
From the 1Department of Rehabilitation Medicine, 2Department of Oral and Maxillofacial Surgery, University Medical Centre Groningen, University of Groningen, Groningen, The Netherlands
Objective: To assess long-term outcomes of amputation in patients with long-standing therapy-resistant complex regional pain syndrome type I (CRPS-I).
Design: Partly cross-sectional, partly longitudinal study.
Subjects: Patients who had amputation of a limb due to long-standing, therapy-resistant CRPS-I, at the University Medical Centre Groningen, The Netherlands, between May 2000 and September 2015 (n = 53) were invited to participate.
Methods: Participants were interviewed in a semi-structured way regarding mobility, pain, recurrence of CRPS-I, quality of life, and prosthesis use. Those who reported recurrence of CRPS-I underwent physical examination.
Results: A total of 47 patients (median age at time of amputation, 41.0 years; 40 women) participated. Longitudinal evaluation was possible in 17 participants. Thirty-seven participants (77%) reported an important improvement in mobility (95% confidence interval (95% CI) 63; 87%). An important reduction in pain was reported by 35 participants (73%; 95% CI 59; 83%). CRPS-I recurred in 4 of 47 participants (9%; 95% CI 3; 20%), once in the residual limb and 3 times in another limb. At the end of the study of the 35 participants fitted with a lower limb prosthesis, 24 were still using the prosthesis. Longitudinal evaluation showed no significant deteriorations.
Conclusion: Amputation can be considered as a treatment for patients with long-standing, therapy-resistant CRPS-I. Amputation can increase mobility and reduce pain, thereby improving the quality of patients’ lives. However, approximately one-quarter of participants reported deteriorations in intimacy and self-confidence after the amputation.
Key words: CRPS-I; outcome; amputation; rehabilitation; long-term.
Accepted Jul 5, 2020; Epub ahead of print Jul 30, 2020
J Rehabil Med 2020; 52: jrm00087
Correspondence address: J. H. B. Geertzen, Department of Rehabilitation Medicine, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands. E-mail j.h.b.geertzen@umcg.nl
Amputation is a mutilating treatment for persons with a life-threatening disease in an arm or leg. In patients with long-standing, therapy-resistant complex regional pain syndrome type I (CRPS-I), which is a poorly understood condition, amputation is sometimes performed; however, this treatment is controversial. This study evaluated the long-term outcomes of amputation in these patients, with respect to quality of life, pain, recurrence of CRPS-I, and functioning. In the last 15 years, 53 patients have undergone amputation at our hospital. A total of 48 patients participated in the study and were interviewed and, if indicated, physically examined. Thirty-seven patients reported an important improvement in mobility, and 35 reported an important reduction in pain. CRPS-I recurred in one out of 12 patients. Deterioration in intimacy and self-confidence were reported by 13 and 11 patients, respectively. Amputation can be considered as a treatment for these patients, because it can increase mobility and reduce pain, and thereby improve the quality of patients’ lives; however, the possibility of deteriorations such as intimacy problems or less self-confidence should be carefully considered in the decision-making process.
Complex regional pain syndrome type I (CRPS-I) is characterized by pain, which is disproportionate to the inciting event. Other symptoms include sensory, sympathetic, motor, and trophic changes (1, 2). The syndrome often requires long and intensive treatment (3), including physical therapy, occupational therapy, pharmaceutical therapy, comprehensive multidisciplinary therapy, and/or neuromodulation (4, 5). The pathophysiology of CRPS-I is not yet fully understood (2, 6). Within 6–13 months of onset, in many patients, symptoms improve considerably (7). However, in a small number of patients, CRPS-I might become therapy-resistant (i.e. not responding to medical treatment, physical therapy, occupational therapy, or multidisciplinary therapy, as recommended in the Dutch Guidelines) (4, 5). Consequently, patients might request amputation of the affected limb due to severe or unbearable pain, infections, or extremely limited mobility (4, 5, 8–10). However, amputation as a treatment for long-standing therapy-resistant CRPS-I remains controversial (4, 5, 11, 12). The procedure is irreversible, associated with surgery-related complications, and may result in phantom pain. Furthermore, CRPS-I can recur in the residual limb or elsewhere, for instance, in the opposite limb. Recently, a study comparing CRPS-I patients with and without amputation found clinically relevant differences in all outcome measures in the amputation group (13).
Limited data exist on the long-term effects of amputation as a treatment for long-standing, therapy-resistant CRPS-I. Furthermore, little is known about the course of patients’ functioning following amputation. The aim of this study was therefore to assess long-term outcomes of amputation in patients with long-standing therapy-resistant CRPS-I regarding mobility, pain, recurrence of CRPS-I, use of a prosthesis, quality of life, and functioning in daily life. This study follows up on previous research (11) and includes a larger study population, has a longer follow-up time, and allows for a longitudinal evaluation of outcomes in a subgroup
Design
The current study was partly cross-sectional, and partly longitudinal.
Subjects
A total of 53 adult patients who underwent amputation of a limb affected by long-standing, therapy-resistant CRPS-I at the University Medical Centre Groningen (UMCG) between May 2000 and September 2015 were invited to participate. Patients were referred to our outpatient rehabilitation clinic if they had long-standing CRPS-I despite earlier treatment and they had strongly expressed to their own physician that they wanted to undergo amputation. Prior to amputation, CRPS-I was diagnosed at our outpatient rehabilitation clinic, according to the International Association for the Study of Pain (IASP) criteria (14), and criteria described by Bruehl et al. (1), and Budapest criteria were also applied from 2012 onwards (15, 16). Amputation was performed due to unbearable and therapy-resistant pain, life-threatening infection, or poor mobility. For instance, if patients experienced their affected limb as an obstacle, were afraid to bump the limb, and expected to improve function and mobility by undergoing amputation of the limb. Within rehabilitation medicine, mobility is considered the ability to move or be moved freely and easily, with or without aids, wheelchairs, prostheses, orthoses, canes, crutches, etc.
Procedures
CRPS-I was considered therapy-resistant if it persisted despite earlier treatments, according to Dutch guidelines (4). First, patients who requested an amputation were extensively screened by a multidisciplinary team to determine whether amputation might be a treatment option (9, 11). This screening included an evaluation of whether all evidence-based treatments had been tried. The screening procedure and decision-making process have been described previously (12, 17).
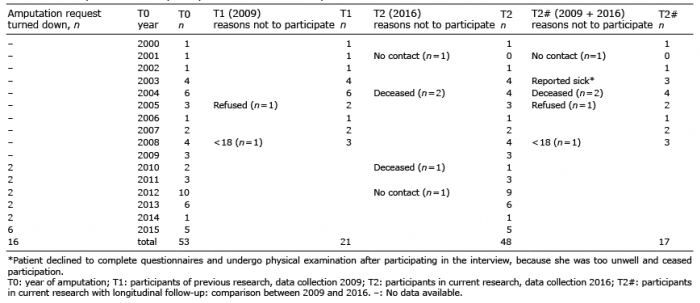
An invitation letter to participate in the follow-up study was sent to all 53 patients, of whom 21 had also participated in the previous study (11). Data for these 21 patients were used for longitudinal evaluation. Participants returned the informed consent forms using a prepaid envelope. Once written informed consent was obtained, a link to a secure website was sent to participants at which they could complete questionnaires online (a paper version was sent if preferred) and a semi-structured interview was scheduled.
Semi-structured interviews
Semi-structured interviews were conducted by telephone by a physician (J.S.) in the presence of a psychologist (E.S.) who acted as an observer. Participants were informed about the presence of an observer, but the identity of the observer was masked. Prior to the start of the interview, participants were reassured that the collected data would be handled confidentially, as described in the invitation letter. The interviews were recorded digitally. In addition, answers were recorded on paper by the physician and psychologist. Digital and paper results were compared. In case of disagreement, the results were discussed, and the interview was replayed to reassess the interpretation of the interview.
Participants were asked to rate perceived changes (comparing the current post-amputation situation to the situation prior to amputation) on a 5-point Likert scale (important improvement, slight improvement, no change, slight deterioration, important deterioration). Perceived changes concerned mobility, pain, self-care, household tasks, job participation, hobbies, sport activities, social interaction, intimacy, mood, appearance, worrying, sleep, use of pain medication, self-confidence, and the general situation after amputation. A subgroup (last 31 participants included in the study), had been asked prior to the amputation to rate their worst overall pain, perceived in the last week, on a numerical rating scale (NRS) (0 = no pain, 10 = worst imaginary pain). The same question was repeated during the interview of the current study. Finally, some open questions were asked; for example, regarding complaints if the participant suspected recurrence of CRPS-I. Interviews were completed in 30–60 min. If recurrence of CRPS-I was reported by the participant, an appointment was made for a physical examination by a physician (J.S.), in which the Budapest criteria were applied (15). This physical examination was performed at the participant’s home or in a hospital nearby, depending on the participant’s preference.
Questionnaires
A total of 5 questionnaires were completed by the participants.
The World Health Organization Quality of Life-BREF (WHOQOL-BREF) was used to assess quality of life (18). It is divided into 4 domains: physical health (7 items), psychological (6 items), social relationships (3 items), and environment (8 items) (18). Domain scores range from 4 to 20. Low scores indicate a poor quality of life. The internal consistency is good for all domains, except for the social domain, which is marginal (19).
The Connor-Davidson Resilience Scale (CD-RISC) was used to assess resilience, using 25 items (20). Higher scores on this scale indicate better resilience. The internal consistency and psychometric properties are good (21).
The Hospital Anxiety and Depression Scale (HADS) was used to assess the severity of anxiety and depression symptoms (22, 23). The internal consistency is adequate for both HADS scales (24). Scores above 8 indicate a possible anxiety disorder or depression. The depression subscale was part of the semi-structured interview.
The Trinity Amputation and Prosthesis Experience Scales – Revised (TAPES-R) was used to assess the psychosocial processes involved in adjusting to a prosthesis (25). This is a 64-item questionnaire divided into 4 sections: psychosocial adjustment; activity restriction; satisfaction with the prosthesis; and exploration of phantom pain, residual limb pain, and other medical conditions not related to the amputation. All scales and subscales show acceptable internal consistency (25). In the TAPES-R, participants are asked to rate intensity (little, annoying, alarming, terrible unbearable) and burden (none, little, moderate, much, very much) of residual limb pain, phantom sensations, and phantom pain in the last 2 weeks. Scores on the TAPES-R for activity level of lower limb amputee patients were converted into K-levels for prostheses users (26). K-levels are not applicable to persons with an upper limb amputation.
The Symptom Checklist-90 – Revised (SCL-90-R) was used to assess psychological distress (27). All 90 items are rated on a 5-point scale over the last 4 weeks. The internal consistency of the total scale is excellent (28). Higher scores represent more psychological distress.
Completed questionnaires were included in the study until 1 January 2017.
Outcome measures
Interview outcomes, scores on the TAPES-R, scores on the WHOQOL-BREF, and findings during the physical examinations were used as main outcome measures.
Statistical analyses
First, data were anonymized. Data analysis was performed with IBM SPSS Statistics for Windows (version 23.0, IBM Corp., Armonk, NY, USA). Statistical significance was set at p ≤ 0.05, unless stated otherwise. Categorical variables and ordinal variables were analysed non-parametrically. Interval data were checked for a normal distribution using Shapiro-Wilk and Kolmogorov-Smirnov tests. If these tests were significant non-parametric tests were applied, if not significant, parametric tests were applied.
Mann–Whitney test was used to analyse differences between participants amputated before and those amputated after October 2008. Distribution of perceived changes (interview items) was analysed with χ2 test to compare observed distribution with hypothesized distribution. One-sample t-test was used to analyse differences between mean scores on WHOQOL-BREF, CD-RISC and HADS of our participants, compared with norm data and control groups (28–32). SCL-90-R scores were, due to a non-normal distribution, transferred to Z-scores of norm values, and percentages of participants scoring 2 standard deviations (SD) above the norm means were calculated. For the longitudinal analyses changes in scores on WHOQOL-BREF scores, the total score on SCL-90-R and TAPES-R scores were analysed using the Wilcoxon signed-rank test due to the small sample.
A sensitivity analysis was performed for measuring mobility, pain and recurrence of CRPS-I. In the first analysis it was assumed that all participants who dropped out had the worst possible outcome (worst-case scenario); in the second analysis it was assumed that all participants who dropped out had the best possible outcome (best-case scenario).
Ethics, consent and permissions
The research protocol was approved by the local Medical Research Ethics Committee, provided that only patients aged 18 years or older were included (METc 2015/561).
Written informed consent was obtained from all individual participants included in the study.
Availability of data and material
Data availability. The study data are available on request from the rehabilitation department of UMCG and on approval of the ethics committee of the hospital. For data requests, contact Research Coordinator, J. M. Hijmans, e-mail: j.m.hijmans@umcg.nl; or Professor P. U. Dijkstra, e-mail: p.u.dijkstra@umcg.nl.
Participant characteristics
Of the 53 patients invited, 48 participated in this study (Tables I and II). One participant agreed to participate in the interview, but subsequently declined to complete the questionnaires and undergo a physical examination due to health issues. She reported recurrence of CRPS-I in the residual leg, the opposite leg, and one arm, and she experienced pulmonary and abdominal health problems.
Table I. Participation and non-participation at different time-points
Table II. Characteristics of participants amputated due to long-standing therapy-resistant complex regional pain syndrome type I (CRPS-I) (n = 48)
Participants who also participated in the previous study were significantly older (median age 53.5 vs 44.5 years) and time after amputation was significantly longer (median time after amputation 11.5 vs 3.5 years than participants who only participated in the current study. No other significant differences were found between these 2 groups in outcomes with respect to the interview items, scores on questionnaires, and recurrence of CRPS-I (Appendix I). Therefore, the 2 groups were analysed as a single group.
First, data for the total group are presented (n = 48), followed by a longitudinal analysis of the subgroup of participants who had already participated in the previous study (n = 17) (11). In most participants (n = 20, 41%) trauma was the inciting event for developing CRPS-I, followed by some form of surgery (n=16, 34%; Table II). Forty-three participants (90%) underwent a lower limb amputation.
Perceived changes in mobility and pain after amputation
Thirty-seven participants (77%) reported an important improvement in mobility (95% CI 63; 87%; Table III). An important reduction in pain was reported by 35 participants (73%; 95% CI 59; 83%). In the subgroup of 31 participants, a significant decrease in worst perceived pain in the last week, of 3.5 points (SD 3.3), was found (p < 0.001).
In the worst-case scenario for mobility, 70% (95% CI 56; 80%) of the participants would score an important improvement and for pain this would apply for 66% (95% CI 53; 77%) of the participants. In the best-case scenario for mobility, 79% (95% CI 67; 88%) of the participants would score an important improvement, and for pain this would apply for 75% (95% CI 62–85%) of the participants.
Table III. Perceived changes after amputation as reported in the interviews (n = 48)
Number and type of changes reported after amputation
After amputation, 45 participants (94%) reported one or more important improvements (ranging from 1 to 15 per participant; interquartile range (IQR): 3.0–8.8), and 20 participants (42%) reported 1 or more important deteriorations (ranging from 1 to 11 per participant; IQR: 0.0–3.0). Deterioration was reported most often for the items intimacy (n = 13, 27%), self-confidence (n = 11, 23%), household activities, and sleep (both n = 10, 21%).
Recurrence of CRPS-I
Recurrence of CRPS-I was reported by 22 participants (46%; 95% CI 33; 60%). The diagnosis was confirmed by physical examination in 4 of 47 participants (9%; 95% CI 3; 20%) after applying the Budapest criteria. One participant refused a physical examination (Table IV). In the worst-case scenario regarding recurrence of CRPS-I, 27 of 53 participants (51%; 95% CI 38; 64%) would have self-reported recurrence and 10 of 53 participants (19%; 95% CI 11; 31%) would have recurrence using the Budapest criteria. In the best-case scenario regarding recurrence of CRPS-I, 22 of 53 participants (42%; 95% CI 29; 55%) would have self-reported recurrence and 4 of 53 participants (8%; 95% CI 3; 18%) would have recurrence using the Budapest criteria. Self-reported residual limb recurrence of CRPS-I developed within 3.5 years (range 0–3.3 years) in 13 participants and self-reported recurrence elsewhere developed within 5 years in 4 of 6 participants (range 1.0–11.0 years; total n < 22 due to missing values).
Table IV. Post-amputation results: reported recurrence by participants, recurrence based on to physical examination using 2 sets of criteria and prosthesis use, as reported in the interviews (n = 48)
Prosthesis use
Thirty-five participants (73%) were fitted with a lower limb prosthesis (Table IV). Eleven participants no longer used the prosthesis at follow-up due to pain or fitting problems. Nineteen participants (40%) used the lower limb prosthesis for 8 h or more daily. Two participants with an upper limb amputation (1 trans-humeral and one trans-radial amputation) were fitted with a prosthesis and both used the prosthesis for 4–8 h daily.
Re-amputation
Seven participants (15%) underwent a re-amputation due to recurrence of CRPS-I, of which 6 participants were re-amputated without consulting our department. These re-amputations mostly took place in other hospitals. One participant had already undergone an amputation before re-amputation in our centre, due to recurrence of CRPS-I in the same limb. Of these 7 participants, 2 (29%) still had complaints and reported recurrence of CRPS-I elsewhere. Nine participants (19%) underwent re-surgery in the residual limb for reasons other than CRPS-I (e.g. adherent scars or bone spurs).
Residual limb pain was experienced by 23 of 43 participants (missing n = 5) and phantom pain by 23 of 42 participants (missing n = 6) (Table V). Compared with norm data participants had a significantly poorer quality of life (physical, social and environment), and anxiety score of the HADS. Nine participants (19%) scored 2 SD above the norm mean of the SCL-90-R total score. Participants had a significantly higher quality of life (physical and psychological) and resilience scores compared with rehabilitation outpatients. Anxiety and depression scores were significantly lower compared with persons with phantom pain. Three participants scored 2 SD above the mean of SCL-90-R total score of patients with chronic pain (Table VI).
Satisfaction with decision for amputation
A total of 47 (98%) participants stated that they would choose an amputation again under the same circumstances. One participant would not choose amputation again. In her case, a life-threatening infection was the primary reason for a lower limb amputation.
Table V. Experienced intensity and burden of residual limb pain and phantom pain based on the outcomes of the Trinity Amputation and Prosthesis Experience Scales – Revised (TAPES-R)
Table VI. Results of questionnaires (WHOQOL-BREF, CD-RISC, and HADS SCL-90-R), compared with reference and control groups
Longitudinal follow-up
Longitudinal analysis (n = 17) showed no significant changes in WHOQOL-BREF scores and total score on the SCL-90-R (Table VII). Burden of phantom sensations, residual limb pain, and phantom pain was significantly less compared with the previous study (11). Post-hoc analysis of the intensity of residual limb and phantom pain showed that 2 participants still experienced alarming to terrible residual limb pain, and 2 participants still experienced alarming phantom pain. No participants still experienced unbearable residual limb or phantom pain. Fewer participants reported wearing their prosthesis (9 participants in current study vs 11 participants in the previous study); however, this difference was not significant. The outcomes of the interviews had not changed significantly (data not shown; available on request).
Table VII. Longitudinal analysis of questionnaires outcomes in patients who underwent an amputation for complex regional pain syndrome type I (CRPS-I) (n = 17)
Approximately three-quarters of the participants perceived important improvements in mobility and pain after amputation. Recurrence of CRPS-I was reported by half of the participants, but could be confirmed in only 4 participants after applying the Budapest criteria. The improvement in mobility while performing specific activities (e.g. using a toilet, performing hobbies/sports, or participating at work) could not be generalized to all activities. General symptoms, such as worrying, mood, and negative attention, did not change, for the most part, after the amputation. Analysis of deterioration related to specific activities occurred in less than one-third of participants. The above-reported results should be taken into account when considering an amputation, because treatment options for therapy-resistant CRPS-I are scarce, and patients suffer immensely (10).
Pain reduction was the main goal of most participants, and a majority of participants indeed experienced an important improvement in pain, which contrasts with another study on amputation in patients with CRPS-I, in which only 11 participants (32%) experienced pain relief (8). This difference might be based on our assessment of improvement instead of relief. The mean decrease in worst pain perceived in the last week (3.5 points) is clinically relevant. In a comparison of pain intensity between amputee and non-amputee patients with CRPS-I, amputee CRPS-I patients experienced a mean of 3.2 points less intense pain (13).
The second goal of many participants was an increase in mobility. More than three-quarters of the participants reported an important increase in mobility. When asked for specific activities that require mobility, fewer participants experienced improvement and more participants experienced deteriorations. For some activities, the discrepancy between general improvement in mobility and perceived deterioration of one specific activity is explainable. For example, participants mentioned disappointment due to difficulties donning and doffing their prosthesis in the restroom, but they still experienced a general improvement in mobility because they could walk with a prosthesis. Furthermore, wheelchair mobility may be experienced as improved, because participants’ fear of bumping the affected limb decreased or disappeared altogether. Improved wheelchair mobility may also explain the discrepancy between improvement in general mobility and the relatively low number of participants using a prosthesis. The discrepancies between general improvement in mobility and deterioration of mobility related to work, hobbies, and sports might be explained by what participants prioritize. Poor social acceptance of disabled persons in work and leisure activities might explain part of these discrepancies.
A striking deterioration was seen for the items self-confidence and intimacy post-amputation. Negative effects of an amputation on social function and intimacy have been reported previously (33, 34). These effects might be linked to perceived appearance. Deterioration of appearance in relation to the reported deterioration of intimacy was analysed in a post-hoc analysis. Only 4 of the 13 participants (31%) who reported deterioration of intimacy also reported deterioration of appearance.
Although quality of life in participants did not meet Dutch norm standards, it did exceed standards for rehabilitation outpatients. The difference from the Dutch norm standards is only of clinical importance relevant to the physical domain and may be explained by the amputation, and by the fact that after recovery from residual symptoms of CRPS-1 may still be present (35). Approximately half of participants reported recurrence of CRPS-I, but recurrence could be confirmed in only 4 participants by means of physical examination. Most often, signs and symptoms could be better explained by another condition; for example, neuroma. In addition, in many cases not enough symptoms were present to meet the Budapest criteria. In a systematic review, recurrence of CRPS-I was reported in 34 of 65 participants (52%); however, the criteria used for the diagnosis of recurrence were not reported in the source studies (9).
Almost all participants stated that they would choose an amputation again, which is a positive result, although this could have been influenced by cognitive dissonance. The theory of cognitive dissonance predicts that, in case of an irrevocable choice, people try to minimize regret (36). An amputation cannot be reversed; hence, instead of regretting this decision, it feels better to consider that it was the best choice.
The low mean scores on the depression and anxiety scale after amputation are remarkable. Another study found that anxiety and pain-related fear, especially, were associated with poor outcomes in patients with CRPS-I (37). Anxiety and pain-related fear tended to decrease after 1 year in that study (by that time, most patients had fewer symptoms than at the start of the CRPS-I). It is possible that in the current study the amputation was felt as a relief, or it could be that patients who were motivated to undergo the amputation had lower scores on depression and anxiety prior to the amputation.
The mean age of the participants in this study was lower than that of patients with CRPS-I in the Netherlands reported previously (38). The highest incidence of CRPS-I was found in females aged 61–70 years and the upper extremity was more often affected than the lower extremity (38). This age difference could be related to the severity of CRPS-I. In the current study, only patients with long-standing, therapy-resistant CRPS-I who were motivated to undergo an amputation were seen, whereas the other study is a cohort of all patients with CRPS-I recorded in a general practice research database over a 9-year period. The current participants seem to be more similar to those included in a systematic review (9) than to patients with CRPS-I recorded in a general practice research database (38).
In the longitudinal analysis prosthesis use remained stable over 7 years. Small, but significant, reductions were found in residual limb pain and phantom pain. Similar improvements in phantom pain have been reported previously (39).
A strength of the current study was the relatively large number of participants. Compared with the previous study in 2012, twice as many participants were included.
The current study lacked a control group of patients with long-standing therapy-resistant CRPS-I who did not undergo an amputation. Nevertheless, it was possible to compare the current data with norm values. Only patients with an amputation were included. Therefore, no insight into quality of life and functioning of patients who were refused an amputation could be gained. In the period January 2010 to September 2015, 16 patients who requested an amputation were turned down. The main considerations were (more items per person are possible): criteria for CRPS-I were not met (n = 6); patients did not have realistic expectations about outcomes of the amputation (n = 4); not all treatments according to the Dutch guidelines had been tried (4) (n = 4, of which 3 patients were advised to follow a multidisciplinary rehabilitation programme and 1 patient was advised to try neuromodulation); the extremity was still functional (n = 2); comorbidity negatively influenced possible outcomes (n = 2); conversion (n = 1); suspicion of CRPS-2 (n = 1); and suspicion of auto-mutilation (n = 1). Patients’ requests that were turned down were not systematically recorded before 2010.
The participants in the current study form a selection of patients. During the study period diagnostic criteria for CRPS-I changed, making the interpretation of diagnosis and recurrence rather difficult. We therefore decided to apply the most recent criteria to determine recurrence, although these criteria (the Budapest criteria) are also under scrutiny. Some critics claim that CRPS-I is not a disease, that overlap exists with other diseases, and that the validity of the criteria is not sufficient and not tested thoroughly (40). Furthermore, the follow-up time was relatively long for many participants, which could have resulted in recall bias when assessing the situation prior to the amputation.
Conclusion
Approximately 75% of the participants in this study experienced an important improvement in mobility and reduction in pain. Longitudinal follow-up showed no significant deteriorations after amputation. Some participants experienced residual symptoms of the CRPS-I. Approximately one-quarter of the participants reported deteriorations in intimacy and self-confidence after the amputation. Therefore, it is important to extensively screen patients to assess whether their post-amputation expectations and goals are realistic. For patients with long-standing, therapy-resistant CRPS-I, amputation may be considered as a treatment option.
Funding. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors have no conflicts of interests to declare.
Appendix I. Overview of subgroup A (patients amputated between May 2000 and October 2008) vs subgroup B (patients amputated between October 2008 and September 2015)
Appendix I. cont


 Click to show fullsize
Click to show fullsize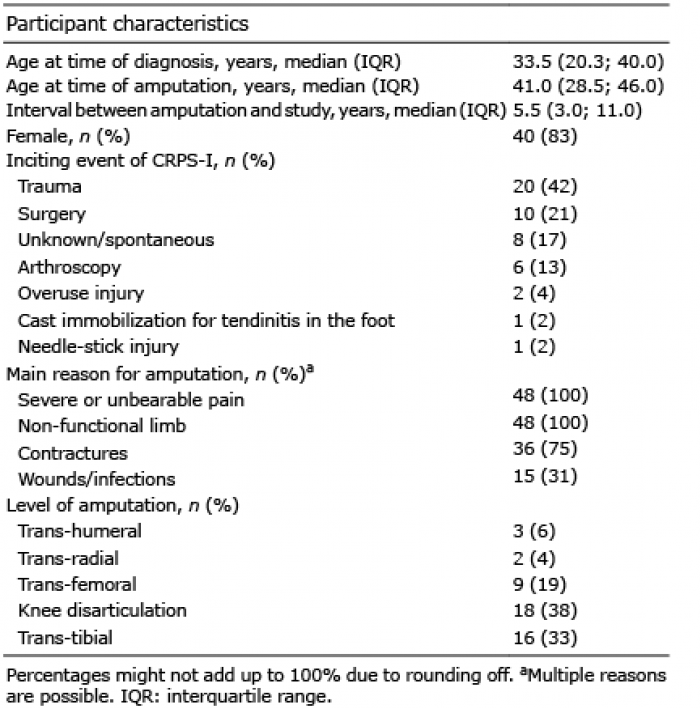 Click to show fullsize
Click to show fullsize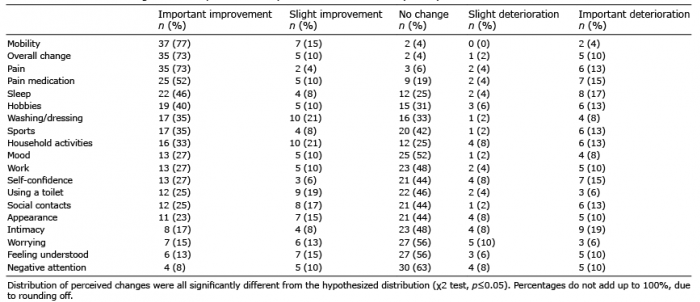 Click to show fullsize
Click to show fullsize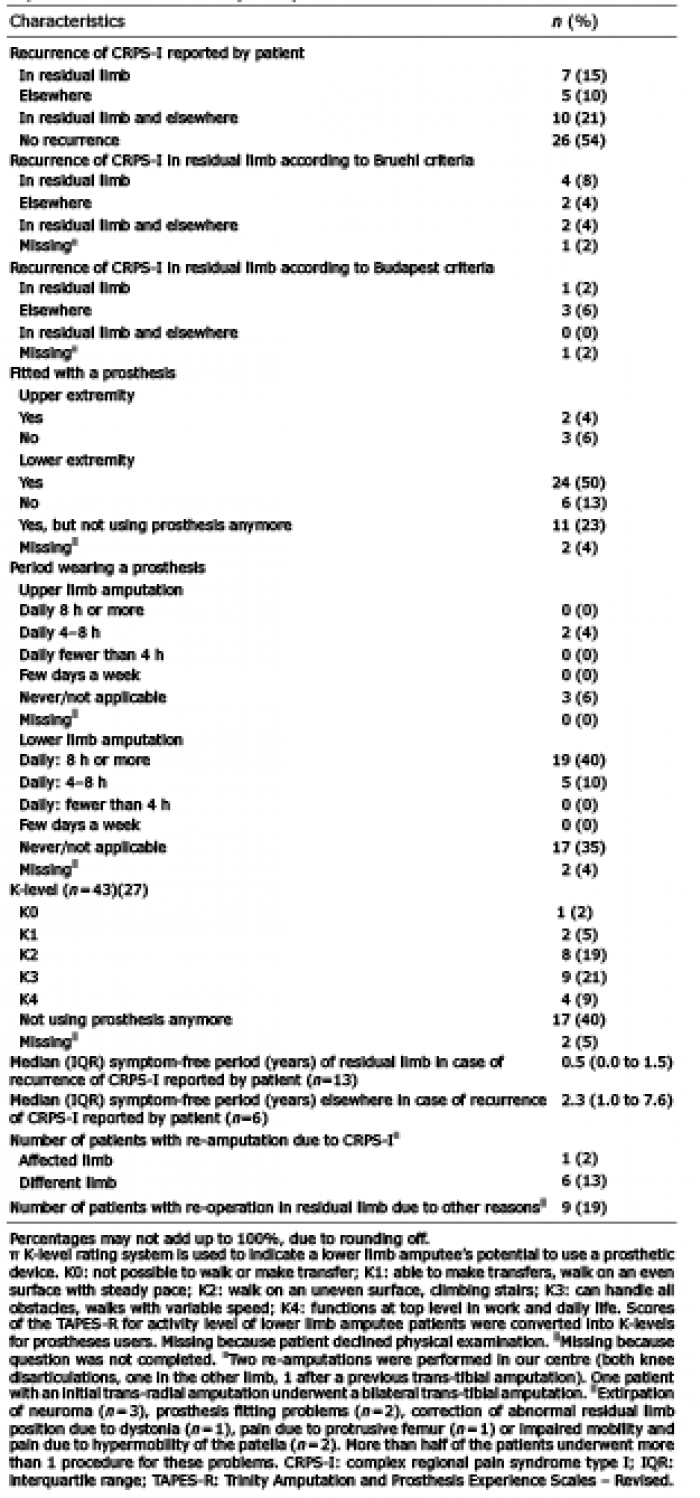 Click to show fullsize
Click to show fullsize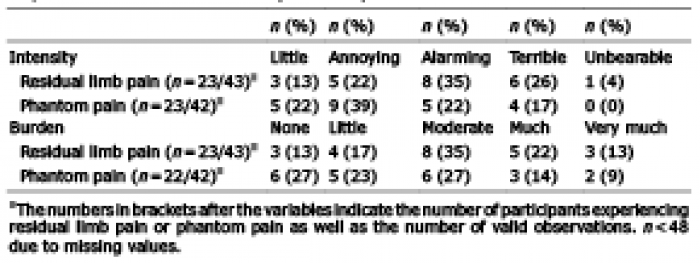 Click to show fullsize
Click to show fullsize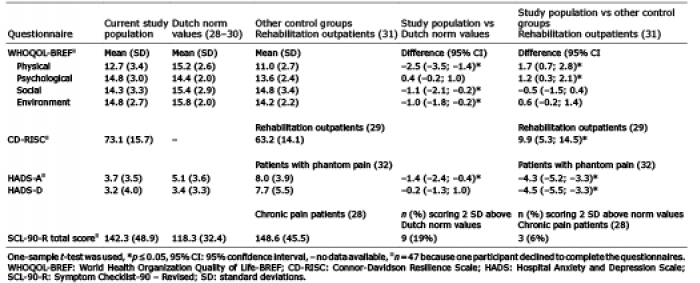 Click to show fullsize
Click to show fullsize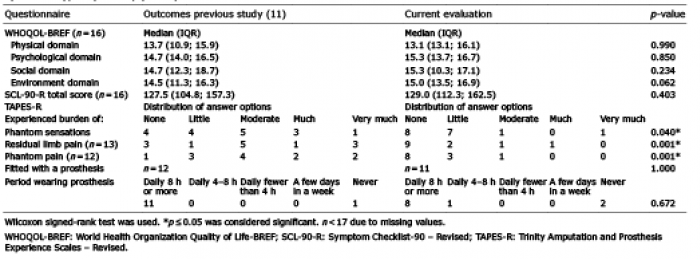 Click to show fullsize
Click to show fullsize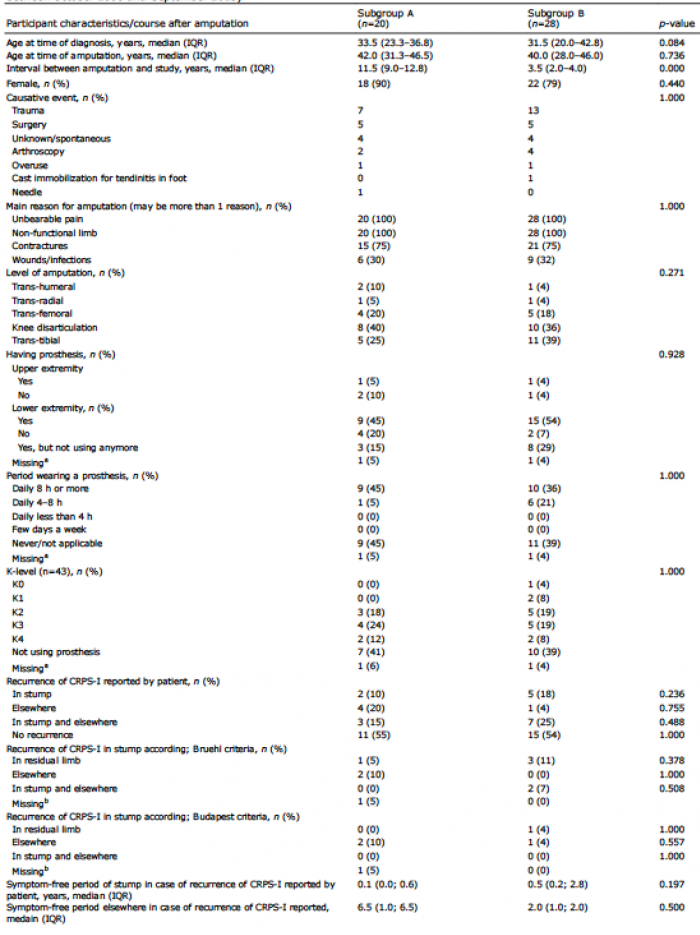 Click to show fullsize
Click to show fullsize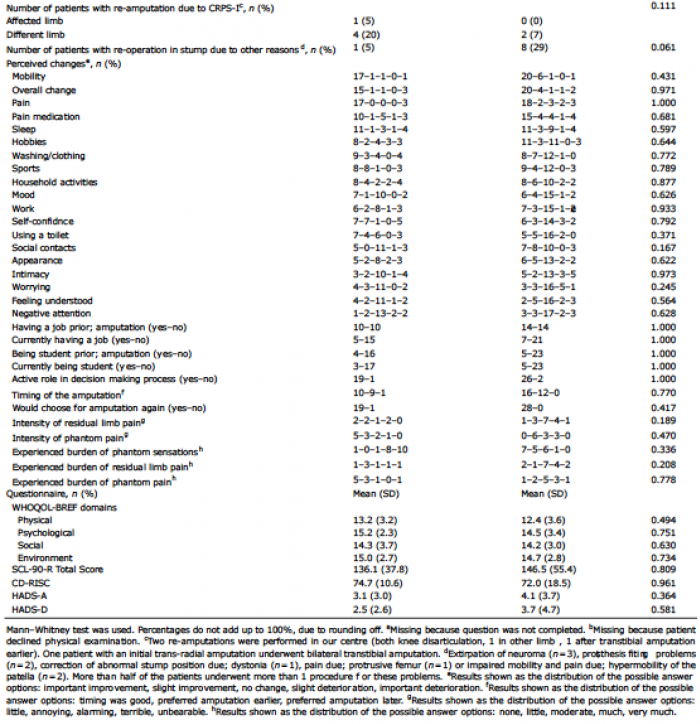 Click to show fullsize
Click to show fullsize