
From the 1Department of Physical and Rehabilitation Medicine, Hacettepe University Medical School, Ankara, Turkey, 2Department of Physical and Rehabilitation Medicine, Doctor Ayten Bozkaya Spastic Children Hospital and Rehabilitation Center, Bursa, Turkey, 3Department of Physical Medicine, Rehabilitation, and Sports Medicine, Department of Physiology and Biophysics, University of Puerto Rico School of Medicine, San Juan, Puerto Rico
Objective: Impairment of physical function is the main determinant of morbidity/mortality in sarcopenia and frailty. Physical function tests are performed by the movement around the joints, and skeletal muscles are the main generators of the forces required to perform these functional tasks. However, the central nervous system, which initiates and coordinates muscle movements, controls the magnitude and temporal parameters of muscle forces.
Methods: Non-systematic literature review was performed about the effects of aging on neuromotor control.
Result: The ability of a muscle to produce force by aging is deteriorated not only by muscle structural changes, but also by neuromotor control dysfunc-tion. With aging, changes in muscle structure and loss of volumes in brain structures related with movement and cognition have been shown. Age-related cognitive impairment can have considerable negative effects on the force generating capacity of skeletal muscles. In this sense, the relationship has been found between hand grip strength, gait speed, and cognition.
Conclusion: Treatments targeting muscle mass only would be insufficient unless we address the impairment of neurocognitive functions. It is essential that prescribing life-long exercise is important for heal-thy aging including the preservation of muscle mass/strength, physical and cognitive functioning, and independent living.
Key words: sarcopenia; physical function; cognitive impairment.
Accepted Mar 18, 2020; Epub ahead of print Apr 7, 2020
J Rehabil Med 2020: 52: jrm00042
Correspondence address: Ayşe Merve Ata, Doctor Ayten Bozkaya Spastic Children Hospital and Rehabilitation Center, Bursa, Turkey. E-mail: amerveata@hotmail.com
Decline of physical function is the main cause of morbidity and mortality in sarcopenia and frailty. Physical function tests are performed to show the daily functional tasks. The central nervous system initiates, coordinates and controls muscle movements. Thus, the ability of a muscle to produce force by aging is determined not only by skeletal muscle, but also by neuromotor control systems. Therefore, treatments should contain targeting muscle mass and also neurocognitive functions. In this regard, an example of a rehabilitation program that influences both muscle and brain function is exercise. Accordingly, it is essential that prescribing life-long exercise is important for healthy and independent aging including the preservation of muscle, physical and cognitive functions.
Impairment of physical function is the main determinant of morbidity and mortality in sarcopenia and frailty (1). This impairment has been attributed mainly to age-related quantitative/qualitative changes in skeletal muscles, which has been accepted as a criterion for the diagnosis of sarcopenia (2). In elderly people, correlations of strength and performance tests with morbidity and mortality are higher than correlations with measurements of muscle mass (3). This is true for 2 very frequently used measurements, such as hand grip strength and gait speed.
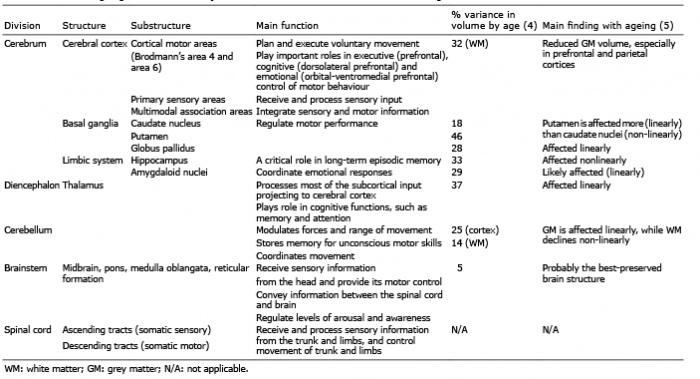
Tests of physical function are performed with appropriate stabilization and movement of the body segments around the joints. Skeletal muscles are the main generators of forces needed to execute these functional tasks. However, the magnitude and temporal parameters of muscle contraction are controlled by the central nervous system. Thus, the force-generating capacity of a muscle is determined not only by its structural features (i.e. muscle mass/quality), but also by the neuromotor control systems mediated by the central nervous system (3). With ageing, not only changes in muscle structure (i.e. loss of muscle mass/quality), but also loss of volume in brain structures related to movement (as well as cognition) are thought to be responsible for the decline in muscle function (Table I) (4, 5).
Table I. Effects of ageing on volumes of major brain structures related to movement and cognition
Age-associated cognitive impairment, which is the loss of intellectual functions, such as thinking, remembering, reasoning, and planning, with age, can have considerable negative effects on the force-generating capacity of skeletal muscles (6). These effects may be mediated by the negative influence of impaired cognition on neuromotor control. There is now substantial evidence to suggest an association among hand grip strength, gait speed, and cognition (6–8). For example, a recent meta-analysis including 9 longitudinal studies in older adults showed a positive correlation (overall r=0.55) between changes in hand grip strength and changes in cognitive function (6). Similarly, other longitudinal studies in older adults have shown that both low hand grip strength and slow gait speed at baseline predict future cognitive decline (9, 10). Furthermore, systematic reviews have shown that hand grip strength is positively associated with global cognition and some cognitive subdomains, including episodic memory, visuospatial ability and working memory (11). Finally, hand grip strength changes were more strongly related to mental state (which declines much later), whereas gait speed changes were more strongly related to changes in fluid cognition (which declines as early as midlife) (12).
All of the above strongly suggest that, during the ageing process, muscle structure and function as well as cognitive ability decrease, and that age-related declines in grip strength and gait speed occur simultaneously with both loss of muscle mass/quality and cognitive impairment. Evidence of this is the fact that the force produced during a maximum voluntary grip strength task is approximately half of what would be expected if the skeletal muscles were fully activated by the nervous system, probably due to impaired muscle activation by the central nervous system (13, 14). Furthermore, it was found that gait speed slows not only in musculoskeletal, but also in peripheral/central nervous system diseases. Walking requires motor coordination, strength and balance, which are regulated by the cerebellum in connection with the cortical associative areas (supporting higher mental func-tion), including the prefrontal cortex, which regulates several aspects of fluid cognition. Since grip strength and gait speed are associated with tasks that require higher neurocognitive processes, these measurements and impairments may also reflect the general health of higher brain functions and the decline in brain health associated with advanced adult age (15, 16).
The association in age-related decline in physical and cognitive functions may be mediated by 1 of 3 mechanisms (6, 11): (i) impaired physical function directly affects cognitive function; (ii) cognitive function directly results in impaired physical function; or (iii) a third factor simultaneously affects decline in both physical and cognitive performance. A “common cause” suggests the presence of an underlying mechanism that drives the association between physical and cognitive functions and the simultaneous presence of both impairments. The “common cause hypothesis” stems predominantly from the evidence for a strong correlation between age-related declines in both physical and cognitive functions reported in cross-sectional studies, and rarely from within-subject changes in longitudinal studies (6, 11, 17). In this regard, a common cause of the ageing process can operate at different physiological levels (12).
Biological changes within the central nervous system, such as white matter hyperintensity, brain ageing, shrinking of the hippocampus, smaller cortical surface area, more cortical thinning, and mitochondrial abnormalities within nerve cells, dopaminergic downregulation, inadequate motor programming/coordination have been put forward as possible underlying mechanisms (8, 13, 18). It should be noted that these mechanisms are not mutually exclusive and may, in fact, work simultaneously. Authors of a recent review have argued that age-related mobility limitations are due to, in large part, to degradations in the central neural control of mobility. While relatively few studies have investigated the role of motor control of basal ganglia and its dopaminergic neurone function in age-related immobility, there is a strong theoretical basis to support such a role (19).
Based on the evidence, the investigation of sarcopenia and its associated functional decline should focus not only on skeletal muscle, but perhaps more importantly on the neuromuscular system including the central nervous system. Treatments targeting skeletal muscle mass only (e.g. nutritional supplementations, myostatin-inhibitors) would be insufficient unless we address the impairment of neurocognitive functions (e.g. with vitamin D, vitamin B12, antidepressants, and possibly dopamine agonists). Herein, a noteworthy example of a rehabilitation intervention that influences both muscle and brain functions would be exercise, i.e. physical activity, which is usually regular and performed to improve or maintain fitness and health (20, 21). Thus, it is reasonable to conclude that prescribing exercise is important for healthy ageing, i.e. preservation of muscle mass/strength, physical and cognitive functioning, and independent living (6, 22). Further longitudinal studies are necessary to better understand the role of central nervous system in age-related loss of muscle mass and function (12).


 Click to show fullsize
Click to show fullsize