
From the 1Department of Rehabilitation, University Hospital of North Norway, Harstad, 2Faculty of Health Sciences, Department of Clinical Medicine, UiT – The Arctic University of Norway, 3Faculty of Health Sciences, Department of Psychology, UiT – The Arctic University of Norway, 4Department of Rehabilitation, University Hospital of North Norway, Tromsø, Norway, 5Faculty of Health Sciences, Department of Health and Care Sciences, UiT – The Arctic University of Norway, Tromsø, Norway, 6Hammel Neurorehabilitation Centre and University Research Clinic, Aarhus University, Aarhus, Denmark and 7Institute of Health and Society, Research Centre for Habilitation and Rehabilitation Model and Services (CHARM), Faculty of Medicine, University of Oslo, Oslo, Norway
Objectives: To investigate changes in health-related quality of life between 3- and 12-months post-stroke in a north Norwegian and a Danish region that organize their rehabilitation services differently, and to identify clinically relevant predictors of change.
Design: Prospective multicentre cohort study.
Subjects: In total, 304 patients with first-ever stroke (male sex 59%, mean age 68.7 years) participated from Norway (n = 170) and Denmark (n = 134).
Methods: The Quality of Life after Brain Injury-Overall Scale (QOLIBRI-OS) was administered twice to measure change in satisfaction with function and wellbeing.
Results: QOLIBRI-OS scores showed a small statistically significant difference in favour of Norway at 12 months post-stroke (p = 0.02; Cohen’s d = 0.26). Using a calculated minimal clinically important difference score of 12, 20% reported worse, 54% unchanged and 26% better QOLIBRI-OS scores between 3 and 12 months. Age below 65 years predicted a negative change (odds ratio (OR) 0.4, p = 0.007).
Conclusion: In this population with mild and moderate stroke, QOLIBRI-OS scores were slightly higher in the Norwegian region. Approximately 50% of participants experienced clinically important changes in satisfaction with functioning and wellbeing between 3 and 12 months post-stroke. Younger age predicted negative change. This result could indicate increased rehabilitation needs over time in young patients and should be investigated further.
Key words: stroke; HRQoL; QOLIBRI-OS; satisfaction; change.
Accepted Jun 23, 2020; Epub ahead of print Jul 30, 2020
J Rehabil Med 2020; 52: jrm00096
Correspondence address: Guri Heiberg, Department of Rehabilitation, University Hospital of North Norway, St. Olavs Gate 70, NO-9404 Harstad, Norway. E-mail: Guri.heiberg@unn.no, guriheiberg@icloud.com
This article compares experiences in satisfaction with functioning and wellbeing at 3 and 12 months between patients with stroke in a region in Denmark and a region in North Norway. Acute treatment of stroke in stroke units at hospitals is comparable in the 2 regions, but subsequent rehabilitation services differ. The Danish region had more organized municipality-based rehabilitation, while the North Norwegian region used more in-patient rehabilitation at specialized rehabilitation wards. In total, 170 patients from Norway and 134 from Denmark answered questionnaires about satisfaction with functioning and wellbeing at 3 and 12 months after stroke. At 3 months, patients reported comparable satisfaction, but after one year, the Norwegians were slightly more satisfied, especially with cognitive and emotional status. Change in satisfaction with functioning between 3 and 12 months was comparable between the 2 regions.
Stroke is the second leading cause of death and a major cause of disability (1). The concomitant physical, cognitive and psychosocial consequences post-stroke (2, 3) may affect daily life activities and participation in society (4). A valid approach to identify consequences may be using patient-reported outcomes (5) to assess health-related quality of life (HRQoL). The term HRQoL is adapted from the general concept of QoL by weighting subdimensions related to health more strongly (6).
Patient-reported stroke scales provide various multidimensional assessments, but few include aspects of patient satisfaction with functioning and future health expectations (7). The brief condition-specific 6-item Quality of Life after Brain Injury – Overall Scale (QOLIBRI-OS) has recently been validated in patients with stroke (8). Using QOLIBRI-OS at 3 and 12 months post-stroke provides the opportunity to examine changes in self-reported satisfaction with function and wellbeing between the subacute and early chronic phases following stroke. Identifying factors promoting positive and negative changes in satisfaction with function might be essential to improve subacute rehabilitation services (9).
The degree and direction of changes in satisfaction with life and function vary between studies. Generic measurements may show no change (10), an increase (11) or a decrease (12) in HRQoL. Both internal factors and external factors such as rehabilitation services contribute to satisfaction (13), but the relative importance in neighboring countries is unknown. A study (14) using the disease-specific Stroke Impact Scale at 3 and 12 months showed both clinically relevant improvements and declines across different domains. Bouffioulx et al.(15) used Satis-Stroke, a questionnaire developed to assess satisfaction with functioning. Significant improvements in satisfaction with activity and participation between the acute and post-acute phases overlapped with improvements in motor abilities, but there were no changes in satisfaction between the post-acute and chronic phases. A multi-centre study, including rehabilitation clinics in 7 countries, compared the concept life satisfaction after stroke using the generic instrument LiSat-11(10). Findings indicated that levels of satisfaction differed between clinics, while the longitudinal data during the first year indicated slightly improved satisfaction with mental health and life as a whole. However, no consistent predictors of change have been reported (10,14).
To reduce the burden of stroke, evidence-based medicine and rehabilitation are essential (16, 17). Acute treatment and rehabilitation in stroke units (16) are organized fairly similarly across Western Europe (18). However, the organization of subacute (19) rehabilitation services varies more substantially. In the Danish study region, multidisciplinary neuro-rehabilitation teams offer individualized and planned services to patients with stroke (20), whereas municipalities in northern Norway seldom provide multidisciplinary teams and seem to use inpatient rehabilitation to a larger extent (21, 22).
The study objectives were to: a) compare the QOLIBRI-OS scores between two country-regions with different organized subacute rehabilitation services, but comparable in terms of health service systems and cultural values, b) assess levels and rates of change following stroke, and c) identify any geographical, demographic, psychosocial or treatment-related factor that may be associated with any observed changes.
Design
This study was a prospective, international, multicentre cohort study of consecutive patients with first-ever stroke living in predefined geographic areas in northern Norway and central Denmark. Patients were included when they were treated in stroke units and registered in the national Norwegian or Danish stroke registries. Data were collected acutely and at 3 and 12 months post-stroke.
Study areas
Participants were recruited from 30 municipalities served by the University Hospital of North Norway (UNN) and from 2 municipalities served by the University Hospital of Aarhus located in the Central Region of Denmark.
The population sizes were fairly comparable, with 138,455 and 185,289 people in the Danish and Norwegian regions, respectively. The UNN study admission area was 23 times larger than the Danish study area. In Denmark, stroke patients are admitted to a single university hospital serving 1.3 million inhabitants. In northern Norway, acute stroke treatment is provided at 1 of 3 stroke units in 3 different hospitals located 300 km apart, serving 35,000–100,000 inhabitants. In both regions, > 90% of all patients with stroke are admitted to stroke units. In Denmark, patients are transferred earlier to specialized community-based care, while northern Norwegian patients seem to be offered in-hospital rehabilitation more frequent in the early subacute phase after stroke (20).
Inclusion and exclusion criteria
The inclusion period was from March 2014 until the end of December 2015. All patients fulfilled the inclusion criteria of the national stroke registries, defined clinically according to the World Health Organization’s definition of stroke as acute ischaemic or haemorrhagic stroke in patients aged 18 years or above (International Classification of Diseases – 10th edition (ICD-10) diagnosis I.63 and I.61, respectively). Patients with subarachnoid haemorrhage were not included, as these patients are not part of the Norwegian stroke registry. Patients with stroke due to malignancy or head trauma were excluded.
Patients who died within the first year post-stroke were excluded. In addition, proxy responders, namely, a relative who had completed a short questionnaire on behalf of a patient, were excluded. A smaller number of patients in Norway (n = 25) were not included due to severe comorbidity or a short expected remaining life-span.
Recruitment
Patients from the Norwegian region were recruited at the stroke units by direct contact, by telephone after discharge or by the hospital staff responsible for collecting and submitting consecutive data to the national Norwegian stroke registry. In Denmark, one of the authors (HHS) retrieved information from the Danish National Stroke Registry on patients with stroke living in the 2 defined municipalities. The patients received postal questionnaires and were subsequently informed by the same author about the study by telephone or letter. Those who responded to the posted questionnaires became consenting participants in the study.
Measurements acute, and at 3- and 12- months post-stroke
Acute. Norway and Denmark have mandatory national stroke registries that gather person-identifiable information about patients with acute stroke admitted to hospitals. Information on stroke subtypes, stroke severity, length of stay in stroke units (LOS), thrombolysis, age, sex and living conditions was collected from the national stroke registries. Demographic data are presented according to recommendations from the Stroke Recovery and Rehabilitation Roundtable (23).
Stroke severity was defined within 24 h after admission to the hospital. In Norway, the National Institute of Health Stroke Scale (NIHSS) was used to measure neurological impairment after stroke, while the Scandinavian Stroke Scale (SSS) (24) was used to report stroke severity in Denmark. We chose to use the SSS, as the data from the Danish National Stroke Registry (25) were more complete. The missing Norwegian NIHSS scores were retrospectively coded from medical records. Conversion of NIHSS to SSS scores was performed using an unadjusted mathematical model for interconversion (26). The SSS sum score is divided into 4 categories: 0–14 indicates very severe stroke, 15–29 severe stroke, 30–44 moderate stroke and 45–58 mild impairment post-stroke (24).
At 3 months. In Norway, the National Stroke Registry collected follow-up data 3 months after hospital admission from medical records or through a telephone interview with patients or relatives as proxy respondents. As Denmark has no regular follow-up stroke registrations, a telephone interview, with selected questions from the Norwegian follow-up registry, was performed at 3 months post-stroke to acquire similar data from both countries.
The information on the course of rehabilitation following stroke unit care was collected by telephone interview in both study regions. Based on this information, the first rehabilitation received was classified as in-patient, community-based or no rehabilitation given.
At 3- and 12-months post-stroke. The participants completed a postal questionnaire containing QOLIBRI-OS and the Hospital Anxiety and Depression Scale (HADS).
The QOLIBRI-OS (27) is a HRQoL measure of satisfaction with function and wellbeing specifically tailored to patients with brain conditions (27). The 6 items assess the degree of patients’ self-reported overall satisfaction with “Physical Condition”, “Cognition”, “Emotions”, “Ability to Perform Daily Activities”, “Personal and Social Life,” and “Current Situation and Future Prospects”. A Likert scale provides the following 5 response categories for each item: not at all (score 1), slightly satisfied (score 2), moderately satisfied (score 3), quite satisfied (score 4), and very satisfied (score 5) (27). Thus, the item score range is 1–5, and the total score range is 6–30. The total score is arithmetically converted to a scale score between 0 and 100, where 100 is the optimal score. The questionnaire is validated for traumatic brain injury (27), subarachnoid haemorrhage (28) and stroke (8). A previous psychometric analysis of the QOLIBRI-OS in the same stroke study population showed high internal consistency (Cronbach’s α = 0.93) (8).
The HADS is a widely used screening instrument for symptoms of anxiety (HADS-A) and depression (HADS-D). The scale range is 0–21 for both the anxiety and depression subscale. Scores of 8 or above in either subscale indicate a possible clinical condition of anxiety or depression (29).
Ethics
The Norwegian Ethical Committee Health Region North approved the study (2013/1472).
In Denmark, approval was obtained from the Danish Data Protections Agency (reference no. 1-16-02-363-14).
Statistical analysis
All statistical analyses were conducted using IBM SPSS 25. Descriptive data are presented as means and confidence intervals or percentages. A simple imputation of scale scores was used (mean replacement) when 1 or a maximum of 2 items was missing on the QOLIBRI-OS and HADS. Differences between continuous and categorical data were examined with independent or paired sample t-tests and χ2 tests, respectively. Severe deviations from normal distribution assumptions were examined visually using P-P plots. The LOS and the Danish SSS scores were non-normally distributed; thus, we examined differences between SSS categories with χ2 tests, and the median and interquartile range (IQR) are reported for LOS.
The included explanatory variables were based on the referred literature and discussions in the research group and were the following: country-region, age, sex, pre-stroke demographics (living alone, working, education, independence), SSS, stroke subtype, thrombolysis, LOS, HADS-A and HADS-D.
Minimal clinically important difference (MCID) scores were calculated with the standard error of measurement (SEM) formula, i.e. . The SEM indicates the minimum raw score change that reflects a true change beyond measurement error, thus avoiding interpretation of a change score below the SEM score as reflecting a true change when measurement error is actually the primary reason for the observed change. A difference of at least 1 SEM has been used to define the MCID (30), but we chose to use stricter criteria by multiplying it by Z = 1.96 to improve the confidence intervals. Thus, a calculated SEM of 6 yields an MCID of 12 scale scores for the total QOLIBRI-OS. Effect sizes were calculated with Cohen’s d. A value below 0.5 is regarded as small, 0.5–0.8 is considered medium, and greater than 0.8 is considered a large effect size (31).
A multiple linear regression analysis was conducted to examine predictors of change in QOLIBRI-OS sum scores as the outcome, defined as the QOLIBRI-OS score at 12 months minus the QOLIBRI-OS score at 3 months. We report unstandardized beta coefficients because the QOLIBRI-OS scale range of 0–100 is well-established (27). The explained variance of each block is reported as the adjusted R2. Multicollinearity was checked with the variance inflation (VIF) estimate with a cut-off of 10, and the residual scores were examined for normality and homoscedasticity.
Two additional logistic regression analyses were conducted to examine predictors of decline and improvement in QOLIBRI-OS scores based on the MCID scores (with “no change” as the reference). Using MCID, change was defined as reliably negative or positive if change in QOLIBRI-OS scale scores decreased or increased by a minimum of 12 scale scores, respectively. The results are presented as adjusted odds ratios (OR). Model fit was investigated with the Hosmer and Lemeshow test to assess the agreement between the observed and predicted outcomes of our models. The degree of pseudo-explained variance was reported according to Nagelkerke’s R2.
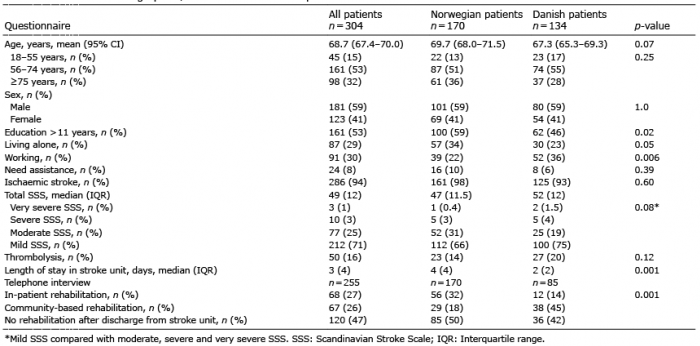
The descriptive data for the 2 cohorts are provided in Table I. A total of 304 patients with complete QOLIBRI-OS data at 3- and 12-months post-stroke were included as participants in the study; see the flowchart (Fig. 1) following the STROBE criteria.
Table I. Pre-stroke demographics, treatment and stroke-specific characteristics
Fig. 1. Flowchart of the study.
Dropout analysis
In total, 746 surviving persons with stroke (Norway, n = 423; Denmark, n = 323) were potentially eligible. Among them, 553 persons consented, but 249 of these persons were defined as non-participants as they did not complete the QOLIBRI-OS at both 3 and 12 months.
Analysis of representativeness was performed in 2 steps (Fig. 1). First, eligible persons not included from the Norwegian region because they did not consent (n = 73) were compared with the 170 Norwegian participants. Age did not differ significantly, but participants were more frequently men (63% vs 41%, respectively, p = 0.004). Second, the included participants from both countries (n = 304) were compared with non-participants (n = 249).
Non-participants in both countries needed more often help pre-stroke (p = 0.04), and had more severe strokes, with an SSS score of 45 (best score=58, standard deviation (SD) 12), while participants scored 48 (SD 11) (p = 0.003). The percentage of haemorrhagic stroke was higher among non-participants (14% vs 6%; p = 0.001). Age, sex and marital status were similar among participants and non-participants in both countries.
Demographics, stroke characteristics, mental health and treatment
The descriptive data for the 2 cohorts are presented in Table I. There were no significant differences between Norwegian and Danish participants in age, sex or stroke severity. However, the Norwegian participants tended to have more severe strokes. The country-regions differed significantly in terms of pre-stroke years of education and pre-stroke work status (Table I). An analysis of changes from the time of the event to 12 months post-stroke showed that the proportion of patients living in their own home without needing assistance decreased from 90% to 81% in the Norwegian region and from 94% to 83% in the Danish region. At 12 months post-stroke, 20% of northern Norwegian and 31% of Danish participants were employed. The number of those who had worked prior to the stroke decreased by 3% and 8%, respectively.
Data on in-hospital, community-based or no rehabilitation are presented in Table I. As indicated, the participants received more in-patient rehabilitation in northern Norway and more community-based rehabilitation in Denmark. The rehabilitation data must be interpreted with caution, as only 63% of the Danish population responded to this part of the survey, while all Norwegian participants answered these questions. Neither the HADS score at 3 and 12 months nor the HADS change scores differed significantly between the regions.
Country differences and changes in QOLIBRI-OS scores
Participants in both countries had a mean QOLIBRI-OS total score > 65 (maximum 100) (Table II).
Table II. Quality of Life after Brain Injury-Overall Scale (QOLIBRI-OS) items and scores at 3 and 12 months
The total QOLIBRI-OS score was not significantly different between the Norwegian and Danish regions at 3 months post-stroke (p = 0.08), but Norwegians had significantly higher scores at 12 months post-stroke (p = 0.02) (Table II and Fig. 2). The pre-existing country differences increased slightly, but the difference in the total QOLIBRI-OS score was small (Cohen’s d = 0.26).
Fig. 2. QOLIBRI-OS item and scale scores at 3 and 12 months in Norway and Denmark.
On the QOLIBRI-OS item score level, the effect sizes of the country differences were d = 0.41 for cognitive function, d = 0.28 for daily activity and d = 0.23 for emotions. The rate of change in the total QOLIBRI-OS scores from 3 to 12 months after stroke was not significant when examined separately in the country-regions (Fig. 2); thus, the rate of change between the country-regions was also not significant (p = 0.66).
Prediction of change in continuous QOLIBRI-OS scores
Linear regression analysis with the QOLIBRI-OS change score as the dependent variable revealed that all predictors were non-significant (Table III). The residuals were normal and homoscedastic, and the multicollinearity was negligible, as the VIF ranged between 1.0 and 1.7. Moreover, the test score reliability for the QOLIBRI-OS was excellent at both 3 and 12 months (0.92 and 0.93, respectively).
Table III. Unstandardized beta (β) coefficients for predictors of change in the Quality of Life after Brain Injury-Overall Scale (QOLIBRI-OS) score between 3 and 12 months according to the multiple regression analyses
As an alternative approach, minimal clinically important change scores were constructed. Using an MCID score of 12, patients were classified into 3 groups: no change (54%), worse (20%) and improved (26%). A logistic regression analysis with “no change” as the reference and the same predictors as those in the linear regression analysis indicated a sole predictor: age below 65 years predicted a negative change status (OR 0.4, p = 0.007) (Table IV). An MCID decline was observed among 29% of those below 65 years of age, compared with 16% for those above 65 years of age. Nagelkerke’s R2 was 0.12.
Table IV. Uni- and multivariate logistic prediction models with positive or negative change in health-related quality of life (HRQoL) as outcome (unchanged as reference)
No variables predicted a positive change. There were no significant differences between the country-regions in the worse, unchanged or improved clinical course distributions.
This study investigated satisfaction with functioning and wellbeing, as measured by the QOLIBRI-OS instrument, in 2 neighbouring country-regions that used similar acute treatment strategies, but organized sub-acute stroke rehabilitation services differently. At 12 months post-stroke, there was a slight difference in the QOLIBRI-OS score in favour of participants from the northern Norwegian region compared with participants from Denmark. Approximately half of the participants reported substantial clinical changes in the QOLIBRI-OS according to the MCID classification. Several predictors of MCID change were examined and it was found that age below 65 years was the sole predictor of risk of decline in satisfaction with functioning from 3 to 12 months post-stroke, whereas no predictors explained positive changes. These findings indicate that organization of subacute rehabilitation services had a minor impact on satisfaction with function and wellbeing in patients with mild and moderate strokes, as measured by QOLIBRI-OS. Patients below 65 years old were more likely to experience a decline in satisfaction, probably related to the loss of more complex activities and social roles or to higher expectations of functioning in general (22).
QOLIBRI-OS scores in the Norwegian and Danish regions
Comparable outcomes were found for the QOLIBRI-OS at 3 months post-stroke, as well as a clinically minor, but significant, difference between the country-regions in favour of the Norwegian Arctic Region at 12 months post-stroke. The dissimilarities were significant for items measuring cognition, emotions and activities of daily living. Cultural differences reflecting different expectations for health-related quality of life between the regions may play a role in explaining the slightly higher levels of satisfaction with functioning among Norwegians, although other studies did not find convincing signs of cultural influences that could explain the unequal life satisfaction (13).
Several other studies have compared HRQoL after stroke across countries. Ayis et al. (32) reported patient differences in HRQoL among 5 European populations that could not be explained by stroke severity or sociodemographic factors. Others (18) have found differences in patient-reported outcomes after stroke associated with how factors in stroke rehabilitation impose constraints that may cause disincentives for the rehabilitation process. In addition, Sprigg et al. (33) reported considerable differences in physical and emotional QoL (based on the Short Form-36) between regions and countries in Europe that persisted after adjusting for prognostic case mix and care quality variables. Langhammer et al. (13) found significant unexplained differences in life satisfaction when comparing rehabilitation units in 7 countries.
One reason for the small differences in HRQoL as revealed in our study may be that prior studies compared countries with more underlying differences in socioeconomic or healthcare systems than the Scandinavian countries. The health systems in Nordic countries are tax-financed, offering equal healthcare services to all inhabitants (34). Even though Norway has implemented the Coordination reform, advising early transfer of patients from hospital to community-based rehabilitation and care, northern Norwegian patients in this study seemed to be treated with in-hospital rehabilitation to a greater extent than the Danish patients. A likely reason may be that many smaller municipalities do not have the facilities or staff competence to offer subacute stroke rehabilitation. Regarding self-reported satisfaction with functioning and wellbeing as measured by QOLIBRI-OS, this study indicates that the organization of rehabilitation in Denmark, with its specialized multidisciplinary, community-based teams that reflect the principles of early supported discharge (ESD) (35), should be investigated further to assess effects compared with those of other subacute rehabilitation services.
Change in satisfaction with functioning and wellbeing from 3 to 12 months
The rate of change in QOLIBRI-OS scores from 3 to 12 months was not significant for either country or different between Norway and Denmark. A lack of change post-stroke coincides with other studies using change in self-perceived health-related functioning post-stroke as the outcome (4, 10). However, the degree of individual changes in wellbeing and satisfaction with functioning were substantial, as almost 50% of the patients reported a clinically significant change in the QOLIBRI-OS. This magnitude of clinically meaningful changes in either direction is in accordance with a study by Guidetti et al. (14) examining changes using the Stroke Impact Scale score during a similar follow-up period as that in the present study. The substantial degree of individual changes in wellbeing and satisfaction with functioning is interesting because it may involve long-term changes in rehabilitation needs. This finding indicates that patients should be followed for a longer period to identify vulnerable patient groups experiencing functional declines that may hamper their HRQoL.
Predictors of change in QOLIBRI-OS scores
Several predictors of MCID change were examined, such as country, demographic factors, stroke characteristics, LOS and psychological factors. Psychological factors contributed strongly to HRQoL (36), but they did not contribute to changes in the QOLIBRI-OS score in the present study, a finding that is in accordance with a study by Donnellan et al. (36). However, age below 65 years was the sole predictor of negative change, whereas no predictors explained positive change in QOLIBRI-OS scores.
White et al. (10) found positive change in HRQoL between 3 and 12 months among younger persons in a stroke cohort study. In contrast, we observed that younger patients were more susceptible to negative changes in HRQoL. Some of the younger patients may experience unfulfilled aspirations of returning to work after stroke, resulting in significantly decreased subjective wellbeing and life satisfaction (37). They may also experience more demands across several life areas compared with older patients, resulting in the observed increased risk of decline in wellbeing and satisfaction with functioning (38). Comparably, a systematic review (3) revealed a negative impact on family relationships, sexual life, economy and leisure activities among patients with stroke below 65 years old. Moreover, a Swedish twin study by Harris et al. (39) reported that genetic factors contributed more to perceived satisfaction with health among those older than 65 years of age, whereas the satisfaction of younger individuals with health was more strongly related to environmental factors.
Based on our findings, we recommend that rehabilitation services pay attention to younger patients with stroke, as they are more prone to perceiving a decline in satisfaction with functioning and health during the first year post-stroke.
Strengths and limitations
The observational design of this study allowed the tracking of patient satisfaction and functioning to be compared between these 2 country-regions. The number of participants in the present study was high compared with that in previous similar studies (4, 10). The recruitment process differed between the 2 countries, but every stroke survivor fulfilling the inclusion criteria in the predefined area and time period was asked to participate, apart from 25 Norwegian patients who had severe dementia or were terminally ill. It was not possible to exclude Danish patients at the beginning of the study, but it is not likely that Danish patients in an equivalent situation would have been able to participate in the study. The participants differed significantly only in education and proportion working.
The findings of this study may not be representative of populations with more severe stroke severity. Analyses revealed some selection biases, as non-participants more often had haemorrhagic strokes, severe strokes and needed help pre-stroke.
Retrospective coding of some Norwegian stroke severity data may represent a limitation, but studies have found adequate reliability of SSS data coded from medical journals (40).
Furthermore, the results from regional studies may not be representative of the national situation.
Conclusion
Minimal differences in patient-reported wellbeing and satisfaction with functioning measured with QOLIBRI-OS between the investigated regions in Arctic Norway and Central Denmark were found, despite different sub-acute rehabilitation organization after stroke. No overall change in satisfaction from 3 to 12 months post-stroke was found; however, being younger than 65 years increased the risk of a decline in satisfaction with functioning and wellbeing.
Collaborators at stroke units have contributed in recruiting patients.
The publication charges for this article have been funded by a grant from the publication fund of UiT The Arctic University of Norway
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize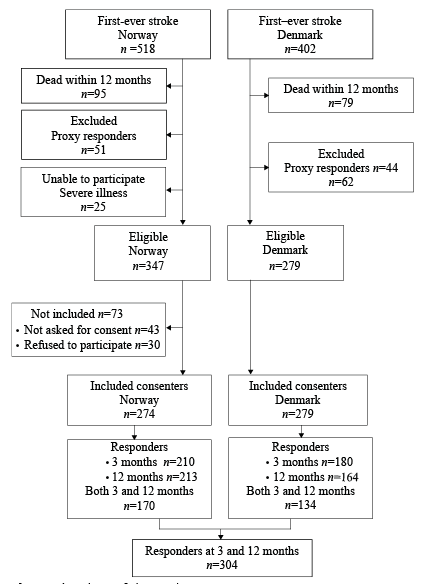 Click to show fullsize
Click to show fullsize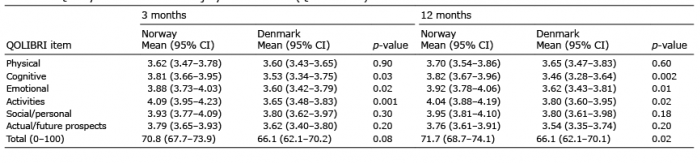 Click to show fullsize
Click to show fullsize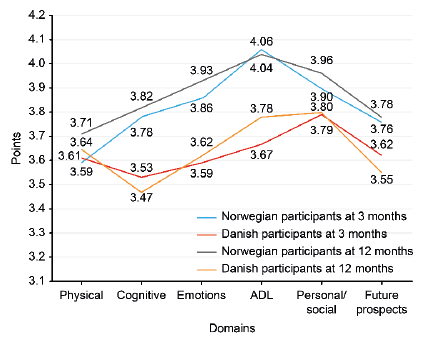 Click to show fullsize
Click to show fullsize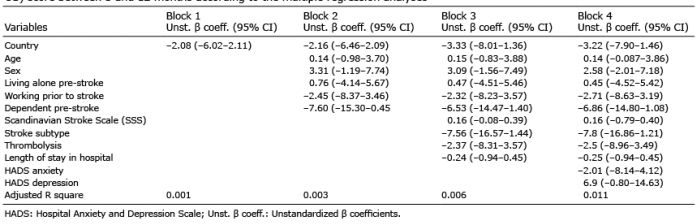 Click to show fullsize
Click to show fullsize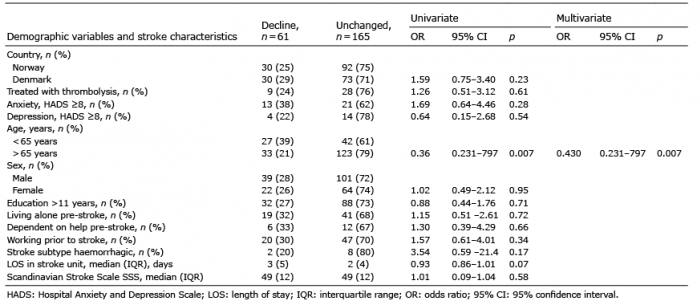 Click to show fullsize
Click to show fullsize