
From the 1Department of Psychosomatic Medicine and Psychotherapy, University Medical Center of the Johannes Gutenberg University Mainz, and 2Department of Orthopaedics and Traumatology, University Medical Center of the Johannes Gutenberg University Mainz, Mainz, Germany
Objective: To examine the psychological, social, behavioural and injury-related factors impacting functional outcome in patients with ankle or lower limb fracture one year post-operation.
Methods: In this prospective study 66 patients with ankle or lower leg fracture were recruited and followed up one year post-operation. Possible associations between predictors and functional outcome were explored by regression analyses. Functional outcome was assessed with the American Orthopedic Foot and Ankle Society Ankle-Hindfoot Score.
Results: Linear regression models revealed that smoking and elevated symptoms of adjustment disorder were associated with lower functional outcome one year post-operation. Fracture type, depressive symptoms and quality of relationship had no effect on functional outcome. A second linear regression revealed that preoccupations were correlated with functional outcome.
Conclusion: Smoking and symptoms of adjustment disorder, specifically preoccupations, are associated with functional outcome one year post-operation in patients recovering from ankle or lower leg fractures. The results support the notion that differences in functional recovery are attributable to psychological and behavioural factors rather than to fracture type. Psychological, fracture-specific, symptoms play a role in functional recovery rather than general affective symptoms.
Key words: ankle fractures; functional outcome; recovery of function; rehabilitation; adjustment; psychosocial factors.
Accepted May 20, 2020; Epub ahead of print Jun 4, 2020
J Rehabil Med 2020; 52: jrm00086
Correspondence address: Sabine Weimert, Universitätsmedizin Mainz, Klinik und Poliklinik für Psychosomatische Medizin und Psychotherapie, Untere Zahlbacher Str. 8, 55131 Mainz, Germany. E-mail: sweimert@students.uni-mainz.de
After ankle and lower leg fractures, some patients remain impaired for up to one year. Psychosocial factors are known to influence recovery after orthopaedic trauma. This long-term study examined how psychosocial, behavioural and injury-related factors are associated with functional outcome one year after injury. The results show that patients who smoke at 4 weeks after the fracture and have increased symptoms of adjustment disorder have a poorer outcome one year after injury. Fracture type, social support in the relationship and depressive symptoms are not associated with outcome one year after the fracture.
Lower leg and ankle fractures remain one of the most common injuries treated by orthopaedic surgeons (1, 2). Studies suggest that long-term impairments persist up to 3 years after ankle fractures, including pain, stiffness, impaired activity level and function (3–5).
Smoking and injury characteristics are biological factors associated with poor outcomes of operatively treated ankle or lower leg fractures. Smoking is associated with more complications (6) and lower physical functioning up to 3 months after surgical treatment (5). Weber C fractures are associated with poorer functional outcomes than less disruptive Weber A fractures (7).
Psychosocial factors may account for a large proportion of the variance in functioning in orthopaedic conditions (8, 9) and after orthopaedic trauma (10), e.g. relationship conditions (11). Perceived social support in relationships is crucial concerning health outcome after injury (12, 13). Patients with ankle fractures commonly report psychological distress (14). Among patients with lower limb fractures, 32–41% experience depression and notably, depressive symptoms are associated with poorer functional outcome (15, 16). Nota et al. found that depressive symptoms shortly after orthopaedic trauma were correlated with disability 5–8 months after trauma (9). When patients struggle to adapt to these changed circumstances it can result in psychological disorders, such as adjustment disorder (AD). Conceptually, AD is an intermediate health condition between normal responses to stress and more severe psychological disorders, such as anxiety and depression (17). AD overlaps with anxiety and depression, but comprises heterogeneous symptoms, such as rumination, disorders of social behaviour or irritability. To our knowledge there is no prospective study investigating the role of symptoms of AD in the context of fractures, despite the fact that AD is one of the most common used psychological diagnoses in psychiatry (18) and in the medical context (19–21). Comprehensive follow-up of symptoms of this frequent psychological disorder are necessary after ankle and lower leg fractures.
The aims of this prospective observational study were: (i) to determine the impact of biological (fracture type, smoking), social (social support from partner) and psychological variables (symptoms of depression and AD) at 4 weeks post-operation on functional outcome one year post-operation, after accounting for baseline functional outcome and age; and, since it was assumed that symptoms of AD would co-vary with long-term functional outcome; and (ii) to explore which symptoms of AD are specifically related to functional outcome one year post-operation.
Sample and recruitment
Under an institutional review board-approved protocol, patients who sustained a fracture of the ankle or the lower leg and who were treated at the University Hospital of a large public university in Germany between 1 December 2014 and 31 April 2016 were assessed for eligibility.
Inclusion criteria were: (i) age 18 years or older; (ii) fracture of the lower leg (AO 41-A, 41-C, 42-A, 42-B, 42-C, 43-A, 43-B, 43-C) or the ankle (AO 44-A, 44-B, 44-C) that required surgery; (iii) sufficient command of the German language; and (iv) Injury Severity Score (ISS) lower than 16 on admission.
Exclusion criteria were: (i) malignant disease; (ii) pathological fractures (e.g. caused through osteoporosis); (iii) psychosis, or active alcohol or substance dependence; (iv) cognitive deficiency or other factors that could interfere with informed consent processes; (v) pregnancy or breastfeeding. Some fractures, such as uncomplicated ankle fracture, might be treated with conservative treatments, but for better comparability, the study included only those patients who were treated operatively. Patients who sustained an AO type 41 B fracture were not included, since they were already included concurrently in another study at the same clinic. Eligible patients were approached shortly after their operation. Patients who agreed to participate completed a questionnaire measuring symptoms of AD, mechanism of injury and pre-existing psychological disorders at enrollment (Baseline). Since the study focuses on functional outcome, the patients for whom the data on functional outcome were available at both 4 weeks post-operation and at follow-up, formed the study cohort (Table I). There were no significant differences in age, sex, symptoms of AD or fracture type between patients with and without complete follow-up data. A flow diagram of the patients who completed both assessments of functional outcome is presented in Fig. 1. The patients were recruited, on average, 2 days after the operation.
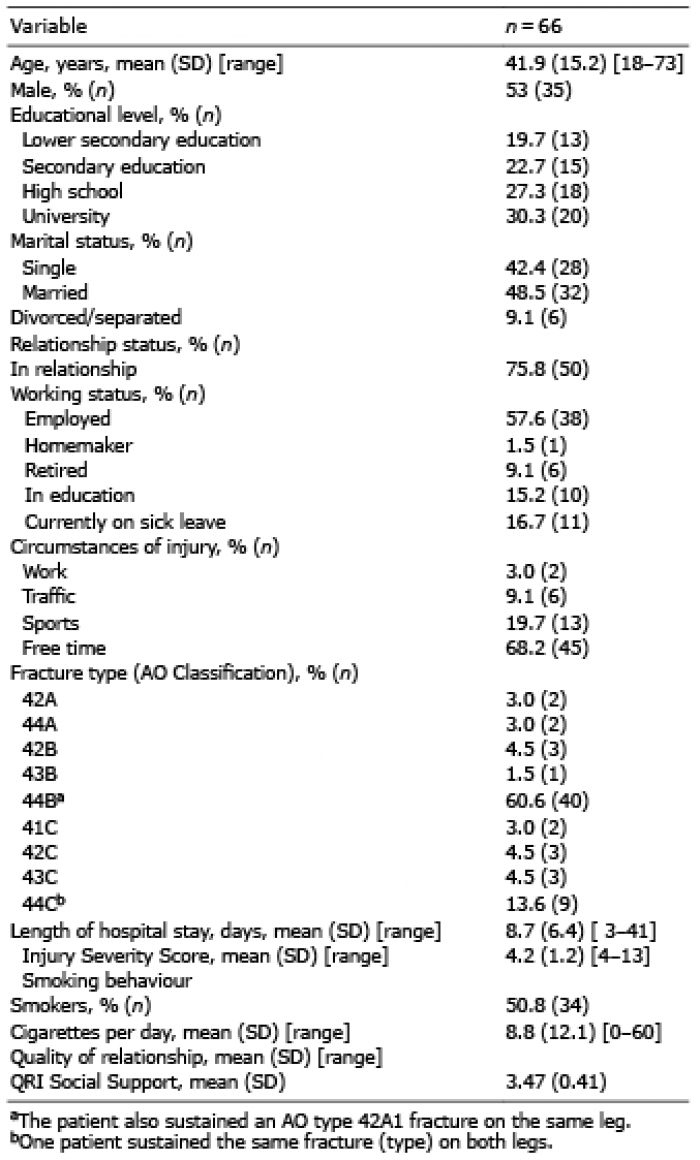
Table I. Demographic variables and baseline characteristics of the study cohort
Fig. 1. Flowchart of patients who completed both assessments of functional outcome (American Orthopedic Foot and Ankle Society; AOFAS).
At 4 weeks post-operation, patients were physically examined by an intensively trained and experienced medical student to assess functional outcome, and interviewed by a psychologist to assess psychological disorders. This was done as an outpatient assessment. If the patient had not been discharged by 4 weeks post-operation, the examination and interview was performed in the patient’s hospital room. Physical examination included the measurement of flexion and extension angles and the circumference of the knee joint gap, ankle and lower leg. In addition, a standardized procedure for the measurement of functional outcome was performed. At 4 weeks post-operation, patients also completed a set of questionnaires that contained demographic questions, questions on smoking behaviour and validated measures of symptoms of AD, depressive symptoms and relationship quality. Six months post-operation patients completed a set of questionnaires on the symptoms of AD and depression. A follow-up assessment was conducted one year post-operation: patients underwent physical examination and completed questionnaires on symptoms of AD and depression. Mechanism of injury, fracture type and ISS were abstracted from the medical record.
The time frame of 4 weeks was based on our experience that recovery (e.g. taking little or no pain medication, bearing weight) is not yet established by this time. After that time we expected the onset of symptoms of AD, since patients left the hospital, where they experienced full-time care, and had to manage everyday life in their regular environment. In contrast, by one year post-operation recovery is well established in most patients. Since this study is observational, patients who were diagnosed with AD were provided with information about treatment options.
The study was approved by the ethics committee of the State Board of Physicians of Rhineland-Palatinate (Germany). All participants provided written informed consent to participate in this study.
Measurements
Fracture type. To characterize the fracture type, X-ray or computed tomography (CT) images of the fractures were reviewed and classified according to the Mueller AO Classification by an orthopaedic surgeon (22). For further analysis fractures were categorized according to the sub-classification, resulting in 3 groups: AO type A, B and C.
Functional outcome. Functional outcome was measured with the American Orthopedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Score (23). The AOFAS Score is among the most commonly used instruments for measuring treatment outcome in patients who have sustained an ankle or hindfoot injury. It comprises a patient-reported part concerning pain and function and an objective part based on the clinicians’ physical examination of the patient (e.g. assessing sagittal motion, ankle-hindfoot stability). The scale includes 9 items that can be divided into 3 subscales: pain (ranging from 0–40), function (ranging from 0–50) and alignment (ranging from 0–10). The sum score can range from 0 to 100. Higher scores indicate no impairments. A sum score of 90 or above is considered “excellent”, scores of 80 to 89 “good”, 60 to 79 “fair” and lower scores are considered as “poor” (23). The validity of the AOFAS Score and the reliability of the patient-reported part have been confirmed (24, 25). The reliability of the objective part has not yet been confirmed.
Symptoms of an adjustment disorder
Symptoms of an AD were measured with the Adjustment Disorder New Module (ADNM) (26). The self-administered questionnaire consists of 29 items, which ask about the frequency of symptoms that the patients experienced on a scale ranging from 0 to 3. The ADNM was adjusted so that all items referred to the accident that caused the fracture. The sum score can range from 29 to 116, with high scores indicating more symptoms of AD. Six subscales can be evaluated: intrusions, avoidance, failure to adapt, anxiety, depression and disorders of impulse control. The scales are not standardized. After the ADNM was conceptualized, the model of AD on which it is based on, as well as the ADNM itself, has been further developed. The symptom cluster, which was called “intrusions” has been developed to “preoccupations” (27). The current terminology is therefore adopted. Reliability and validity have been confirmed (28). The internal consistency of the sum score was high (Cronbach’s α 0.95) in the current sample.
Depressive symptoms. Depressive symptoms were measured with the German Version of the Patient Health Questionnaire – 9 (PHQ-9) (29). The self-administered questionnaire consists of 9 items regarding the frequency of depressive symptoms. Items are scored from 0 to 3, with a maximum score of 27. A score of 10 or above is frequently used as a cut-off point to identify patients with major depression. The PHQ-9 has been proven to be a reliable and valid measure of depressive symptoms (30). The internal consistency of this was satisfactory (Cronbach’s α 0.76) in the current sample. One patient did not provide information on depressive symptoms.
Psychological disorders. To assess psychological disorders and history of mental illness the German Version of the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders was conducted (SCID-I and SCID-II) (31).
Social support. The Quality of Relationships Inventory (QRI) (32) is a self-administered questionnaire that consists of 25 items, scored from 1 to 4. The QRI is divided into 3 scales: Social Support, Conflict and Depth. The QRI has been shown to be reliable and valid (32). The internal consistency of the Social Support Scale was satisfactory (Cronbach’s α 0.77) in the current sample.
Fifty patients completed the QRI, 16 patients were not currently in a relationship. Only the social support scale was used for further analysis.
Smoking behaviour. Information on smoking behaviour and history was determined by the following questions: (i) “Do you smoke?” (ii) “If yes: I’ve been smoking since ... years” (iii) “How many cigarettes per day do you smoke?”. One patient did not provide information about smoking behaviour. The number of cigarettes smoked per day was included in the regression analysis.
Statistical analysis
Descriptive statistics were used to describe both demographic and primary study variables. χ2 tests, a Mann–Whitney U test and analyses of variance (ANOVAs) were used to compare drop-outs with those who completed the follow-up in terms of demographic data, fracture type and ADNM scores. Measures of functional outcome, quality of relationship, and symptoms of AD and depression were treated as continuous scales. Pearson’s correlation coefficients were computed to indicate the strength and direction of relationship between the 2 variables. Fracture type was treated as an ordinal scale and Spearman’s rho was calculated to indicate the strength and direction of relationships between fracture type and other variables. Changes in ADNM scores over time were evaluated with repeated measures analysis of variance (rmANOVA). As the data violated the assumption of sphericity, the Greenhouse-Geisser correction was applied. Change in AOFAS scores over time were evaluated with a t-test for paired samples. In order to determine the association between history of mental illness and ADNM, a Welch’s test was performed, since variance homogeneity between groups was not given.
Multiple regression analysis was conducted to determine factors linked to the functional outcome at one year post-operation, with the AOFAS sum score serving as dependent variable. The model was controlled for AOFAS sum score at 4 weeks post-operation. Age, the number of smoked cigarettes per day and fracture type, ADNM sum score, PHQ-9 score and QRI Social Support scale were entered as independent variables. To control for multicollinearity in the model, variance inflation factors were determined for the independent variables and had to be below 10.
To determine which symptoms of AD contribute to functional outcome, a linear regression analysis was conducted with the ADNM subscales serving as independent variables. A p-value < 0.05 was considered significant. Data were analysed using IBM SPSS Statistics 23.
Demographic variables and baseline characteristics
Patients were in mean 41.9 years old (standard deviation (SD) = 15.2; range: 18–73 years) and 53% (n = 35) were male. Demographic information and baseline characteristics are summarized in Table I. The majority (60.6%) of the cohort sustained a type-44B fracture (Table I). Three patients (4.5%) had an open fracture. The majority of the cohort (97.0%) had an ISS of 4. The mean hospital stay was 8.7 days (Table I). Fifty-one percent of the patients were smokers. Compared with a representative German sample (32), the current sample had higher scores on the social support scale.
Psychological diagnoses
According to the SCID, 13 (12.1%) patients had a history of mental illness. Three patients (4.5%) met the diagnostic criteria of AD 4 weeks and one patient (2%) one year post-operation. Three patients (5%) had a recurrent depressive disorder. None of the patients met the criteria for post-traumatic stress disorder (PTSD).
Symptoms of AD and depression
The ADNM and PHQ-9 scores can be seen in Table II. The severity of the symptoms of an AD peak 4 weeks post-operation. Preoccupation is the most common symptom at all measurement times. Preoccupations are recurring memories and thoughts of the fracture (and the situation in which it was sustained), which occur unintentionally. There was no significant association between a history of mental illness and the ADNM sum score 4 weeks post-operation (t(14.55) = –1.05; p = 0.31).
Functional outcome
The mean AOFAS sum score and subscales all increased between over time (Table II). One year post-operation 47 patients (71.2%) had an excellent functional outcome. Three patients (4.5%) had a poor outcome.
Table II. Change in primary study variables over time (n = 66)
Multivariable analysis of research questions
Linear regression analysis was conducted in order to predict long-term functional outcome. The results are shown in Table III. The extent of symptoms of an AD (β = –0.43; p < 0.05) and cigarettes smoked per day (β = –0.28; p < 0.05), both at 4 weeks post-operation, were significant predictors in the final model (F (7, 41) = 3.59, p < 0.01, adjusted R2 = 0.27) for functional outcome one year post-operation. Variance inflation factors were all below 3. We conducted another regression analysis without the social support variable to include the 16 patients who were not currently in a relationship. Symptoms of AD and the number of cigarettes smoked per day remain-ed significant predictors. The results can be found in the supplemental material (Table SI1)
Table III. Regression model for predicting long-term functional outcome (n = 48)
Linear regression analysis was conducted in order to predict physical function one year post-operation serving as dependent and the subscales of the ADNM serving as independent variables. The results are shown in Table IV A significant effect was observed for the preoccupations scale only (β = –0.38; p < 0.05) in the regression model (F (6, 59) = 5.18; adjusted R2 = 0.28; p < 0.01).
Table IV. Regression model of Adjustment Disorder New Module (ADNM) subscales at time 1 on long-term functional outcome (n = 65)
The prevalence of AD was higher in patients who have sustained a fracture of the ankle or foot than in the general population, in which it is estimated to be 0.9% (33). There appears to be a higher risk of developing AD after a fracture. Compared with a representative German sample, the study cohort reported higher levels of depressive symptoms at all measurement points (34).
The current study identified 2 significant factors that were linked to reduced functional outcome one year post-operation: (i) smoking; and (ii) symptoms of AD. These findings support those of previous studies, showing that smoking is predictive of lower physical functioning after ankle fractures (5) and is associated with a variety of orthopaedic conditions and complications (35, 36). Impairing osteoblast function and hindering collagen synthesis are just 2 examples of the many processes of bone and wound healing on which smoking has an adverse effect (37).
Symptoms of AD were related to reduced long-term functional outcome, while the fracture type was not. In the current study the fracture type was associated only with short-term functional outcome. It is possible that a complex fracture delays functional recovery, but has no effect on the long-term outcome. The findings of the current study underline that psychological factors play a vital role in physical recovery after orthopaedic trauma (38, 39).
The results show that symptoms of AD have a substantial correlation with recovery one year after a fracture, even when they do not meet the diagnostic criteria for a psychological disorder. This does not appear to be related to categorical diagnoses, as shown by the results from the clinical interview, but rather to specific symptoms. The current results support the results of Wegener et al. (39), indicating that “even moderately elevated levels of affective distress may lead to poorer functional outcomes”. Remarkably, symptoms of AD correlated with functional outcome, while depressive symptoms did not. Preoccupation was the most common symptom of AD in the study cohort 4 weeks post-operation, and the sole psychological factor that had a significant effect on functional outcome. Preoccupations, which are a main characteristic of AD, are triggered by and refer to the fracture. Hence, a fracture-specific symptom, and not general affective or cognitive symptoms, was significantly related to functional recovery. The symptoms of AD and depression overlap, but AD has a trigger by definition, whereas depression has no clear cause and the symptoms are unspecific. These results highlight that mental preoccupation with the injury hinders good rehabilitation, and anre in agreement with previous studies, which have shown that cognitive occupation and coping (such as catastrophic thinking) play a significant role in recovery after orthopaedic trauma (9, 10).
Surprisingly, social support in the relationship had no effect on functional outcome. Previous research shows that a high number of social relationships, not exclusively romantic, is a protective factor in various health conditions (40), which is a possible explanation for this result.
This study should be interpreted in the light of its limitations. Although dropouts did not differ statistically from the patients who completed the study, there is a potential for systematic differences based on unmeasured characteristics. Caution should be exercised when generalizing results of this study to other trauma populations. In addition, other clinical factors of rehabilitation, such as readmissions and complications, were not taken into account. Due to the study design no causal conclusions can be drawn.
The current study supports approaching patients with ankle and lower leg fractures from a biopsychosocial perspective, and challenges the traditional biomedical model. Surgeons should be aware that psychological and behavioural factors impact treatment success even more than injury characteristics (41). Informing patients about the impact of smoking in the recovery process could lead to better functional outcomes. Given the findings of this study, which indicate that symptoms of AD are a risk for a poor functional recovery, it is vital to carefully assess patients who have sustained ankle or lower leg fractures and, if necessary, initiate psychological interventions. Surgeons would be well advised to screen for psychological distress early in the treatment process, especially as even subclinical levels of symptoms of AD are related to impaired functional recovery, as the current results indicate. To ensure optimal treatment, it is crucial to focus not only on the physical symptoms, but also on possible psychological symptoms.
Surgical techniques have become more successful, and it is now important to also improve other aspects of treatment, taking into account the complex processes of recovery.
This study is supported by the Graute-Oppermann Foundation.The authors would like to express special thanks to the project coordinators Julia Bechtluft-Sachs, Patricia Lutz, Caroline Neumann and Philipp Winter.
Funding sources. The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize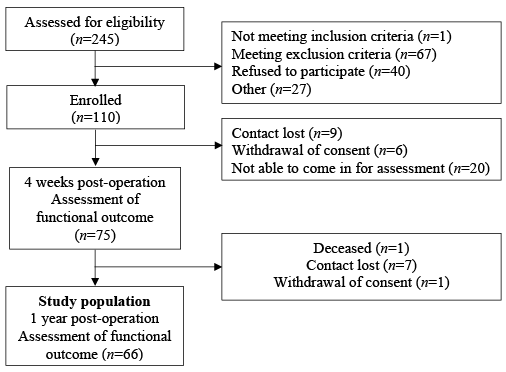 Click to show fullsize
Click to show fullsize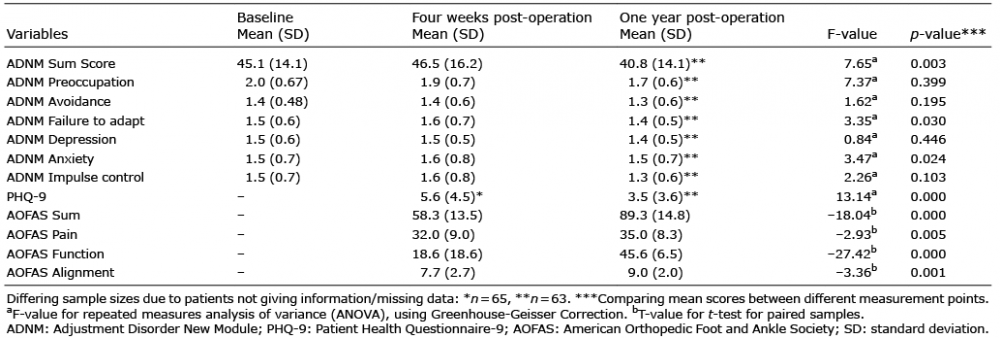 Click to show fullsize
Click to show fullsize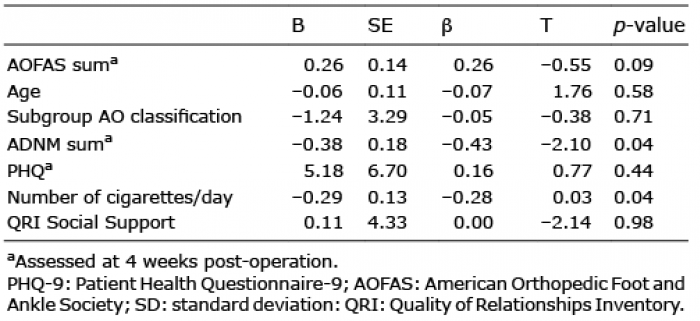 Click to show fullsize
Click to show fullsize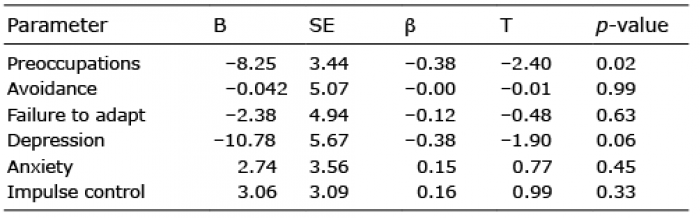 Click to show fullsize
Click to show fullsize