
From the 1National Advisory Unit on Rehabilitation in Rheumatology, Department of Rheumatology, Diakonhjemmet Hospital, Oslo, 2St Olavs Hospital, Trondheim University Hospital, Trondheim, 3Haukeland University Hospital, Bergen, 4Haugesund Rheumatism Hospital AS, Haugesund, Norway and 5Centre for Health Sciences Research, University of Salford, Salford, UK
Objective: To assess construct validity (Rasch analyses) of the Measure of Activity Performance of the Hand (MAP-Hand) in people with carpometacarpal osteoarthritis (CMC1 OA), and to explore differences in activity performance between people with CMC1 OA and those with rheumatoid arthritis.
Design: Cross-sectional study.
Subjects: A total of 180 people with CMC1 OA referred for surgical consultation were recruited from rheumatology clinics in Norway, and 340 people with rheumatoid arthritis were recruited from outpatient rheumatology clinics in the UK.
Methods: The MAP-Hand consists of 18 predefined items scored on a 4-point scale from 1 (no difficulty) to 4 (unable to do), from which a mean score is calculated. Construct validity was assessed using Rasch analyses. Differences between the 2 groups were assessed using an independent sample t-test at the group level and differential item functioning (condition as grouping variable) at the item level.
Results: Some mis-targeting of data and clusters of dependency were found, but the MAP-Hand scores showed an overall fit to the model. No between-group difference in total mean MAP-Hand score was found, but there were significant differences between the 2 groups on item levels.
Conclusion: The MAP-Hand showed satisfactory construct validity and could differentiate between people with CMC1 OA and those with rheumatoid arthritis on item levels.
Key words: hand; osteoarthritis; arthritis; self-report; psychometrics.
Accepted May 5, 2020; Epub ahead of print May 28, 2020
J Rehabil Med 2020; 52: jrm00070
Correspondence address: Anne Therese Tveter, Norwegian National Advisory Unit on Rehabilitation in Rheumatology, Department of Rheumatology, Diakonhjemmet Hospital, PO Box 23 Vinderen, N-0319 Oslo, Norway. E-mail: AnneTherese.Tveter@diakonsyk.no
This study evaluated the use of the Measure of Activity Performance of the Hand (MAP-Hand), which is an 18-item questionnaire based on patient´s own perception of activity limitations of the hand. The questionnaire was tested in 180 people with osteoarthritis of the base of the thumb and showed that the questionnaire was suit-able for use in this patient group. We also compared the scoring of people with hand osteoarthritis to the scoring of 340 people with rheumatoid arthritis and found that, although the total mean score of the questionnaire was the same, the 2 patient groups showed different activity limitations of the hand. While people with hand osteoarthritis had more problems with fine hand use, people with rheumatoid arthritis showed more problems with carrying and pushing items. Further research is needed to evaluate whether the questionnaire may be suitable for use in clinical trials and clinical practice in patients with different forms and stages of hand osteoarthritis.
Osteoarthritis (OA) and rheumatoid arthritis (RA) both affect the hand joints. Whilst RA is an autoimmune inflammatory joint disease (1), OA is mainly characterized by an imbalance between degeneration and regeneration of the cartilage, although there is also some degree of synovial inflammation (2). Despite their different aetiologies, OA and RA in the hand joints lead to comparable disease burden and clinical symptoms, such as increased pain and stiffness, and reduced range of motion, muscle strength and hand function (2–4). However, there are also important differences between the 2 conditions. RA can be highly destructive of joints, affecting the wrist, thumb, metacarpophalangeal (MCP), and interphalangeal joints (1). In comparison, hand OA (HOA) is most prevalent in the distal interphalangeal (DIP), proximal interphalangeal (PIP) and 1st carpometacarpal (CMC) joints (5). Compared with people with HOA, people with RA have equal or poorer health-related quality of life (6, 7), and greater reductions in physical function, grip- and pinch strength (7, 8). Despite this, self-reported activity limitations are comparable in the 2 conditions (8). In-depth evaluation of specific activity limitations in each of these conditions can be useful for targeted treatment planning.
There is no cure for OA or RA. Even though medication has dramatically improved outcomes of RA (1), there are still people requiring conservative treatment. For people with HOA, conservative treatment is the first line of treatment (9). In order to assess the extent of activity limitations, monitor disease progression and evaluate effects of treatment, there is a need for reli-able and valid patient-reported outcome measurements (PROMs) that can be used by therapists in a clinical setting. Several hand and upper limb PROMs exist, such as the Australian/Canadian Hand OA Index (AUSCAN), the Functional Index for Hand OA (FIHOA) or the Michigan Hand Outcome Questionnaire (MHQ) (10); however, these are mostly based on items selected by clinicians and not on what is important to patients (11). Thus, the Outcome Measures in Rheumatology (OMERACT) HOA working group has highlighted the need for PROMs that include patient perspectives for use in clinical trials and observational studies (12).
The Measure of Activity Performance of the Hand (MAP-Hand) has included the patient perspective by being based on descriptions of activity limitations in people with RA (13). The measure is shown to be reliable and valid in people with RA (13, 14). Studies assessing the construct validity of the MAP-Hand using Rasch analyses in people with RA in Norway (13) and in the UK (14) concluded that the MAP-Hand satisfied the Rasch model requirements after some adjustments. Assessment of the measurement properties of the MAP-Hand has also been conducted in people with HOA, showing acceptable reliability (15) but conflicting evidence regarding its validity (15, 16). In addition, it has not been assessed whether the questionnaire satisfies the Rasch model requirements in people with HOA with specific involvement of the carpometacarpal joint (CMC1).
The main aims of this paper are: (i) to test the construct validity (Rasch analyses) of the MAP-Hand in people with CMC1 OA, and (ii) to explore differences in activity performance of the hand in people with RA vs people with HOA with specific involvement of the CMC1 joint.
Carpometacarpal joint osteoarthritis-sample
People referred for surgical consultation due to CMC1 OA were recruited from 3 rheumatology clinics in Norway (Trondheim University Hospital (St Olav’s Hospital), Haukeland University Hospital and Haugesund Rheumatism Hospital) between April 2013 and June 2015 as part of a randomized controlled trial (RCT) (trial registration identifier: NCT01794754) (17). Study design and data collection of this RCT are described in detail elsewhere (17). People who did not read, write or speak Norwegian or had cognitive deficits were excluded. Eligible people were screened by a local project coordinator (occupational therapist (OT)) at each hospital. Those giving their written informed consent were included. The study was approved by the Regional Ethics Committee in Norway (2012/2265/REK sør-øst C).
Baseline data from people with CMC1 OA in that RCT (n = 180) are used in this analysis.
Rheumatoid arthritis sample
People diagnosed with RA by a rheumatology consultant were recruited between July and November 2013 by research nurses from 17 outpatient rheumatology clinics in the UK, who were participants in a previous outcome measure study. Study design and data collection are described elsewhere (14). People were excluded if they were unable to read, write and understand English; or were about to or recently started or increased dose of a biologic or disease modifying anti-rheumatic drug (DMARDs) in the last 3 months. Prior to the start of the study, ethical approval was obtained from the Ethical Committee North West (12/NW/0841) and the University of Salford Research Ethics Panel.
Baseline data from people with RA in that study (n = 340) are used in this analysis.
Variables
Measure of activity performance of the hand (MAP-HAND). Activity performance was measured using the MAP-Hand, which is an 18-item sex- and season-neutral PROM measuring activity performance of the hand, originally developed for use in people with RA (13). The item generation of this questionnaire was based on patients’ description of activity limitations in people with RA (13). The 18 predefined items are scored on a 4-point scale from 1 (no difficulty) to 4 (unable to do). A total mean score can be calculated (for a minimum of 15 items). The questionnaire also includes the possibility to formulate and score up to 5 optional patient-specific items but given the patient-specific nature of these items, they are not included in the current study.
Demographic variables. All participants answered a set of sociodemographic and clinical variables, including age, sex, education level, work status, marital status, handedness, referred hand, disease duration, pain and use of analgesics/type of medication. All variables were used to describe the samples, while age and sex additionally were used as variables in the Rasch analyses. Age (years) and sex (male/female) were collected in the same manner in both samples. However, education level, work status, and marital status were collected differently. Thus, education level was dichotomized into below vs at or above bachelor’s degree level. Work status included full- or part-time work, homemaker, student, unemployed and retired in both samples. The Norwegian sample could respond to more than one category. Long-term sick leave and early retirement due to ill health (UK) were grouped together with sick leave, work assessment allowance and disability pension (Norway). For marital status, the Norwegian sample was only asked if they were living together with someone or not. UK participants answering married or living with a partner were grouped as living together with someone, while those reporting to be single, divorced, separated, or widow/widower were grouped as living alone. Handedness was recorded in the CMC1 sample, but not in the RA sample. The referred hand for surgery was collected from the patient medical records for the CMC1 OA sample (right, left or both hands). Disease duration was self-reported and measured in years. Both samples reported pain on a numeric rating scale (NRS) from 0–10, where 0 is no pain and 10 is worst pain (18). Pain was specific to the referred hand for the CMC1 OA sample, and numbers are given as right, left or the mean of both hands depending on the referred hand. Pain for the RA sample was for both hands. The CMC1 OA sample reported if they used analgesics or not, whilst the RA sample reported medication type. Medication type for the RA sample was either biological disease-modifying anti-rheumatic drugs (DMARDs), combination therapy (people on two or more synthetic DMARDs or one synthetic DMARD plus prednisolone), monotherapy (people on one synthetic DMARD) or not on DMARDs (people on steroids only or analgesics only).
Analyses
Demographic variables were assessed using Stata version 15. Variables are presented as: mean (standard deviation (SD)) or median (interquartile range, 25th and 75th percentile) if continuous; and number and percentage if categorical. Differences in demographic variables between CMC1 OA and RA samples were assessed with independent Samples t-test or Mann–Whitney U test for continuous data and either χ2 or Fischer’s exact test for categorical data. The p-value for these analyses was set to ≤ 0.05.
Construct validity (Rasch analyses) of the MAP-Hand in people with carpometacarpal joint osteoarthritis
Rasch analyses (conducted in RUMM2030), as described by Tennant & Conaghan (19), were used for the assessment of construct validity of the MAP-Hand scores in people with CMC1 OA. To assess the difference between the observed responses and that expected by the Rasch model, χ2 statistics were used for testing of model fit, which should be non-significant. With Bonferroni correction, a significant value for 18 items was set to p < 0.002. We considered the individual person and item fit by assessing standardized item and person residuals, where the summary mean residual should be zero and the summary standard deviation residual should be 1 for perfect fit to the model. Mis-targeting of persons or items were assessed by person and item location, where misfitted persons were removed if item person fit residual exceeded +2.5. Threshold ordering of the items was assessed to evaluate if the categories were suited for people with CMC1 OA. Differential item functioning (DIF) for sex and age group (dichotomized into 40–59 and 60–80 years) was also assessed for both uniform and non-uniform DIFs. Residual principal components analysis was used to evaluate unidimensionality of the MAP-Hand items. Local dependency was examined through a residual correlation matrix. If local dependency was violated (i.e. mean correlation was ≥ 0.20), items were grouped to absorb dependency.
Differences in activity limitation between carpometacarpal joint osteoarthritis and rheumatoid arthritis patients
An independent Samples t-test was used to assess the difference in total mean MAP-Hand score between RA and CMC1 OA samples, with the p-value set at ≤ 0.05 (Stata version 15). Differential item functioning (DIF), with condition as the grouping variable (person factor), was used to assess differences (Bonferroni adjusted p-value of < 0.002) in individual items (RUMM2030).
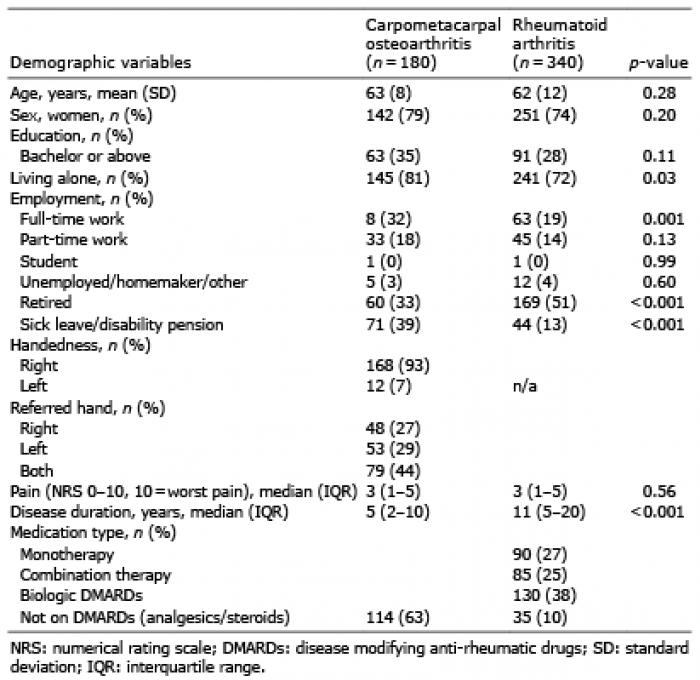
Demographic variables are shown in Table I. The RA sample contained significantly more people who were retired (p < 0.001) and had longer disease duration (p < 0.001), while the CMC1 OA sample had more participants working full-time (p = 0.001) and on sick leave (p < 0.001). People with CMC1 OA also reported to be living alone more often than people with RA (p = 0.03).
Table I Demographic variables for people with carpometacarpal osteoarthritis and rheumatoid arthritis
Construct validity (Rasch analyses) of the MAP-Hand in people with carpometacarpal joint osteoarthritis (n = 180)
A χ2 of 60.4 (df = 36, p = 0.007) indicated that there was no misfit between data and the model. The person and item fit residuals showed no serious misfit among items or persons (item fit residual mean 0.13 (SD 1.08); person fit residual mean –0.17 (SD 1.17)). However, the mean person location showed some mis-targeting of the data. The scale and persons were off target as the people with CMC1 OA were more able (i.e. had less difficulty with items) than the mean of the scale (person mean –2.21 (SD 1.39)).
Nine participants data were misfitted (item person residual > 2.5). All items had ordered thresholds. However, for items: 1 (buttoning buttons); 2 (putting on socks); 10 (slicing bread); and 12 (stirring food), there were very few people ticking off the “unable to do”-option. We only found uniform DIF for sex in item 1 (buttoning buttons, p = 0.0007), with women scoring worse than men. No DIFs were found for age groups. The Residual Principal Components analysis supported the unidimensional structure of the MAP-Hand in people with CMC1 OA (p = 0.073). Clusters of local dependency could be observed, where we defined 3 clusters; cluster 1: buttons, socks, laces (items 1, 2, 3); cluster 2: opening screw tops, cans and jam jars (items 7, 8 and 9); cluster 3: carrying bags, pushing, carrying heavy (items 14, 17 and 18).
Grouping items with local dependency did not improve the overall fit to the model and worsened the mis-targeting of the data and therefore was not performed. When removing misfitted persons, rescoring items 1, 2, 10 and 12 by collapsing response categories 3 (“great difficulty”) and 4 (“unable to do”), and splitting item 1 (buttoning buttons) for DIF (sex), the scale and persons were less off target with a mean person location of 1.33 (SD 1.34). The overall fit to the model remained almost the same; χ2 = 53.0 (DF 38, p = 0.046); item fit residual mean = 0.15 (SD 1.09); person fit residual mean = –0.11 (SD 1.03), indicating no misfit to the Rasch model.
Differences in activity limitation between people with carpometacarpal joint osteoarthritis and rheumatoid arthritis (n = 520)
There was no significant difference in total mean MAP-Hand score between people with CMC1 OA and RA (mean 1.97 (SD 0.42) vs mean 1.98 (SD 0.65), p = 0.95) (Fig. 1). When assessing DIF of the different items of MAP-Hand using condition as a person factor, it was found that people with CMC1 OA had more problems with items 4 (squeezing out of tubes), 9 (opening jam jars), 12 (stirring food in a pan) and 13 (wringing out clothes), while people with RA had more problems with items 14 (carrying shopping bags), 17 (pushing with hands), and 18 (carrying heavy objects) (Fig. 2).
Fig. 1. Box plots showing mean activity limitations (MAP-Hand mean score; 1 = no activity limitations, 4 = unable to perform activity) in people with carpometacarpal osteoarthritis vs rheumatoid arthritis.
Fig. 2. Differential item functioning (DIF) between people with carpometacarpal osteoarthritis (n = 180) or rheumatoid arthritis (n = 340) with Bonferroni correction (p-value of < 0.002), shown for items in the Measure of Activity Performance of the Hand (MAP-Hand) questionnaire. The percentages of people scoring in the different response categories are shown in light grey (rheumatoid arthritis) and blue (carpometacarpal osteoarthritis)
The aims of this paper were to assess if the scores of the MAP-Hand questionnaire satisfied the Rasch model requirements with regard to construct validity in people with CMC1 OA and to explore the differences in activity performance of the hand between people with RA and CMC1 OA. The results of the Rasch analyses showed that the MAP-Hand had acceptable construct validity in people with HOA. There was no difference between people with CMC1 OA and RA with regard to the total mean score of the MAP-Hand. However, there were some differences at item levels with people with RA having more problems with carrying and pushing items, while people with CMC1 OA had more problems related to fine hand use (squeezing) and twisting/turning (stirring, opening jars and wringing clothes).
Construct validity (Rasch analyses) of the MAP-Hand in people with carpometacarpal joint osteoarthritis
In line with previous findings in people with RA (13), the MAP-Hand questionnaire showed an overall fit to the Rasch model in people with CMC1 OA. The overall fit to the model did not alter on removing misfitted persons, splitting for DIF or rescoring items, highlighting that the questionnaire can be used in its current form. The unidimensional nature of the questionnaire displayed in both people with RA (13) and CMC1 OA indicates that the total mean score can be calculated and that comparisons can be made across different conditions.
Although the overall fit to the model was good, a mis-targeting of scores was displayed, indicating that the questionnaire may have a ceiling effect in people with CMC1 OA. This finding was underlined by less mis-targeting of scores when collapsing the 2 worst response categories (“great difficulty” and “unable to do”) in 4 of the items. However, this ceiling effect may be related to the characteristics of the current CMC1 OA sample, and not a general ceiling effect in people with HOA. The NRS pain score in the current sample indicated that the participants had mild pain and activity limitations were considered to be moderate. Thus, rather than altering the scoring of the questionnaire, additional testing of the construct validity of the MAP-Hand scores in a more affected HOA sample is recommended.
The MAP-Hand questionnaire is based on patients’ own views of their activity problems, and includes a variety of handgrips (13). We found some dependency between handling buttons, socks, laces, between opening screw tops, cans and jam jars, and between pushing and carrying items. However, grouping these items did not improve the overall model fit, and worsened mis-targeting of data. Based on these results, we do not recommend any alteration of the instrument. Keeping the original items will give insight into all the different handgrips, allow comparison of activity limitations across different conditions and enhance its applicability in clinical practice.
Differences in activity limitations between people with carpometacarpal joint osteoarthritis and rheumatoid arthritis
A systematic review has concluded that people with OA entails a disease burden that is comparable to people with RA regarding pain and function (4). In line with the results of a previous study (8), we found that self-reported activity limitations were comparable in the 2 conditions. However, even though no significant difference was found in the total mean MAP-Hand score between people with CMC1 OA and RA, we found several differences at item levels. According to the International Classification of Functioning, Disability and Health (ICF) framework, people with CMC1 OA had more problems with fine hand use and twisting and turning activities, while people with RA had more problems related to carrying and pushing items. The results may have been influenced by the difference in disease duration between the 2 samples. However, these results may also be an indication of the difference in joint manifestation between the 2 conditions, with people with HOA showing more distal involvement, while people with RA have more proximal involvement (1, 5). This highlights that activity limitations should not only be assessed and reported by mean scores, but also by scrutinizing activity limitations at an item level.
Study limitations
There are some limitations to this study. The CMC1 OA and RA samples were collected from different countries, with differences in education and welfare systems. This made it somewhat difficult to compare the 2 samples. Also, the MAP-Hand questionnaire was administered in different languages in the 2 countries. However, as the questionnaire has been cross-culturally adapted and validated in both countries, the results should be comparable. In the present study, 78% of patients with CMC1 OA reported pain from other joints of the hand, supporting that they may be representative of people with HOA in general. Although the MAP-Hand seems to have sufficient measurement properties both in HOA and RA, the responsiveness of the questionnaire needs to be further investigated. In addition, as the questionnaire was developed for patients with RA, it may be that other activities than the current set should have been included for patients with HOA. In clinical practice, the questionnaire should also be accompanied by measurement of other aspects, such as pain, which is not included in the MAP-Hand.
Conclusion
The MAP-Hand questionnaire satisfies the Rasch model requirements regarding construct validity and can be used to evaluate activity limitations in people with CMC1 OA. An overall difference in activity limitations between people with CMC1 OA and RA was not found. However, people with CMC1 OA report more problems with fine hand use and twisting and turning activities, while people with RA report more problems related to carrying and pushing.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize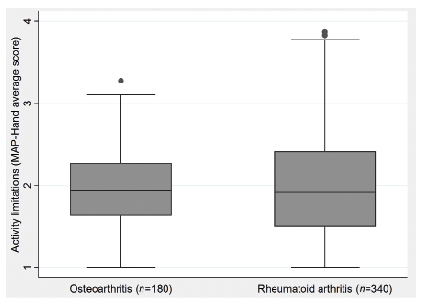 Click to show fullsize
Click to show fullsize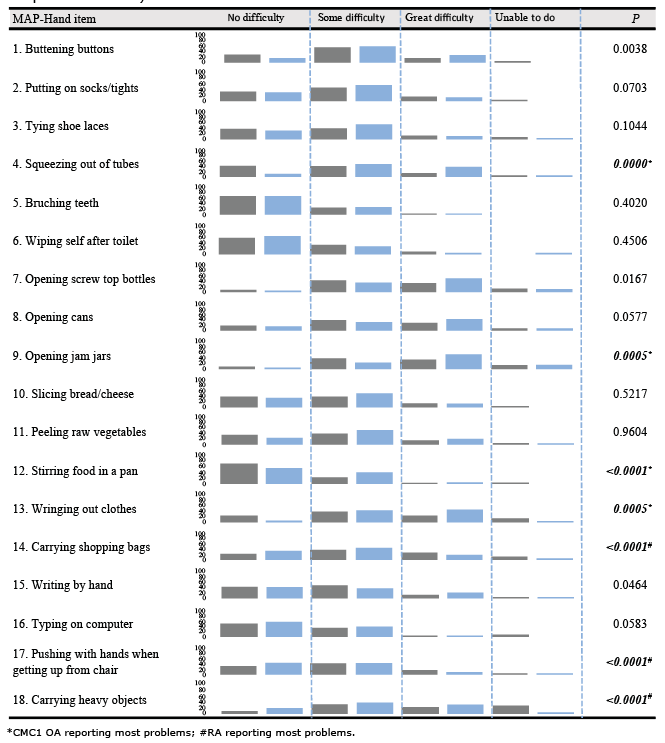 Click to show fullsize
Click to show fullsize