, serum creatinine level, and serum total cholesterol level on admission were not significant variables in predicting FIM efficiency.
Table III. Multivariate analysis of Functional Independence Measure (FIM) efficiency
No differences in age, sex, stroke type, FIM score, serum creatinine level, and serum total cholesterol level on admission were observed between the included and excluded patients (Table IV). Data regarding these characteristics were available for 219 (82.0%) of the 267 excluded patients (due to missing data).
Table IV. Comparison of included and excluded patients
This study indicated that nutritional improvement, or simply maintaining normal nutritional status, was positively associated with effective functional recovery in post-stroke rehabilitation. Adult patients of all ages were included in this study, because most other studies regarding nutrition and post-stroke outcomes have focused on patients aged ≥ 65 years (3, 4). The fact that similar results were obtained despite no age limitation for inclusion suggests that such an association exists in all age groups of adults.
Use of the CONUT system in this study was influenced by the thoroughness with which it has been validated in earlier research applications (10). The CONUT score has been reported to efficiently predict clinical outcome following aneurysmal subarachnoid haemorrhage (11), to be a simple alternative for assessing the nutritional status of individuals who are unable to stand (12), and to monitor the nutritional status of patients with pressure ulcers (13). In the present study, we chose to use the CONUT score, which is not limited to individuals aged ≥ 65 years, although the Geriatric Nutritional Risk Index (14), which explicitly included those aged ≥ 65 years, has been used in previous studies (3, 4) for nutritional monitoring. Furthermore, we proceeded with the view that the CONUT system could be a highly useful nutritional metric in post-stroke rehabilitation.
Because patients are now surviving cerebrovascular accidents more often, and living longer thereafter (15), the post-stroke overall life expectancy, particularly for younger patients, is increasingly being perceived in a new light. Therefore, improvements in nutritional status during rehabilitation several months after stroke may lead to better rehabilitation outcomes, possibly contributing significantly to improvements in quality of life over a substantial number of years, or decades.
In addition to the retrospective cross-sectional design, the present study has several other limitations. First, potential bias may have resulted from including only the patients for whom the CONUT score was estimated both on admission and before discharge. However, as presented in Table IV, there were no significant differences in some characteristics between the included and excluded patients. Secondly, there is an issue of universal applicability, because the present study was conducted within the framework of the medical insurance system of a single country.
In conclusion, the results of this study suggest that nutritional improvement or maintenance of normal nutritional status during rehabilitation in the convalescent rehabilitation ward is associated with better functional recovery in post-stroke adult patients of all ages.
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize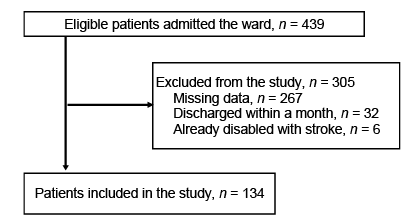 Click to show fullsize
Click to show fullsize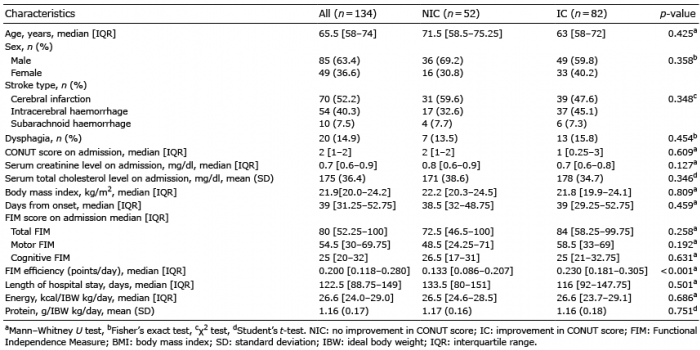 Click to show fullsize
Click to show fullsize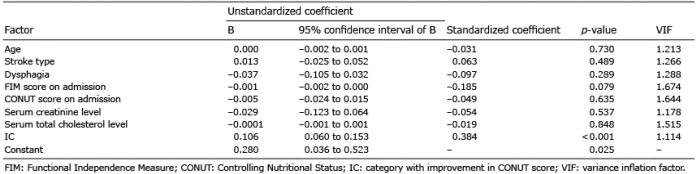 Click to show fullsize
Click to show fullsize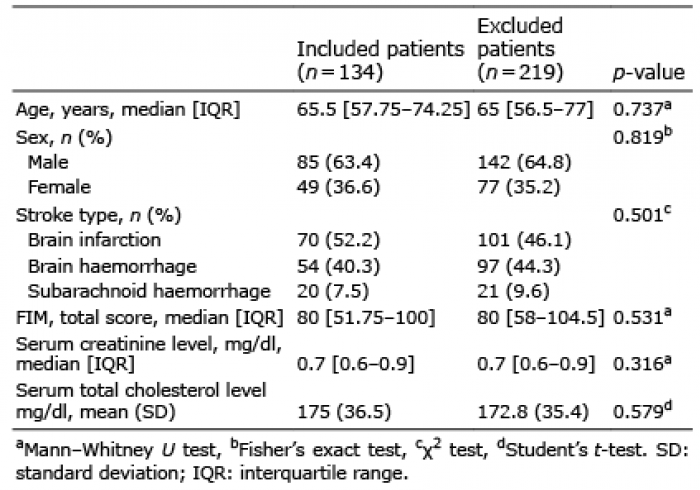 Click to show fullsize
Click to show fullsize