
From the 1Department of Neuropsychology and Psychopharmacology, Faculty of Psychology and Neuroscience, Maastricht University, Maastricht, 2Limburg Brain Injury Center, 3Department of Psychiatry and Neuropsychology, School for Mental Health and Neuroscience, Maastricht University, Maastricht, 4Center of Excellence for Rehabilitation Medicine, Brain Center Rudolf Magnus, University Medical Center Utrecht and De Hoogstraat Rehabilitation, Utrecht, 5Clinical Research Department, Rijnstate Hospital, Arnhem and 6Department of Rehabilitation Medicine, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
Objective: Psychological factors influence stroke outcomes, such as participation and quality of life. Although important for clinical practice, not much is known about the temporal stability of these factors. This study explored whether psychological factors are stable post-stroke.
Methods: Prospective longitudinal cohort study. The following psychological factors were assessed using self-report questionnaires at 2 months and at 2 years post-stroke: proactive coping, self-efficacy, extraversion, optimism, passive coping, neuroticism and pessimism. Changes over time, associations and dimensions among psychological factors were considered.
Results: Data for 324 participants were available. Only passive coping scores showed no change between 2 months and 2 years post-stroke. Participants showed less proactive coping, lower self-efficacy, less extraversion, less optimism, more neuroticism and more pessimism over time. All but one inter-correlation of psychological factors, r = [–0.14; 0.71], and all correlations over time, r = [0.42–0.64], were significant. At both time-points, the psychological factors clustered into an “adaptive psychological factor” (proactive coping, self-efficacy, extraversion) and a “maladaptive psychological factor” (passive coping, neuroticism).
Conclusion: Across all psychological factors, changes toward less favourable scores were found. Clinicians should pay attention to adaptive and maladaptive psychological factors among stroke patients during long-term care.
Key words: stroke; psychological factors; rehabilitation; longitudinal studies.
Accepted Aug 7, 2018; Epub ahead of print Oct 26, 2018
J Rehabil Med 2019; 51: 00–00
Correspondence address: Caroline M. van Heugten, NP&PP, FPN, Maastricht University, PO Box 616, 6200 MD Maastricht, The Netherlands. E-mail: caroline.vanheugten@maastrichtuniversity.nl
Every person has a distinct personality. Personality traits may influence how people recover from stroke. This study followed 324 patients in the first 2 years after stroke and examined whether these personality traits are stable over time. We found changes to less favourable outcomes, such as less extraversion, less optimism and more neuroticism. Clinicians should be aware of these changes and stimulate the use of more adaptive psychological factors, such as proactive coping and optimism.
Stroke is a major health problem due to its high prevalence, disabling consequences and risk of recurrence (1). According to the International Classification of Disability, Functioning and Health (ICF), functioning and health are influenced by personal factors, including psychological factors (2). Examples of psychological factors are proactive coping, self-efficacy, extraversion, optimism, passive coping, neuroticism and pessimism.
In stroke, specifically, previous research has revealed associations between psychological factors and participation or quality of life (3–5). Research has shown that proactive coping, self-efficacy, extraversion and optimism are related to better outcomes, whereas passive coping, neuroticism and pessimism are related to worse outcomes (3–7). These strong associations with outcome highlight the importance of gaining knowledge about the properties of these psychological factors, such as their stability after stroke. Knowledge about temporal stability can be used to optimize the timing of psychological assessments and to gain knowledge about whether these factors can be influenced in such a way that outcome can be optimized.
In healthy people psychological factors, especially personality traits, are generally regarded as stable (8). Most studies confirm the temporal stability among psychological factors in healthy adults (9–13), but a few studies have reported changes over time, in e.g. optimism (14) and neuroticism (10, 12). Studies in patients with stroke and similar neurological conditions, such as traumatic brain injury (TBI), have shown mixed findings. Regarding personality traits, inconsistent results across and within factors have been found, and specific evidence remains scarce for patients with stroke (11, 12, 15–17). These inconsistencies are also found with regard to coping (3, 17, 18), possibly also because terminology for subtypes of coping styles differ widely (19).
These inconsistencies and limited findings in patients with stroke show the need for further exploration of the temporal stability of psychological factors. Therefore, the main aim of the current study was to explore whether psychological factors, namely proactive coping, self-efficacy, extraversion, optimism, passive coping, neuroticism and pessimism, are stable over the first 2 years post-stroke. Furthermore, we explored possible clustering of these psychological factors.
The current study was part of the Restore4Stroke cohort study, a multicentre prospective longitudinal cohort study in which patients with stroke were recruited on admission to the acute stroke unit at 1 of 6 general hospitals in the Netherlands and were followed up for 2 years after their stroke. Details of the study procedures are given elsewhere (20). The medical ethics committees of all participating hospitals provided approval. Participants were recruited between March 2011 and March 2013 and all provided written informed consent.
After obtaining participants’ informed consent, information on stroke-related factors (e.g. type of stroke, lateralization, stroke severity, activities of daily living (ADL) dependency) was extracted from the hospital database. Information on demographic factors was obtained from the patient or family members (within the first week post-stroke). At 2 months post-stroke, participants completed self-report questionnaires regarding psychological factors and underwent cognitive screening with a trained research assistant. At 2 years post-stroke, participants completed the same self-report questionnaires regarding psychological factors. The questionnaires were administered on computer or paper and were guided by a research assistant if necessary.
Inclusion criteria of the Restore4Stroke cohort study were: ≥18 years old, having a diagnosis of stroke (ischaemic or intracerebral haemorrhagic lesion) clinically confirmed by the treating neurologist and stroke onset within the last 7 days.
Exclusion criteria were: (i) having a serious other condition that could be expected to influence the study outcomes (e.g. cancer or dementia); (ii) having already been dependent regarding activities of daily living (ADL) before the stroke, as defined by a Barthel Index (BI) score ≤ 17; (iii) having insufficient command of the Dutch language to understand and complete the questionnaires, based on clinical judgment; and (iv) experiencing cognitive decline before the stroke, as defined by a score ≥ 1 on the Heteroanamnesis List Cognition (HLC). The HLC is a 5-item questionnaire, completed by the patient’s spouse, assessing premorbid cognitive dysfunctioning on 5 cognitive domains. Participants who completed the questionnaires for psychological factors at 2 years post-stroke were selected for the current study.
Details and references for all measures are described elsewhere (20).
Demographic and stroke-related factors. Data regarding age, sex, education and marital status (single or in a relationship) were collected. The highest completed level of education was recorded according to the 7-point Verhage system, classifying the Dutch education system into 7 categories ranging from no primary school completed (“1”) to completion of a higher educational level (such as college (“6”) and university (“7”)). Stroke-related factors, such as type (ischaemic, haemorrhagic or unknown/other), lateralization (left, right, cerebellar, brainstem or unknown/other), severity (assessed by the National Institutes of Health Stroke Scale (NIHSS)) and discharge destination (home, or (geriatric) rehabilitation) were collected. ADL was measured with the Barthel Index at day 4 post-stroke and cognitive functioning was measured with the Montreal Cognitive Assessment (MoCA) at 2 months post-stroke.
Psychological factors. All questionnaires to assess psychological factors are reliable and valid in patients with stroke (20). Proactive coping competencies were assessed with the Utrecht Proactive Coping Competence scale (UPCC). The 1-month test–retest reliability is 0.72 (21).The questionnaire consists of 21 items scored on 4-point scale ranging from “not very competent” to “competent”. A mean score is calculated, ranging from 1 to 4, with a higher score indicating a higher level of proactive coping competencies.
Self-efficacy was assessed with the General Self-Efficacy Scale (GSES). The 7-week test–retest reliability is 0.72 (22). The scale consists of 10 items scored on a 4-point scale ranging from “not at all true” to “exactly true”. A sum score is calculated, ranging from 10 to 40, with a higher score indicating a higher level of self-efficacy.
Extraversion and neuroticism were assessed with 2 subscales of the Eysenck Personality Questionnaire Revised Short Scale (EPQ-SS). Both scales consist of 12 items with a dichotomous (yes/no) response option. The 6-month test–retest reliability is 0.85 for optimism and 0.70 for neuroticism (23). A sum score is calculated, ranging from 0 to 12, with a higher score indicating a higher level of extraversion or neuroticism, respectively.
Optimism and pessimism were assessed with the Life Orientation Test Revised (LOT-R). The 4-month test–retest reliability is 0.68 (24). It consists of 10 items, with 3 items measuring optimism, 3 items measuring pessimism and 4 filler items. The items are scored on a 5-point scale ranging from “strongly disagree” to “strongly agree”. A score is calculated per subscale, ranging from 0 to 12, with a higher score indicating a higher level of optimism or pessimism, respectively.
Passive coping was assessed with the passive reaction pattern subscale of the Utrecht Coping List (UCL). The 6-week test–retest reliability is 0.84 for the passive reaction pattern subscale (25). The questionnaire consists of 7 items, scored on a 4-point scale ranging from “seldom” to “very often”. A sum score is calculated, ranging from 7 to 28, with a higher score indicating a higher level of passive coping.
Preparatory analyses. All data analyses were performed using SPSS Statistics 24.0 for Windows (IBM Corp., Armonk, NY, USA). Missing data were inspected and imputed with the mean value within the corresponding subscale if at least 80% of the participant’s data of the specific questionnaire was available. For the GSES, the criterion suggested by the manual of at least 70% non-missing data was used. Data were inspected for normality and outliers. In case of non-normality (skewness or kurtosis value <–1 or >+1), data were transformed. Skewness to the right was resolved with a logarithmic transformation. A quadratic transformation was executed to resolve skewness to the left. All analyses were performed using an alpha level of 0.05.
Baseline differences. Group differences on baseline characteristics between the included and excluded participants were analysed using Pearson χ2 tests for nominal variables including all available levels, independent t-tests (T) for normally distributed continuous variables, and non-parametric tests (Mann-Whitney U test) for continuous variables in case of non-normality.
Changes over time. To reveal changes over time, paired samples t-tests were performed. For further inspection, changes over time were categorized into 3 categories: “worse”, “equal” and “better”. Hereby, we used a change of 0.5 SD as pragmatic indicator of change of the psychological variable score over time, as suggested by Norman et al. (26). For the variables proactive coping, self-efficacy, extraversion and optimism, an increase of more than 0.5 SD over time was considered an adaptive change (“better”) (see Introduction). For the variables passive coping, neuroticism and pessimism an increase of more than 0.5 SD over time was considered a maladaptive change (“worse”) (see Introduction). A change of less than 0.5 SD over time was considered as no change over time (“equal”). Effect sizes were calculated using Glass’s delta (27).
Correlation and factor analyses. To explore associations among the psychological variables, Pearson correlations were calculated and interpreted as suggested by Evans (28) (≤ 0.19 very weak; 0.20–0.39 weak; 0.40–0.59 moderate; 0.60–0.79 strong; ≥ 0.80 very strong). To explore dimensions among the psychological variables, exploratory factor analysis (EFA) (including the extraction methods principal axis factoring and maximum likelihood estimation) was performed using data from participants who completed all questionnaires at both time-points (n = 282). Factor extraction was based on multiple criteria, as suggested by Osborne & Costello (29).The K1 criterion (eigenvalue ≥1.0), the Scree plot, small residual correlations ([–0.1; 0.1]) and a non-significant goodness-of-fit test (based on maximum likelihood estimation) were used as 4 indicators for extraction. If the criteria suggested multiple solutions for factor extraction, e.g. a 1-factor structure on the basis of the Scree plot and a 2-factor structure on the basis of the K1 criterion, all suggestions of factor extraction were executed and the best solution, indicated by smaller residual correlations and a non-significant goodness-of-fit test, was chosen. Only factor loadings greater than 0.30 were displayed. Because we expected the factors to be correlated, Oblimin rotation was preferred over Varimax rotation.
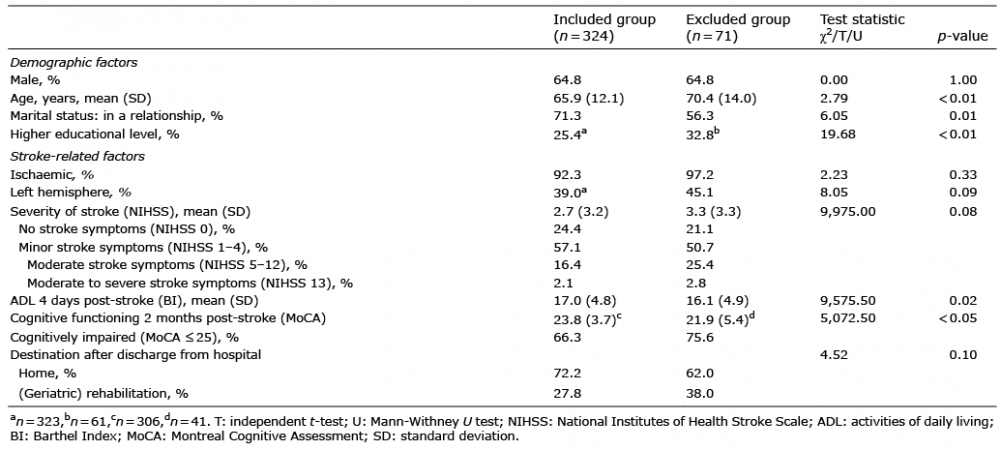
Of the 395 participants in the Restore4Stroke cohort, 324 (82.0%) provided data on psychological factors at 2 years post-stroke and were included in the current study. Furthermore, depending on the psychological factor, imputation was performed for 0.0–9.6% of participants. Baseline characteristics of both the included group (n = 324) and excluded group (n = 71) and significant differences between them are shown in Table I. The participants in the included group were significantly younger, less often highly educated and more often involved in a relationship in comparison with the excluded group. Regarding stroke-related factors, the included group had a significantly higher level of cognitive functioning 2 months post-stroke and a significantly higher level of independence in ADL 4 days post-stroke in comparison with the excluded group.
Table I. Patients’ characteristics at baseline
Table II provides the results of the temporal stability analysis of psychological factors. All psychological factors except passive coping showed significant changes over time. At 2 years post-stroke, participants reported less proactive coping, lower self-efficacy, less extraversion, less optimism, more neuroticism and more pessimism in comparison with 2 months post-stroke. The largest effect sizes were found for optimism (Glass’s Δ = –0.58) and proactive coping (Glass’s Δ = –0.42). Furthermore, looking at changes over time (“worse”, “equal”, “better”), 28.6–46.8% participants showed changes in a negative direction and 10.7–22.7% improved across all psychological factors.
Table II. Temporal stability of psychological factors
For all psychological factors moderate or strong correlations were found between scores at 2 months and 2 years post-stroke, ranging between 0.42 and 0.64 (Table II). In Table III correlations among the various psychological factors within each time-point are reported.
Table III. Correlations of psychological measures at 2 months post-stroke (below the diagonal) and at 2 years post-stroke (above the diagonal)
At 2 months post-stroke, all psychological factors correlated significantly with each other, except for extraversion with neuroticism. The correlations ranged between very weak to strong. The highest correlation was found between proactive coping and self-efficacy (r = 0.62).
At 2 years post-stroke, all psychological factors correlated significantly with each other. The correlations ranged between weak and strong. The highest correlation was again found between proactive coping and self-efficacy (r = 0.71). Overall, correlations at 2 years were somewhat stronger compared with 2 months.
The correlations among the psychological variables at both time-points were best described by the extraction of 2 factors using principal axis factoring as EFA extraction method (Table IV). After factor extraction and oblimin rotation, the factor correlation was 0.58 and –0.70 at 2 months post-stroke and 2 years post-stroke, respectively. The pattern matrices of both time-points, consisting of the factor loadings after oblimin rotation, are shown in Table V. For interpretation purposes, factor loadings on factor 1 at 2 months post-stroke were inverted.
Table IV. Exploration of factor structures at 2 months post-stroke and 2 years post-stroke
Table V. Factor loadings based on exploratory factor analysis after Oblimin rotation
At 2 months post-stroke, factors 1 and 2 are labelled as “maladaptive psychological factor” and “adaptive psychological factor”, respectively. Passive coping and neuroticism had positive loadings on the maladaptive factor, whereas optimism had a negative loading on this factor. Proactive coping, self-efficacy, extraversion and optimism had positive loadings on the adaptive factor. Pessimism did not load on any factor. The explained variance of the 2 factors together was 43.6%.
At 2 years post-stroke, factors 1 and 2 are labelled as “adaptive psychological factor” and “maladaptive psychological factor”, respectively. Proactive coping, self-efficacy and extraversion had positive loadings on the adaptive factor. Passive coping, neuroticism and pessimism had positive loadings on the maladaptive factor. Furthermore, optimism had a negative loading on this factor. The explained variance of the 2 factors together was 54.8%.
This study found that scores on measures of psychological factors changed during the first 2 years post-stroke. The psychological factors were moderately to strongly correlated with each other and over time and clustered at both time-points into 2 factors: an “adaptive psychological factor” (proactive coping, self-efficacy, extraversion) and a “maladaptive psychological factor” (passive coping and neuroticism). Scores on all adaptive psychological factors decreased over time, whereas scores on maladaptive psychological factors increased or remained stable (passive coping) over time. The added value of our study is that we evaluated the temporal stability of multiple psychological factors simultaneously in a large cohort of patients with stroke using a longitudinal design.
To the best of our knowledge, the finding of a negative temporal impact across all psychological factors post-stroke has not been demonstrated previously. As mentioned in the introduction, previous research on temporal stability of psychological factors in stroke and other populations showed inconsistent results across and within psychological factors, possibly due to the use of different measures, time-points and designs.
Strikingly, even though the sample consisted mainly of patients with a mild stroke overall changes in a negative direction were found. In comparing our results with previous findings regarding temporal stability of psychological factors in healthy populations, we found different patterns of changes over time. Most studies assessing psychological factors in healthy adults showed temporal stability (9–14), whereas our data showed temporal changes in a negative direction across all psychological factors. This suggests that the occurrence of a stroke could be a possible cause of the observed negative changes over time.
The occurrence of stroke results in negative changes regarding emotional, cognitive and energy resources, which could provide an explanation for the observed negative change of psychological factors over time. After a stroke, many patients suffer from depression (30), cognitive complaints (31) and disabling fatigue (32), increasing their burden and calling on their reserves of resilience. The observed negative changes in psychological factors could be concomitant with these negative emotional, cognitive and energy changes. In fact, it was shown that neuroticism is concomitant with depressive symptoms (33), and that cognitive complaints in patients with traumatic brain injury (TBI) are associated with the use of maladaptive coping styles (7). In our sample, 66% were considered to be cognitively impaired (MoCA score ≤ 25) at 2 months post-stroke. Furthermore, Wu et al. (32) proposed a biopsychosocial model including psychological factors as an explanation for fatigue after stroke. Taken together, stroke is associated with negative changes in emotional, cognitive or energy resources. These consequences of stroke may form an explanation for the negative changes observed in psychological factors.
Although the occurrence of stroke provides a possible explanation for the significant differences over time on all measures except for passive coping, it remains unclear whether damage to the brain (i.e. the stroke) or the fact that a stroke is a negative life event (such as a cardiac event) or the chronic character (as in other diseases, such as diabetes) or their combination may induce changes in psychological factors. From earlier studies we know that patients with acquired brain injury make more use of passive reactions and less use of problem-solving coping styles than the general population (7), which may be related to the damage to the brain. From studies on survivors of a cardiac arrest we know that the impact of the event plays an important role in the quality of life in the long term (34); therefore distress may also influence psychological functioning. A study on chronic diseases (35) also found changes over time in extraversion and neuroticism after the onset of chronic diseases, such as heart disease, respiratory disease and stroke. Future studies are needed to relate the observed negative changes to stroke, brain damage, a negative life event, chronic character of the disease or their combination.
Furthermore, one could argue whether these changes comply with the minimal clinically relevant change of these measures and therefore represent clinically relevant changes and/or changes due to measurement error. Because this information is not available, we chose 0.5 SD as pragmatic indicator of change, as suggested by Norman et al. (26). Future research should provide the minimal clinically relevant change per measure to investigate whether the changes observed in this study represent clinically relevant changes. Even if the observed changes do not reflect clinically relevant changes and thus suggest temporal stability, our findings imply, at the very least, that the psychological factors investigated do not improve naturally to a more beneficial level and, consequently, do not foster improved outcomes in terms of participation and quality of life.
To examine whether psychological factors can be modified by treatment programmes, systematic reviews and meta-analyses provide some evidence for the ability to change depression, anxiety, self-efficacy and coping by means of psychological therapy, to possibly improve the outcomes of patients with stroke in terms of quality of life and participation (36–40). Given these positive findings related to the modifiability of some psychological factors, treatment could be aimed at enhancing adaptive psychological factors and limiting maladaptive psychological factors in order to improve participation and quality of life of patients with stroke. However, to provide more insight for the development of such focused and personalized treatment, future research should reveal which patients are at risk of the negative changes over time regarding psychological factors.
Another implication is related to the occurrence of 2 clusters, namely an “adaptive psychological factor” (proactive coping, self-efficacy, extraversion) and a “maladaptive psychological factor” (passive coping and neuroticism). This could suggest the use of a single measure of adaptive psychological factors and a single measure of maladaptive psychological factors for subsequent studies. However, more research is needed to replicate these findings and provide direction for the selection or development of such measures. Also it should be noted that at 2 months post-stroke, pessimism did not load on the extracted factors, whereas optimism loaded on both factors. At 2 years post-stroke, pessimism did load on the adaptive psychological factor, but optimism, although inverted, also loaded on this maladaptive factor and not, as expected, on the adaptive factor.
While interpreting the results of our study, the following limitations should be taken into account. First, the homogeneous sample could limit the generalizability of our results to the entire stroke population or to other patient populations. Most patients in our study had a minor ischaemic stroke. An explanation for this homogeneity is that mild stroke comprises the largest group of stroke patients and patients with a severe ischaemic stroke or a haemorrhagic stroke are less often present, are less often referred to general hospitals, have greater difficulty understanding the questionnaires or study instructions and are less able to provide informed consent within the first week (4). Future research could investigate the temporal stability of psychological factors in patients with a more severe or haemorrhagic stroke. Furthermore, it would be interesting to examine whether, in other patient populations with mild brain injuries, such as mild TBI, or in other chronic diseases with a sudden onset, the same negative effect of time is seen to reveal whether these changes are specific for a mild brain injury (stroke or mild TBI) or related to a more general cause, such as the onset of a disabling chronic disease or occurrence of other significant (health-related) life events. Secondly, psychological factors were measured at 2 time-points, 22 months apart. To provide evidence for the existence of linear or non-linear time effects and to reveal time-related changes within this time period psychological factors should ideally be assessed at more time-points. Thirdly, time-dependent relationships with regard to depression, anxiety and other psychological factors, such as locus of control, sense of coherence and resilience were not considered in this study. This limits any conclusion regarding these other psychological factors or the existence of a mediating role, which might be played by a more general negative emotional state (33).
Despite these limitations, we found, in a large prospective longitudinal multicentre cohort study across 7 different psychological factors in patients with stroke, changes toward less favourable scores, which may be associated with worse outcome, such as participation and quality of life. Clinicians should attend to adaptive psychological factors (e.g. proactive coping, self-efficacy, extraversion) and maladaptive psychological factors (e.g. passive coping and neuroticism) during long-term care.
The presented study is part of the Restore4Stroke Research Program, which is supported financially by VSBfund (grant no. 89000004) and coordinated by ZonMw (the Dutch Organization for Health Research and Development).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize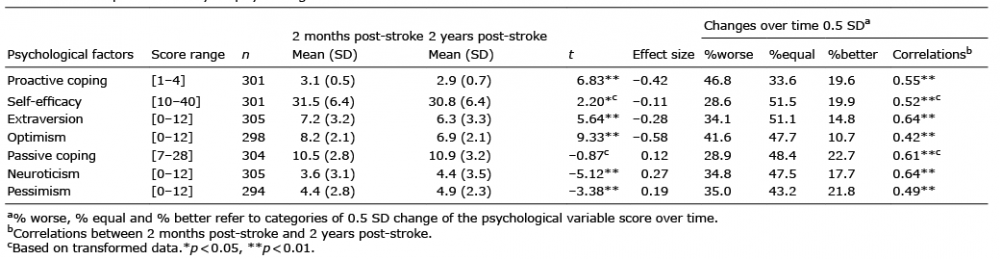 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize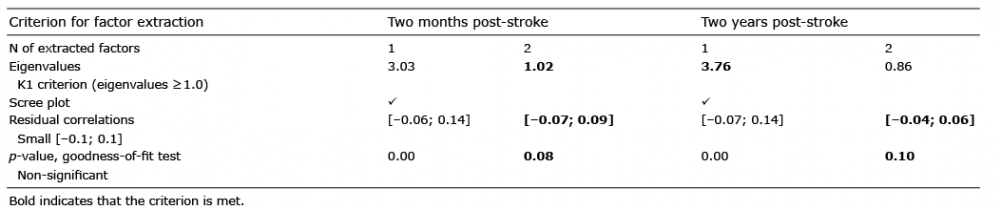 Click to show fullsize
Click to show fullsize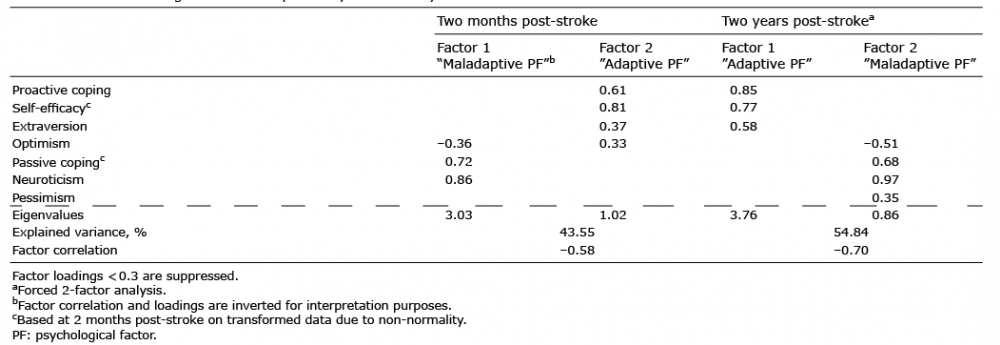 Click to show fullsize
Click to show fullsize