
From the 1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Rehabilitation Medicine, Sahlgrenska Academy, University of Gothenburg and Region Västra Götaland, Sahlgrenska University Hospital, Department of Occupational Therapy and Physiotherapy, 2Institute of Medicine, Department of Molecular and Clinical Medicine, Sahlgrenska Academy, University of Gothenburg and Region Västra Götaland, Sahlgrenska University Hospital, Department of Medicine, Geriatrics and Emergency Medicine, Gothenburg, Sweden
Objective: To determine the frequency of, and factors associated with, physical inactivity 6 months post-stroke.
Design: Prospective longitudinal cohort.
Patients: A total of 215 consecutively included individuals with mild acute stroke from the Fall Study of Gothenburg.
Methods: Physical activity level was assessed using the 4-level Saltin-Grimby Physical Activity Scale. Associations between independent variables and the dependent variable physical inactivity 6 months post-stroke were identified using univariable and multivariable logistic regression analyses.
Results: At 6 months post-stroke, 81 individuals (37.7%) reported physical inactivity. Physical inactivity at 6 months after a mild stroke were associated with: stroke severity, odds ratio (OR) 1.29 (95% confidence interval (95% CI) 1.01–1.66, p = 0.043); physical inactivity prior to stroke, OR 2.89 (95% CI 1.39–6.04, p = 0.0046); moderate postural control, OR 6.71 (95% CI 2.48–18.16, p = 0.0002); poor postural control, OR 2.55 (95% CI 1.19–5.48, p = 0.016); and number of drugs in acute stroke, OR 1.20 (95% CI 1.06–1.35, p = 0.0046).
Conclusion: In this exploratory study, almost 40% of subjects reported physical inactivity 6 months after an acute mild stroke. Predictors of physical inactivity were physical inactivity before stroke and greater stroke severity, impaired postural control and a higher number of drugs in acute stroke.
Key words: physical activity; stroke; rehabilitation; risk factors.
Accepted Jun 3, 2020; Epub ahead of print Jun 11, 2020
J Rehabil Med 2020; 52: jrm00077
Correspondence address: Carina U. Persson, Department of Clinical Neuroscience, Institute of Neuroscience and Physiology, Rehabilitation Medicine, Sahlgrenska Academy, University of Gothenburg, Per Dubbsgatan 14, 3rd Fl, Gothenburg, Sweden and Department of Physio-therapy, Region Västra Götaland, Sahlgrenska University Hospital/Östra, Gothenburg, Sweden. E-mail: carina.persson@neuro.gu.se
Physical activity has positive health benefits and can prevent the onset of stroke. Identification of individuals at risk for physical inactivity after stroke, during the first week after arrival at hospital, could have an important influence on preventive and rehabilitative actions. There are few previous studies on early prediction of physical inactivity, and these studies have a limited number of subjects. This study of 215 individuals aims to determine which factors prior to, and in the first week after, a mild stroke are associated with physical inactivity 6 months after stroke. The results show that physical inactivity before stroke and greater stroke severity, impaired balance and a higher number of drugs taken in the first week after stroke onset are associated with physical inactivity 6 months after stroke.
Physical activity, defined by the World Health Organization (WHO) as any bodily movement produced by skeletal muscles that requires energy expenditure, has significant health benefits (1, 2). Worldwide, insufficient physical activity is one of the leading risk factors for death (1). In addition, low levels of physical activity during leisure time is a determinant of ischaemic stroke (3). To prevent stroke, both primary (4) and secondary, (5) an accumulated physical activity level of at least 150 min per week of moderate intensity is included in the guidelines. However, many people who have experienced a stroke do not follow the guidelines of an accumulated level of at least 150 min a week of moderate-intensity physical activity (6, 7). Community-dwelling survivors of stroke take fewer steps and spend more time in a sedentary position than do healthy volunteers (8). Moreover, in high-functioning stroke survivors, physical activity has been shown to be generally low (9). In a recent study on 73 individuals at 12 months after stroke, a positive correlation was shown between strength, participation and stroke recovery, and self-reported physical activity level (10).
Factors positively associated with higher levels of physical activity are walking ability, balance and degree of physical fitness, based on a review of 26 studies of people living in the community after stroke (11). That review was restricted to generally small populations, where the majority of the participants were aged between 65 and 75 years, and were included late after stroke (a mean of 74.7 days), or with no inclusion time reported. In a more recent review and meta-analysis based on correlation analyses from 21 studies, age, sex, physical function, depression, fatigue, self-efficacy and quality of life were associated with post-stroke physical activity (12). Of these studies, the majority performed cross-sectional analyses, and only 7 studies investigated factors associated with physical activity as their primary aim (12).
The early prediction of modifiable risk factors could have an important impact on rehabilitation and intervention actions (as personalized rehabilitation plans and discharge planning), that can be taken early after stroke onset. However, there is a gap in the literature, since the early prediction of physical activity after stroke has been inadequately studied (13). One study, based on the early prediction of a low physical activity level one year after stroke, found that the determinants were older age, functional dependency and a previously low level of physical activity (13). This study was re-stricted to a sample size of 77 participants. The results from previous analyses needs to be confirmed in larger samples, as it is important to reduce uncertainty and increase confidence in estimates. Given these considerations, the aim of the current study was to determine factors prior to and in the acute phase after a mild stroke that are associated with physical inactivity 6 months after stroke. The acute phase refers to the first 7 days after stroke onset.
The current study is a prospective longitudinal cohort that forms part of the Fall Study of Gothenburg (FallsGOT) and has been presented in detail elsewhere (14–17). The sample size of 504 participants in the FallsGOT was based on power calculations made before the start of the study (14). The main study in the FallsGOT, conducted during a 21-month period of consecutive inclusion during 2014–2016 at 1 of 3 stroke units at Sahlgrenska University Hospital, aimed to identify the factors that predict falls after stroke.
The inclusion criteria were: patients aged 18 years or older, with a clinical diagnosis of first-ever or recurrent stroke. This sub-study had an additional inclusion criterion; it included only participants with mild stroke. Stroke severity was assessed by a trained nurse at the stroke unit using the National Institutes of Health Stroke Scale (NIHSS) (18). The NIHSS score ranges from 0 (no stroke symptoms) to 42 (very severe stroke). Mild stroke was defined in this study as an NIHSS score of 4 or less.
In addition to the former exclusion criteria (patients in a palliative condition, those unwilling to participate and those whose physicians regarded their inclusion as unethical), participants were also excluded if they were using a wheelchair at baseline.
The study was performed according to the Declaration of Helsinki (19). The reporting of the present study conforms with the STROBE guidelines (20). Ethical approval was obtained from the Swedish Ethical Review Authority in Gothenburg on 25 Feb 2014 (ref 004-14) and 9 Apr 2015 (ref T301-15, Ad 004-14). Prior to participation in the study, written and oral informed consent was received from all participants. The Fall Study of Gothenburg (FallsGOT) was registered at ClinicalTrials.gov (Identifier: NCT02264470).
The dependent variable was physical inactivity, the lowest category (score 1) in the Saltin-Grimby Physical Activity Level Scale (SGPALS) (21, 22). The SGPALS is an ordinal scale comprising 4 response categories, coded as: 1 = being physically inactive (i.e. being almost completely inactive, reading, watching television, watching movies, using computers or doing other sedentary activities during leisure time); 2 = some light physical activity (such as walking, riding a bicycle and light gardening for at least 4 h a week); 3 = regular moderate physical activity for a minimum of 3 h a week; and 4 = regular hard physical training for competition sports. SGPALS has been validated against maximal oxygen uptake (23) and for coronary risk factors (24) in population studies, and has been proposed to be a useful assessment tool in everyday healthcare (22). Dependent variable data were retrieved by sending the SGPALS to all participants who were still alive 6 months after stroke and asking them to mark one option out of the 4 response categories.
The independent variables were: age; sex; stroke severity (assessed using the NIHSS, 0 vs 1–4); physical activity level prior to the stroke (assessed using the SGPALS; dichotomized: 1 vs 2, 3 and 4); the Swedish version of the Postural Assessment Scale for Stroke Patients (SwePASS) (25–29); fear of falling (Are you afraid of falling? (yes/no)); self-perceived impaired postural control; tandem standing (item 13 on the Berg Balance Scale) (30), 5 categories, scale 0–4, here in the analyses converted to good ability (=reference value, consisting of response categories 3–4), moderate ability (based on response category 2) and poor ability (based on response categories 0–1)); risk-taking behaviour during tandem standing, cognition (assessed using the Montreal Cognitive Assessment Scale (MoCA) (31), number of drugs taken, orthostatic blood pressure (defined as a decrease of 20 mmHg systolic or 10 mmHg diastolic blood pressure after 1 min or 3 min standing), use of a walking aid, smoking habits and a history of diabetes mellitus, atrial fibrillation, congestive heart failure, ischaemic heart failure, previous stroke and/or previous transient ischaemic attack (TIA). The Oxfordshire Community Stroke Project system of stroke classification was used when subtyping the ischaemic stroke events (32). Independent variable data was retrieved from the participants’ medical records and based on baseline assessments. All the baseline assessments were performed standardized and according to clinical routine within the first 4 days after the admission to the stroke unit by the stroke unit’s team members. There were 2 exceptions related to timing. First, the data related to the number of drugs were based on the prescribed drugs that the nurse in the medical record had recorded administering to the patient on day 4 or on the day of a fall if the patient fell before day 4. Secondly, if cognitive dysfunction was suspected, the MoCA could be performed later during hospitalization. Details of the data collection have been published previously (14).
Data analysis
For categorical data, numbers and percentages were given. For continuous and ordinal variables, the median and interquartile range were specified. Associations between characteristics prior to and during the acute phase after a stroke and physical inactivity (i.e. SGPALS score 1) 6 months after mild stroke were identified using univariable logistic regression analyses. Variables that were significant in the univariate analyses were included in a stepwise multivariable logistic regression analysis. No adjustments for multiplicity testing have been made and the analyses made are explorative. The same set of independently significant variables in the multivariable model was selected when applying both stepwise forward selection and backward logistic regression. Due to some variables having missing data, manual stepwise regression was performed, excluding the not selected variables with smallest impact in the analysis and greatest number of missing data from the stepwise regressions. The Hosmer–Lemeshow test was used to test the goodness-of-fit of the multivariable logistic model. The odds ratio with a 95% CI, p-value and area under the receiver operating characteristic curve are presented. All statistical tests were 2-sided, and the level of significance was p < 0.05 for both entry and stay. The analyses were performed using SAS version 9.4 (SAS, Cary, NC, USA).
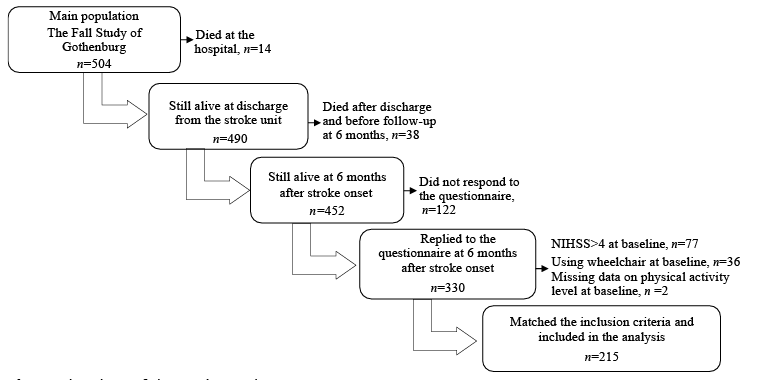
Fig. 1 shows the flow chart of the enrolment process. Table I details the baseline characteristics for the 215 patients who fulfilled the inclusion and exclusion criteria. Pre-stroke, almost 50% of patients reported physical inactivity. Almost one-third of those who were inactive pre-stroke, were physically active 6 months after stroke. Nearly 6 of 10 of the individuals who undertook light to moderate physical activity pre-stroke continued to be so 6 months after stroke. In addition, all of those who regularly spent time being physically active pre-stroke continued to do so at 6 months after stroke. At 6 months after stroke, 37.7% reported physical inactivity.
Fig. 1. Flowchart of the study enrolment process.
Table I. Baseline characteristics, assessments in the acute phase after stroke, length of stay and falls in hospital by all participants and by reported to be physically inactive or physically active at 6 months after stroke onset
Table II shows the results from the univariable and multivariable logistic regression analyses. Based on the univariable analyses, several of the independent variables were statistically significantly associated with low physical activity: age, stroke severity (NIHSS), physical activity level prior to the stroke, postural control (SwePASS), fear of falling, postural control (impaired ability to perform tandem standing), number of drugs taken, orthostatic blood pressure, use of a walking aid, and diabetes mellitus. However, in the multivariable analysis, only stroke severity, being physically inactive prior to stroke onset, number of drugs taken, and impaired and moderate postural control/ability to perform tandem standing in the acute phase after stroke remained statistically significantly associated with being physically inactive 6 months after onset of mild stroke. The result of the Hosmer–Lemeshow test for goodness-of-fit was p = 0.60.
Table II. Univariable and multivariable logistic regression analyses for prediction of physical inactivity 6 months following stroke
In this exploratory observational cohort study, almost 4 in 10 individuals reported physical inactivity at a follow-up 6 months after a mild acute stroke. High severity of stroke, physical inactivity prior to the stroke, moderate and poor postural control (ability in tandem standing) and higher number of drugs taken in acute stroke were identified as determinants of physical inactivity 6 months after stroke. For the multivariable model, the area under the receiver operating characteristic curve is 0.81, which implies that the model has excellent accuracy as a diagnostic test (33).
The rationale for the selection of participants with a NIHSS score of 4 or less was the risk of bias caused by the fact that individuals with more severe stroke might become immobilized by the neurological symptoms caused by the stroke, such as paresis of a lower limb. For the same reason, individuals using a wheelchair at baseline were also excluded. We expected that immobilized individuals are at high risk of being physically inactive even if they want to be physically active. Therefore, we selected a study population with as limited stroke severity as possible.
However, in those who were defined having a mild stroke, stroke severity also matters, with a 29% increase in OR for physical inactivity per each increase in NIHSS score.
The reported proportion of physical inactivity at 6 months after a mild stroke is higher than the proportion reported by the WHO (25% of adults worldwide not being active enough) (1), but also lower than the proportion reported prior to the stroke. Based on previous research (34), the low self-reported physical activity level after stroke was expected. The increased self-reported physical activity level from prior to the stroke to 6 months after stroke, is in line with previous research (34), which showed an increased self-reported physical activity level between 3 and 6 months after stroke. The increased proportion of patients who reported being physically active after the stroke compared with prior to the stroke may have been affected by the stroke onset itself, which may have prompted an increase in the patients’ motivation for a lifestyle change. Training with, and support from, physical therapists and other health professionals during the rehabilitation that followed the stroke may also have affected the level of physical activity at 6 months. The use of supported discharge, physiotherapist support, or physical activity on prescription were not registered, but, in further research, it would be interesting to identify its impact on physical activity level.
Previous research (35) that shows that the majority of studies assessing physical activity via self-reports instead of direct measurements may overestimate the actual physical activity levels. Thus, the proportion of physical inactivity after stroke may be higher than reported. As physical inactivity prior to stroke constitutes a potential modifiable risk factor for physical inactivity after stroke, it should receive more attention. In a review of reviews, the findings with generally curvilinear relationships between physical activity and health outcomes emphasize that health benefits can be accumulated by simply becoming more physically active (2). Previous research has also shown that low physical activity level prior to the stroke associates with higher stroke severity (36). Consequently, the threshold-based message when relating to the international guidelines of 150 min/week of moderate-to-intense physical activity is challenged.
The association between pre-stroke and post-stroke physical activity levels is in line with previous findings (13, 37). The finding that impaired physical function is associated with post-stroke physical activity confirms previous studies among community-dwelling stroke survivors in a review based on correlation analyses (12) and on the early prediction of physical activity one year post-stroke (13). The fact that postural control (also expressed as balance) is associated with post-stroke physical activity level is in line with previous research (11, 34, 38).
To the best of our knowledge, no previous research has found any association between the number of drugs taken and physical inactivity 6 months after stroke. In spite of this, it is not far-fetched to believe that the number of drugs prescribed and administered to the patient in the acute phase after stroke is a proxy for co-morbidity, which can, in turn, (just like stroke severity), affect the conditions for performing physical activity. In the present study, sex was not shown to be associated with physical inactivity, which is in contrast to the results from the previous meta-analysis (12). The reason for these diverging results is unclear, and should not be explained by an uneven proportion of women and men included in the analyses. The fact that age was not associated with physical inactivity is also in contrast to previous research (13, 37). The reason for this difference is also unclear. In the current study, with participants with an age range of 41–104 years, there was no upper age restriction for inclusion. Fear of falling was associated with physical inactivity in the univariable analysis, but not in the multivariable analysis, as might have been suspected. This might have been due to a correlation between fear of falling and impaired postural control.
The current study has 5 major strengths. First, the population size is large compared with prior reports; secondly, the independent variables are representing several of the dimensions of the International Classification of Functioning and Health (39); thirdly, the design is prospective; fourthly, the follow-up time-point is recommended and well-defined (40) and, finally, the inclusion was consecutive.
The study should also be interpreted in the light of its limitations. One such limitation is missing data, mainly for MoCA and orthostatic blood pressure. Another limitation is that, at the time of inclusion, patients who were under consideration for/receiving thrombolysis or thrombectomy were not included, as they were admitted to another of the 3 stroke units at Sahlgrenska University Hospital, resulting in a risk of selection bias. In addition, the selection of mild stroke, also limits the generalization of results. That the SGPALS has not been specifically validated in patients with stroke is a limitation. Even though the use of the SGPALS, including one question, is both inexpensive and time efficient as part of the screening for those individuals most at risk, a further weakness is the risk of both recall and misclassification bias by using self-reported data on physical activity instead of direct measurements of physical activity. In addition to the risk of overvaluation already mentioned, the precision when recalling distant events may be affected. Despite the number of potential determinants of a sedentary lifestyle, other variables, which may be important, such as fatigue; depression; quality of life; metabolic adaptations to physical activity; genetic and motivational factors; social and caregiver support; other environmental factors; the individuals’ health literacy and information on physical activity on prescription and mobility, were not included. In addition, just over a quarter of those individuals who were eligible at the 6-month follow-up did not reply to the questionnaire, and based on the study design, the cause and effect remain uncertain.
For clinical practice in rehabilitation, knowledge of factors associated with a low physical activity level after stroke could guide the clinician at the stroke unit when offering and planning individualized rehabilitation interventions. Above all, this knowledge should be helpful before any stroke event occurs, in the physiotherapist’s motivational conversation (about living habits in general, and about physical activity and the prescription of physical activity more specifically) that begins during the hospital stay at the stroke unit. Further research into the attitude towards physical activity in the general population, the role of physical activity level prior to stroke onset for physical activity post-stroke, and, by partnership, identification of the meaningfulness of such prediction for individuals with stroke, their relatives and rehabilitation teams, is called for.
In conclusion, this exploratory study showed that almost 40% of those with a mild stroke reported physical inactivity 6 months after stroke. More likely to report physical inactivity were individuals who reported physical inactivity prior to the stroke and with greater stroke severity, impaired postural control and a higher number of drugs in acute stroke. For clinicians these results show that individuals at risk of physical inactivity after stroke can be identified in acute stroke using simple methods.
The authors thank all the participants and their relatives, all the team members at stroke unit 354 at Sahlgrenska University Hospital/Östra, Associate Professor Bodil Lernfelt, and statistician Aldina Pivodic at Statistiska Konsultgruppen for their contributions. The study was financed by grants from the Swedish state under the agreement between the Swedish government and the country councils, the ALF agreement (881811), and from the Swedish Neuro Fund.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize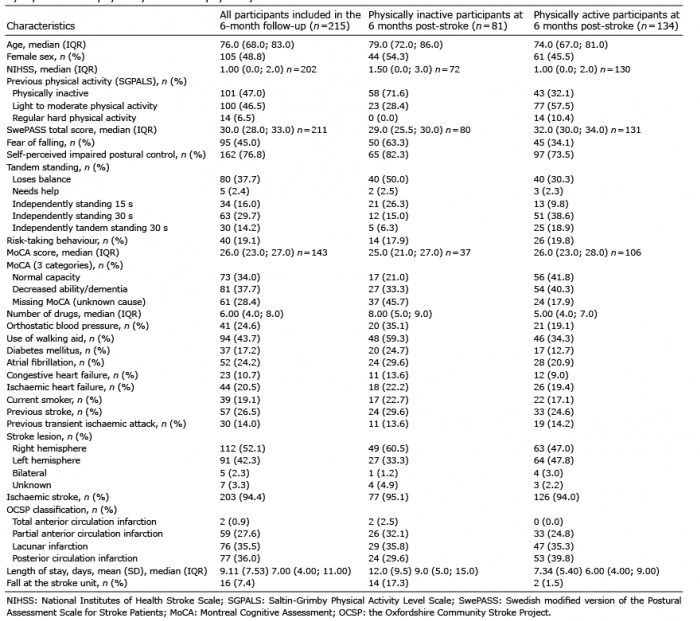 Click to show fullsize
Click to show fullsize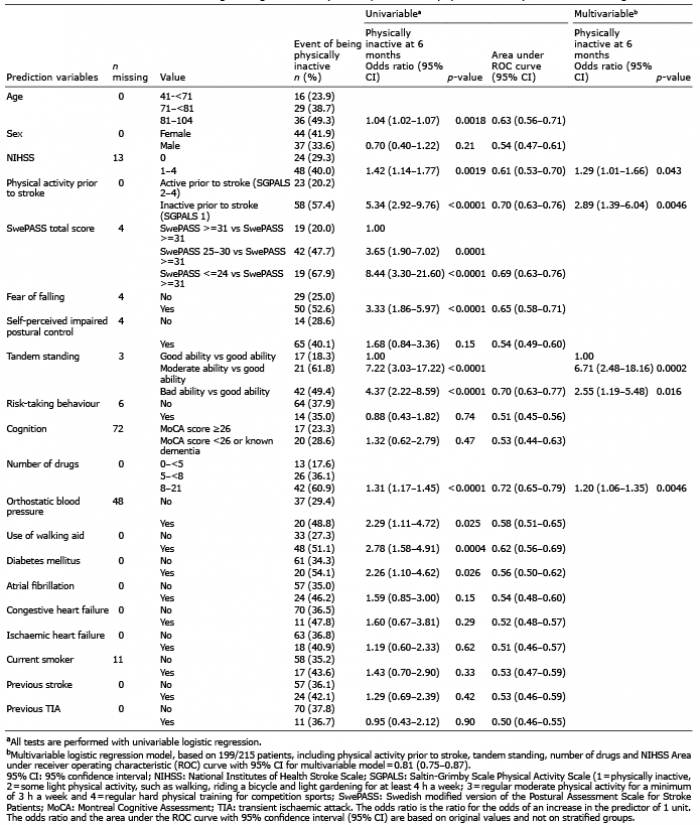 Click to show fullsize
Click to show fullsize