
From the 1Maastricht University Medical Centre, Department of Trauma Surgery, Maastricht, 2Adelante Centre of Expertise in Rehabilitation and Audiology, Hoensbroek, 3Research School CAPHRI, Department of Rehabilitation Medicine and 4Nutrim School for Nutrition, Toxicology and Metabolism, Maastricht University, Maastricht, The Netherlands
Background: Ambulant biofeedback devices can be used to provide real-time feedback for trauma patients on weight-bearing regimes. The devices also enable prescribing clinicians to monitor and train patients’ level of weight-bearing. However, there is limited evidence regarding the feasibility of use of such devices in controlling weight-bearing, and their full potential remains to be elucidated.
Objective: To investigate the feasibility of using ambulant biofeedback training devices to improve compliance with weight-bearing regimes in trauma patients with lower extremity fractures.
Methods: A literature review of the feasibility and clinical validity of ambulant biofeedback devices.
Results: Three clinically validated biofeedback devices were found feasible for use in monitoring the compliance of patients who have lower extremity fractures with different weight-bearing regimes.
Conclusion: Further information about the feasibility and clinical validity of biofeedback training devices is needed in order to optimize weight-bearing instructions for patients.
Key words: lower extremity fracture; trauma patient; compliance; ambulatory biofeedback device; permissive weight-bearing; partial weight-bearing.
Accepted Jul 9, 2020; Epub ahead of print Aug 6, 2020
J Rehabil Med 2020; 52: jrm00092
Correspondence address: Eline Marjolijn Jagtenberg, Maastricht University Medical Centre+Department of Traumatology, P. Debyelaan 25, 6229 HX Maastricht. E-mail: e.jagtenberg@student.maastrichtuniversity.nl
Biofeedback devices, worn as an insole, can be used to provide real-time feedback to trauma patients with fractures of the lower extremities who are undergoing weight-bearing regimes. These devices also enable clinicians to monitor and train the patients’ level of weight-bearing. However, there is little evidence about the feasibility of use of these devices in controlling weight-bearing, and their full potential remains to be investigated.
In order to optimize weight-bearing instructions for
patients, knowledge of the feasibility and clinical validity of the available biofeedback training devices is required. This narrative review examines the feasibility of use of ambulant biofeedback training devices in trauma patients with lower extremity fractures in improving compliance with weight-bearing regimes.
Fractures of the lower extremities account for approximately one-third of all fractures (1). After trauma, or following surgery for the fracture, such patients are often prescribed weight-bearing regimes, in order to achieve optimal healing and prognosis (2). Although weight-bearing instructions are provided, patients’ compliance with these instructions is limited (2–5) due to difficulty in assessing the pressure exerted on the lower extremity (6), and the lack of adequate training methodologies (2, 4, 7, 8).
Current training methodologies to improve patients’ compliance include the use of bathroom scales, verbal instructions, tactile feedback, force plates and biofeedback devices. Hustedt et al. concluded that biofeedback devices are superior to other methods in enabling patients to comply with partial weight-bearing (2). Ambulant biofeedback devices can be used to provide the therapist and/or patient with real-time feedback, by continuously measuring the weight borne on the patient’s affected leg (2–4, 9). These devices may be of importance to achieve optimal compliance with weight-bearing regimes, by monitoring patient performance, which can then be influenced towards optimal healing conditions (10). There is limited evidence regarding the feasibility of use and clinical validity of biofeedback devices in optimizing weight-bearing, and the full potential of these devices remains to be investigated (2).
The aim of this review was to examine the feasibility of use of ambulant biofeedback training devices in trauma patients who have lower extremity fractures, for improving compliance with weight-bearing regimes.
The standard in post-surgical rehabilitation for patients with lower extremity fractures is non-weight-bearing for 12 weeks, followed by a gradual increase in weight-bearing, guided by the percentage of body weight (e.g. 2 weeks 25%, 2 weeks 50%, 2 weeks 75%, and thereafter 100% of body weight) (11). Non-weight-bearing is instructed to prevent failure of the fixation device, delayed fracture healing, or even non-union of bone fragments caused by excessive movement of fracture parts (12–14). Repetitive loads of sub-maximal weight-bearing, however, are associated with increased bone growth, and are necessary for fracture healing caused by stimulated osteoblastic activity (15–19). Thus, non-weight-bearing could be replaced by regimes of earlier/gradual increase in weight-bearing as fracture healing progresses (2).
Orthopaedic surgeons are currently trained to prescribe non-weight-bearing for 6 weeks post-surgery of the injured limb, since overloading after a lower extremity fracture is thought to increase the risk of complications (e.g. malreduction and implant failure) (14, 20–22). On the other hand, early weight-bearing may be important for the successful treatment of lower extremity fractures, and is associated with an earlier return to full weight-bearing (20, 23). Furthermore, several studies have shown that early weight-bearing is not associated with a higher risk of complications (17, 20, 24).
Permissive weight-bearing is a recently developed post-surgical protocol, in which the affected leg is allowed to bear weight earlier than in current post-surgical rehabilitation programmes (18). The progression of weight-bearing is guided by the subjective experience of the patient (e.g. pain and confidence to bear weight) and by objective clinical symptoms occurring during rehabilitation (e.g. limb temperature, oedema and gait parameters) (25, 26). To date, no high-level studies have been published regarding the effectiveness of permissive weight-bearing.
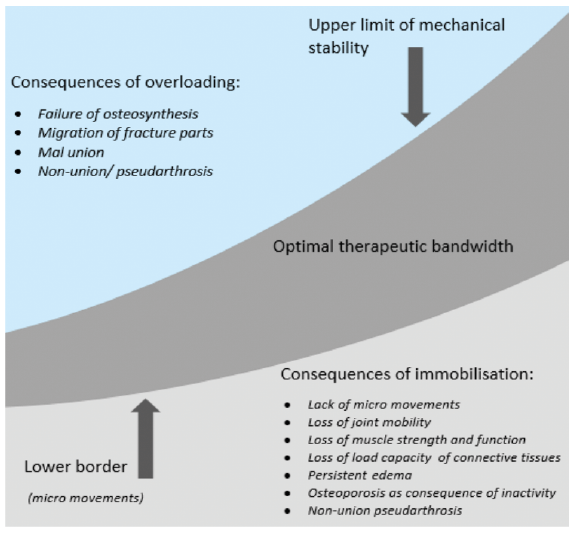
It is important to determine the optimal therapeutic range of weight-bearing in patients with a lower extremity fracture, since this will minimize negative consequences and optimize the postoperative rehabilitation protocol (Fig. 1) (21, 22, 26). Rehabilitation of patients with lower extremity fractures must balance the limitation of weight-bearing in order to protect the surgical fixture, with increasing weight-bearing to facilitate the repetitive stimulation of bone growth (2).
Fig. 1. Overview of consequences of loading in the consolidation process.
A study by van der Vusse et al. revealed that there is no consensus among orthopaedic surgeons regarding early weight-bearing regimes in surgically treated trauma patients with tibial plateau fractures (22). Most surgeons deviate from their own institutional guidelines, based on their clinical experience and gut feeling (22). Despite the lack of consensus, most surgeons and physicians still instruct their patients to restrict weight-bearing (2). Furthermore, although weight-bearing instructions are given, patients frequently do not follow the instructions despite their willingness to comply (2–5). Reasons for this non-compliance include difficulty in assessing the weight borne on the lower extremity (6) and the shortcoming of adequate methodologies to train patients in weight-bearing regimes (2, 4, 7, 8). Training methodologies include tactile feedback, bathroom scales, force plates, verbal instructions and biofeedback devices (2). Ambulant biofeedback devices may enable patients to comply with the weight-bearing instructions in their daily lives.
Search strategy
A literature search was conducted to find studies on ambulant biofeedback systems suitable for use in training patients with lower extremity fractures in a specific weight-bearing regime. PubMed was searched for studies investigating the feasibility and clinical validity of biofeedback devices used for improving patients’ compliance with weight-bearing regimes. The following Medical Subject Headings (MeSH) terms and free terms were used: ((((((((“Biofeedback, Psychology”[MeSh]) OR biofeedback device) OR ambulant biofeedback devices) OR ambulatory biofeedback devices)) OR pedobarography insole) OR gait analysis insole)) AND ((“Weight-Bearing”[MeSh]) OR weight-bearing). In addition, Google Scholar was searched for studies not included in PubMed, with the following main keywords: biofeedback devices, weight-bearing, lower extremities. Finally, the reference lists of all included studies were manually reviewed to identify additional eligible studies that were not identified in the electronic database search. Studies were included if they described the clinical validity, feasibility, usability or reliability of ambulatory biofeedback devices in healthy subjects or patients with injuries of the lower extremities. Studies were excluded if fewer than 5 participants were included, participants were < 18 years, publication was in a language other than English, or if they included protocols describing devices that were in the first phase of development, i.e. up to a technical readiness level (TLR) of 4. Moreover, studies were excluded if they investigated the use of biofeedback systems in patients with neurological conditions.
The literature search identified 155 relevant studies, as shown in Fig. 2. From these, 9 eligible studies were found, describing 3 commonly used ambulant biofeedback devices to monitor weight-bearing of the lower extremities: OpenGo Science (Moticon GmbH, Munich, Germany), Sensistep (Evalan BV, Amsterdam, The Netherlands) and Smartstep (Andante Medical Devices, Beer Sheva, Israel). The feasibility of use and clinical validity of these biofeedback devices are shown in Table I. The studies included in this review were selected on the basis of the validation and clinical findings of the ambulant biofeedback systems. For studies on clinical findings, this also entailed examination of a relevant control group and, if possible, the examination was performed as a randomized controlled trial.
Fig. 2. Study selection described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Table I. Studies evaluating the feasibility of use and clinical validity of currently available ambulant biofeedback devices inpatients with lowe extremity fractures
Three biofeedback devices were feasible for use in trauma patients with fractures of the lower extremities. These devices (Sensistep, OpenGo Science and Smartstep) have been clinically validated to monitor compliance in trauma patients with lower extremity fractures.
Sensistep. This biofeedback system uses a force sensor in custom-made sandals. The sensor sends data regarding the pressure loads, via Bluetooth 4.0, to a wrist-worn device, which acts as feedback instrument for patients and as a data logger. Using a bespoke application installed on a tablet, the data can be shown as real-time graphics and the physician can set a specific target load for the patient (28). In a study by Raaben et al., 10 healthy volunteers were measured with the Sensistep insoles and a dual-belt instrumented treadmill, in order to validate the system in the dynamic situation. They concluded that the use of Sensistep resulted in accurate measurements in the static situation, but that the system needed to be optimized to improve results in the dynamic situation (28). A pilot randomized control trial, also by Raaben et al. (27), determined the immediate and late effect of Sensistep on weight-bearing during rehabilitation after total hip arthroplasty in elderly patients. Twenty-four participants were randomized to the intervention or the control group, in which the intervention group received real-time biofeedback. Raaben et al. concluded that a significant improvement in compliance with therapy occurred in the intervention group, and that early biofeedback had a lasting effect (27). Finally, in a study of the effect of Sensistep in 11 participants with full weight-bearing and 12 participants with touch-down weight-bearing after lower extremity fractures, Raaben et al. found that using the device resulted in significantly higher peak loads in full weight-bearing and increased accuracy of individual steps in touch-down weight-bearing (29).
OpenGo Science. This biofeedback system comprises sensor insoles, an application to analyse the data on a PC and an Adaptive Network Topology (ANT) radio stick for wireless transmission of data between the insoles and the application. The insole comprises 13 pressure sensors, a temperature sensor, and a triaxial acceleration sensor. In live mode, the pressure sensors send the data directly to the application on the PC (31). In an initial study of the OpenGo Science insole, Braun et al. concluded that it is clinically feasible for use in measuring gait differences during the aftercare of lower extremity fractures. They monitored 10 patients with the OpenGo insole for 3 months after surgery for an ankle fracture (10). In another study, Braun et al. investigated the validity and reliability of the OpenGo Science system by collecting gait data from 12 healthy participants at 2 different speeds on a treadmill. OpenGo Science showed comparable reliability and validity to a stationary analysis tool, indicating that OpenGo Science is feasible for use in clinical trials (33). Furthermore, Braun et al. investigated the feasibility of use of the OpenGo Science system in an observational study (30). The OpenGo Science insoles were placed in the shoes of 30 patients during rehabilitation after tibial shaft, intertrochanteric femur and ankle fractures. Compliance with the weight-bearing instructions provided was low, and adherence further decreased over time. The study also found that OpenGo Science appears feasible for use in continuous determination of weight-bearing, and that it could help to establish individual weight-bearing instructions (30). In a study by Van Lieshout et al., 9 patients who were prescribed partial weight-bearing were invited to use OpenGo Science insoles during rehabilitation. Usability of the insoles was measured by a semi-structured interview, a think-aloud method, closed questions and by the System-Usability Scale (35, 36). Overall usability from the patient’s and therapist’s perspective were acceptable (31). In a validation study by Van Lieshout et al. (32), 55 healthy adults were instructed to walk with crutches under different weight-bearing conditions, categorized as a percentage range of body weight: 1–20%, 20–50% and 50–75%. Peak force data from the biofeedback system were subsequently compared with the peak force measured with a force plate. OpenGo Science provided valid feedback only in the lower weight-bearing categories (1–20% and 20–50% of body weight) (32).
SmartStep. This biofeedback system comprises flexible insoles with 2 separate air pockets. A microprocessor control unit is worn around the ankle, which is connected to the air pockets if they are inflated. This microprocessor control unit contains 2 pressure sensors, which provide feedback to the patient by producing an audio signal when they reach a pre-set weight-bearing threshold. Using an application on a PC, and wireless communication via Bluetooth, thresholds can be set and the data analysed (31). SmartStep was tested in the study by Van Lieshout et al. described above. They found that the overall usability of the system was only acceptable from the patient’s perspective. Usability from the physical therapists’ perspective was not acceptable, since the majority had problems inflating the air pockets and attaching SmartStep to the patients after hip surgery (31). A study by Isakov et al. investigating the validity and effectiveness of the SmartStep in 11 healthy subjects and 42 patients with an affected leg, found that the system was reliable and that patients recommended for full weight-bearing could significantly improve body-weight loading with the help of the device (34).
The studies included in this review have some limitations. First, most studies did not investigate client groups appropriate to the aim of the review. Raaben et al. (27), investigated patients who had undergone total hip arthroplasty and patients with lower extremity fractures (29), whereas Van Lieshout et al. (31) studied patients who had undergone surgery of the hip, knee or femur. Braun et al. (10, 30) investigated patients after ankle and femur fractures, and Isakov et al, studied healthy subjects and those with an affected limb (34), while the other studies included only healthy subjects (28, 32, 33). The weight-bearing kinematics of these healthy subjects may not be representative of patients with fractures of the lower extremities (32). Validation in patient populations is therefore necessary. Additional aspects reducing the methodological quality of the studies included in this review entail small study populations and variation in these study sizes, differences in test circumstances, such as validation with the help of different tools (e.g. crutches, treadmill, scales) and the differences in follow-up duration, study designs and, in most studies, the lack of patient and/or control groups.
Other aspects that should be taken into account are the costs and the usability of the devices. Costs may have influenced the reported outcomes in the studies, since knowledge of the high costs of the devices might influence acceptability by undermining their acceptance (37). Moreover, costs differ between the devices, and cost-effectiveness should be investigated in order to draw solid conclusions. The usability of the devices is also important. The time required to set up the device and to train the therapists and/or clients in their use also vary: OpenGo Science was found to be easy to use, and Smartstep was found to be a highly visible, inconvenient device (31).
This review provides an overview of studies regarding current feasible, validated ambulatory biofeedback devices. However, further research is needed in order to draw conclusions about the use of these devices. The quantity and methodological quality of currently available studies is limited; therefore a systematic review is not yet possible.
This narrative review of three clinically validated ambulatory biofeedback devices found that they are feasible for use in monitoring the compliance of patients with lower extremity fractures undergoing weight-bearing regimes. Use of such devices could enable optimal compliance with weight-bearing regimes, since they can be used to adjust aftercare protocols based on real-time patient conditions, rather than fixed weight-bearing regimes. All three ambulatory, clinically validated, biofeedback devices appear feasible for use in improving compliance with weight-bearing regimes among patients who have lower extremity fractures. However, discrepancies in accuracy were evident between the devices regarding different levels of weight-bearing, the usability of the SmartStep was not acceptable from the physician’s perspective, and there were problems with all three devices in monitoring weight-bearing loads above 50% during walking.
Ambulatory biofeedback devices have shown promising results in providing feedback to patients with lower extremity fractures, enabling them to comply with weight-bearing. However, since these devices currently only provide real-time feedback during training sessions, the question arises as to how long the learning effects of such training last, and whether use of the devices provides long-term benefit for the patient. Further clinical research into the feasibility of use and the effects of the biofeedback devices on the course of post-traumatic rehabilitation is needed in order to monitor weight-bearing in trauma patients with fractures of the lower extremities. The cost of the devices varies, and cost-effectiveness analyses of the devices are lacking. These biofeedback devices should be developed further in order to expand their clinical application (e.g. in measuring quality of gait, signs of overloading, and pressure distribution).
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize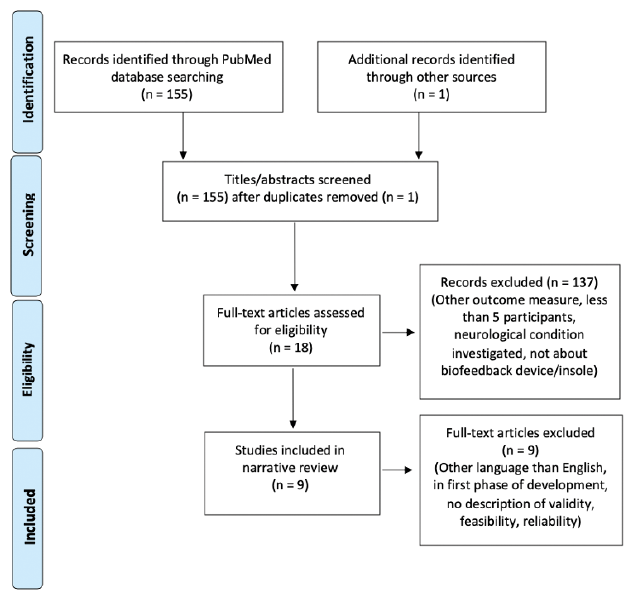 Click to show fullsize
Click to show fullsize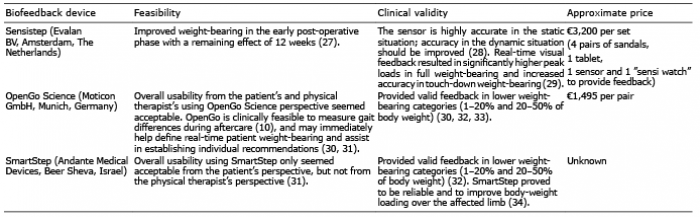 Click to show fullsize
Click to show fullsize