
From the 1Department of Rehabilitation Medicine and 2Department of Orthopedic Surgery, Tokyo Medical and Dental University, Tokyo, Japan
Objective: To describe the effectiveness and risk manage-ment of remote rehabilitation for coronavirus disease (COVID-19) patients in general wards.
Design: Single-centre, retrospective, observational study.
Patients: COVID-19 patients undergoing rehabilitation (24 April to 24 May 2020).
Methods: All COVID-19 inpatients undergoing rehabilitation in the general ward of Tokyo Medical and Dental University were assessed. Data were collected on age, sex, physical ability, rehabilitation modality (remote/direct), need for intubation or extracorporeal membrane oxygenation, degree of pneumonia, oxygen therapy from the start of rehabilitation, D-dimer and C-reactive protein levels, and rehabilitation-related complications. Activities of daily living were measured using the Barthel Index.
Results: Out of a total of 43 patients, 14 were initially provided with remote rehabilitation and 29 with direct (hands-on) rehabilitation. Four patients were switched from direct to remote rehabilitation during the study, thus at the end of the study there were 18 in the remote rehabilitation group and 25 in the direct rehabilitation group. Patients in remote rehabilitation were significantly younger than those in direct rehabilitation. Of 12 patients who required intubation, 3 were given remote rehabilitation. One extracorporeal membrane oxygenation survivor underwent direct rehabilitation. All patients on remote rehabilitation were discharged home or to a hotel. Twelve out of 29 patients on direct rehabilitation were transferred to a rehabilitation hospital due to delayed recovery of activities of daily living. No serious adverse events occurred.
Conclusion: Effective and safe remote rehabilitation was performed in 41.9% of COVID-19 patients in this study, which resulted in which facilitated rehabilitation in COVID-19 specialized general wards.
Key words: coronavirus; early ambulation; infection; pulmonary embolism; rehabilitation; risk management.
Accepted Aug 19, 2020; Epub ahead of print Aug 26, 2020
J Rehabil Med 2020; 52: jrm00095
Correspondence address: Tomoko Sakai, Department of Orthopedics, Tokyo Medical and Dental University, 1-5-45 Yushima, Bunkyo-ku, Tokyo 113-8519, Japan. E-mail: t_sakai.orth@tmd.ac.jp
We assessed the usefulness of remote rehabilitation therapy for coronavirus disease (COVID-19) patients from 24 April to 24 May 2020 in Tokyo Medical and University. A rehabilitation modality was devised to be applied from green area (not-infected area) to red area (infected area) using a mobile terminal. This allowed 18 of 43 patients to be treated indirectly by remote rehabilitation. The patients were significantly younger than those undergoing direct rehabilitation. Four patients switched from direct to remote rehabilitation in the course. All patients undergoing remote rehabilitation were discharged home or to a hotel. No serious adverse events were observed. Remote rehabilitation was an effective and safe modality against the transmission of infection and could facilitate rehabilitation of patients in COVID-19 wards
Since the first patient with coronavirus disease (COVID-19) was confirmed in Wuhan, China, the disease has spread rapidly to become a worldwide pandemic (1). The disease has high contagiousness and mortality. There is limited published research on the rehabilitation of COVID-19 patients (2). In order to prevent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and nosocomial infections and save on personal protective equipment (PPE), current COVID-19 guidelines do not recommend rehabilitation, except for respiratory physiotherapy in the intensive care unit (ICU) for severe symptoms, and mobilization, exercise, and rehabilitation of patients who are frail, have multiple comorbidities, or are at significant risk of developing functional limitations (3). Recent French guidelines include the option of remote rehabilitation via telecare for physiotherapy at home (4).
In Tokyo, Japan, a densely populated city, the number of COVID-19 patients has been increasing since the beginning of April 2020. At the end of May 2020, the total number of COVID-19 patients reached 15,341, with 14,447 survivors and 894 deaths. Tokyo Medical and Dental University, located in the centre of Tokyo, started accommodating COVID-19 patients on 2 April 2020, a few days before the Japanese
government declared a nationwide state of emergency due to the SARS-CoV-2 outbreak on 7 April 2020. The hospital’s role was to treat moderate-to-severe COVID-19 patients requiring oxygen supplementation and intensive care interventions, including intubation, haemodynamic monitoring, and extracorporeal membrane oxygenation (ECMO). Initially, it was planned to provide late-phase rehabilitation only for COVID-19 survivors, in order to avoid hospital-acquired infections and to save on personal protective equipment (PPE), given the prospect of an increase in COVID-19 cases, as observed in other countries. However, 2 cases of pulmonary embolism caused by hypercoagulability and hyperinflammation (4–6) due to SARS-CoV-2 infection occurred immediately after the hospital began accommodating patients; thus, it was decided to start providing early rehabilitation for COVID-19 patients. The aim was to improve respiratory function, and counteract immobilization, which could lead to decreased muscle strength, insufficient sputum drainage, increased risk of deep vein thrombosis or pulmonary embolism, and neuropsychological issues; and promote the recovery of ICU survivors from critical illness (7, 8). Remote or direct (hands-on) rehabilitation delivery of rehabilitation was initiated, with exercises aimed at developing strength, endurance, range of motion, and flexibility.
To minimize contact with COVID-19 patients, in terms of distance and duration, a remote rehabilitation modality was devised using an i-pad.
The aim of this study was to describe the effectiveness and risk management of remote rehabilitation for COVID-19 patients.
Study setting
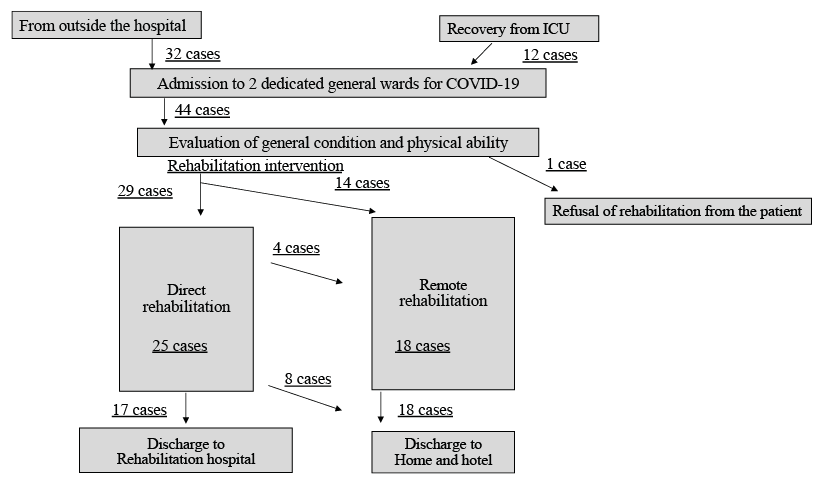
Tokyo Medical and Dental University is a general acute care hospital with 814 beds. The hospital prepared 2 dedicated general wards and an ICU for patients with a confirmed diagnosis of COVID-19 (Fig. 1). The diagnosis of COVID-19 was made in Japanese Public health centres prior to, or after, admission to the hospital, using a polymerase chain reaction (PCR) device. Asymptomatic patients with previously mild and currently few signs of pneumonia on computed tomography, patients with mild symptoms requiring no oxygen therapy, and patients with severe symptoms requiring oxygen therapy (up to 5 l/min) were accommodated in the general wards. Asymptomatic patients and those with mild symptoms were followed up with X-ray examinations, blood tests, and PCR tests to monitor the disease course. Patients with deteriorating X-ray findings, those whose previously mild symptoms worsened, and those with severe symptoms requiring oxygen therapy (up to 5 l/min) were administered favipiravir. This anti-influenza drug was unauthorised for use in SARS-CoV-2 infection and was administered only when patients’ informed consent was obtain-ed, due to the drug’s teratogenic effects. Those whose previously mild symptoms worthened also received Ciclesonide (Alvesco®), an inhaled corticosteroid used in patients with asthma, together with conventional oxygen therapy. In patients with hypercoagulability, anti-coagulants (internal use of rivaroxaban or intravenous administration of heparin) were provided according to D-dimer and C-reactive protein (CRP) levels. D-dimer levels were measured using a CS-5100 automated coagulation analyser (Sysmex Corporation, Kobe, Japan), and CRP levels were measured using LABOSPECT (Hitachi High-Tech Corp., Tokyo, Japan). Patients requiring oxygen therapy (> 5 l/min) were accommodated or transferred to the ICU for intubation, respiratory management, and intensive care. Survivors were transferred from the ICU to the general ward as soon as their respiratory condition recovered following extubation or ECMO treatment. During admission from outside the hospital or from ICU to the COVID-19 general wards (which were in an isolated area) a rehabilitation doctor recommended rehabilitation therapy in accordance with the exclusion criteria on the day of admission, evaluating each patient’s general status and physical activity and prescribing either remote or direct-contact rehabilitation with assistance.
In the COVID-19 general wards, 4 Wi-Fi-connected iPad® terminals were installed (2 in the infected red zone; 2 in the clean green zone) for communication between a physical -therapist in the clean nurses’ station (green zone) and a patient or nurse wearing PPE in the patient’s room (red zone). Using tablets, the physical therapist in the green area could see a full-body view of the patient and talk with them. Remote rehabilitation was provided for patients in the red zone, with the physical therapist in the green zone, using the iPad video and audio link.
The patient’s oxygen saturation (SpO2) and heart rate were monitored using an SpO2 oximeter placed on their finger, and was performed irrespective of the patient’s condition and phys-ical performance. In order to minimize contact between staff and patients, electrocardiography (ECG) and blood pressure monitoring were not performed. A short rest of approximately 1 min was allowed between each exercise to monitor vital signs. Remote rehabilitation aimed to reduce the duration of stay in the red area for staff, including nurses. Therefore, the criteria for remote rehabilitation were as follows: independent standing; light squatting without heart fluttering; no oxygen therapy, SpO2 ≥ 94%; no comorbidities, including uncontrolled arrhythmia or blood pressure; able to follow orders (no alteration in con-sciousness level or delirium); and provided consent to undergo remote rehabilitation.
Fig. 1. Flow chart of the selection of patients with coronavirus disease (COVID-19) undergoing rehabilitation. ICU: intensive care unit.
If a patient did not meet the criteria for remote rehabilitation, direct rehabilitation was performed with the assistance of phys-iotherapists, together with ECG or blood pressure monitoring when needed.
There was no difference in the accuracy or the programme of rehabilitation between remote and direct rehabilitation, although, in remote rehabilitation, the patients and physiotherapist were not in the same space. Both types of rehabilitation included therapeutic muscle and aerobic exercises. In direct rehabilitation, activities of daily living (ADL) exercises were sometimes included depending on the patients’ activity levels, and patients occasionally needed body-to-body assistance from physiotherapists. When the physical ability of patients undergoing direct rehabilitation improved such that they met the criteria for remote rehabilitation, they were switched to remote rehabilitation.
Rehabilitation therapy was started immediately, based on the patient’s general condition. The exclusion criteria were: patients in whom the associated rehabilitation therapy would severely aggravate their condition; and patient refusal. As the cancellation criteria, the ”Guidelines for Safety Management and Promotion”, set out by the clinical practice guidelines committee of the Japanese Association of Rehabilitation Medicine were used to evaluate the patient’s general condition (Table I) (9, 10).
Table I. This is Japanese criteria of cancellation of daily rehabilitation at the start or the during the re-habilitation therapy
Each remote rehabilitation session lasted approximately 20 min. In patients with low ADL undergoing direct rehabilitation, 2 daily sessions were sometimes necessary.
Rehabilitation was continued in the isolation area until discharge. Patients were directly discharged from the COVID-19 isolation wards when they had recovered from COVID-19 symptoms and required no specific medical care, regardless of the necessity for rehabilitation. Patients who could walk independently with sufficient ADL at that point were discharged home or to a hotel. Patients who tested negative for SARS-CoV-2 twice after recovery from COVID-19 symptoms could return to their homes. Those who tested positive for SARS-CoV-2 after recovery from COVID-19 symptoms were discharged to a hotel, and those who could not walk stably and had insufficient ADL at that point were discharged to another hospital specialised for rehabilitation.
Patients
To evaluate the effectiveness and safety of remote rehabilitation for COVID-19 patients, all consecutive COVID-19 patients undergoing rehabilitation in the general COVID-19 wards from 24 April to 24 May 2020 in Tokyo Medical and Dental University were assessed. Data were collected regarding: number of patients, age, sex, results of PCR at start of rehabilitation and at discharge, rehabilitation modality (remote or direct), cases transferred from direct to remote rehabilitation, need for intubation or ECMO therapy, severity of pneumonia (light: not requiring oxygen therapy; moderate: requiring oxygen therapy < 5 l/min; severe: requiring oxygen therapy > 5 l/min and intubation), oxygen therapy at the start of rehabilitation, peak level or level of D-dimer and CRP at the start of rehabilitation, complications, and outcome. Mobility scores on level surfaces and total scores of the Barthel Index were measured at the start of rehabilitation and again at discharge. It was not possible to measure the patients’ ability to use stairs, as there were no stairs in the COVID-19 wards; thus, the maximum Barthel Index score of 90 points was used. In post-intubated patients, the duration of ICU stay, intubation, and ECMO were assessed.
The Mini-Mental State Examination was not performed, as this requires prolonged contact with patients. Instead, the patients’ level of consciousness was assessed using the Glasgow Coma Scale, grading eye opening (E), verbal response (V), and muscle response (M).
Clinical outcomes were: destination after discharge, PCR results, mobility scores on level surfaces, and Barthel Index total scores. On discharge home or to a hotel, where rehabil-itation therapy was no longer provided, or on discharge to a different hospital, where rehabilitation therapy was contin-ued, physiotherapists provided all patients with voluntary exercises.
Statistical analysis
Patients were divided into remote and direct rehabilitation groups. Patients who were switched from direct to remote rehabilitation were included in the remote rehabilitation group. The χ2 test was used to compare the following categorical variables between the 2 groups: sex, oxygen supply, pneumonia, outcome, and intubation. The Mann–Whitney U test was used to compare the numerical variables between the 2 groups: age, peak level and level of D-dimer and CRP at start of rehabilitation, Barthel Index, time from disease onset to start of rehabilitation, admission to rehabilitation, and rehabilitation duration. The Kolmogorov–Smirnov test was used to assess the assumption of normal distribution and homogeneity of variance between the 2 groups before the Mann–Whitney U test. No regression analysis was performed, as the sample size was small. All statistical analyses were performed using Bell Curve for Excel 2016 (Social Survey Research Information Co., Ltd, Tokyo, Japan). Statistical significance was set at p < 0.05.
Ethical considerations
This study was approved by the research ethics committee of Tokyo Medical and Dental University (M2018-073) and conducted in accordance with the World Medical Association Declaration of Helsinki.
No patients had impaired judgement at the time of admission, but they identified a family member to give consent on their behalf, as written consent was not obtained from the patients due to the risk of virus transmission. Written informed consent was obtained by post from the family member whom the patient selected as the key person or guardian (guardian), as no visitors were allowed. In Japan, digital signatures were not considered legally binding at the time of this study.
Of the 44 patients hospitalized in the COVID-19 wards, 43 (31 men, 12 women) underwent rehabilitation (Fig. 1, Table II), with one male patient declining the rehabilitation intervention. Twenty-two patients were previously treated at home: 12 were transferred from the COVID-19 ICU and 10 were transferred from nursing homes or long-stay hospitals due to nosocomial infections. All patients were fully con-cious (Glasgow Coma Scale score E4V5M6), except for 2 patients with a Glasgow Coma Scale score of E4V4M6, and all patients could follow instructions.
Table II. Characteristics of patients with COVID-19
Of the 43 patients who underwent rehabilitation, 18 (12 men, 6 women) underwent remote rehabilitation. There were significantly more men than women in the whole cohort, but the ratio of men and women was not significantly different between the remote and direct rehabilitation groups. The mean age of all patients was 65 years; patients in the remote rehabilitation group were significantly younger than those in the direct rehabilitation group (56 vs 72 years; p < 0.001). The direct rehabilitation group included one patient with an incomplete spinal cord injury, one with osteoarthrosis of the knee, one with atrial fibrillation, one with cerebral infarction, and one receiving haemodialysis. Four patients were transferred from direct rehabilitation to remote rehabilitation during the study period on the basis of increased muscle strength and weaning from oxygen therapy.
No further cognitive assessments were performed in the isolation area. Twelve patients required intubation (Table III), 3 of whom belonged to the remote rehabilitation group. In the direct rehabilitation group, 1 patient who required ECMO survived. The patients’ mean duration of ICU stay was 14 (range 9–31) days, and the mean time interval of transfer from the ICU to the general ward was 3 (range 2–9) days after extubation. The mean total score of the Barthel Index at the start of rehabilitation was 75 (range 0–90); the remote and direct rehabilitation groups had mean scores of 90 (all patients obtained 90 points) and 40 (range 0–85), respectively. The mobility score (on level surfaces) at the start of rehabilitation was 10 (range 0–15); the remote and direct rehabilitation groups scored 15 (all patients obtained 15 points) and 5 (range 0–15), respectively. The mean Barthel Index score at discharge was 75 (range 0–90); the remote and direct rehabilitation groups had mean scores of 90 (all patients obtained 90 points) and 70 (range 0–90), respectively. The mean mobility score on level surfaces at discharge was 15 (range 0–15); the remote and direct rehabilitation groups had mean scores of 15 (all patients obtained 15 points) and 10 (range 0–15), respectively. In the Barthel Index, the remote rehabilitation group had significantly higher scores than the direct rehabilitation group, both in total mobility and mobility on level surfaces.
Table III. Patients with COVID-19 requiring intubation in the intensive care unit
Results of PCR testing for SARS-CoV-2 were positive in 38 patients at the start of rehabilitation; 14 were still positive at the time of hospital discharge. Of the 43 patients who underwent rehabilitation, 12 were critical and required ventilation, 22 had severe symptoms and required oxygen therapy, and 9 were asymptomatic or had mild symptoms. In the remote rehabilitation group, 3 were critical and required ventilation, 12 had severe dyspnoea and required oxygen therapy (up to 5 l/min), and 3 were asymptomatic; these frequencies were not significantly different between the 2 groups.
Peak D-dimer and CRP levels in blood tests -throughout the course and D-dimer levels at the start of rehabilitation were significantly different between the 2 groups.
Of the 43 patients, 26 (all 18 in the remote rehabilitation group and 8 in the direct rehabilitation group) were discharged home or to a hotel upon recovery from COVID-19 symptoms (Table IV). Each patient had a mobility score of 15 (10–15) at discharge, and their total score was 90 (80–90). Seventeen patients were transferred to a rehabilitation hospital due to a decreased recovery of ADL. Their mobility scores at discharge were 5 (0–10), and their total score was 70 (40–85). Of the 25 patients in the direct rehabilitation group, 10, who were from the nursing homes or long-stay hospitals and who were initially unable to walk, remained unable to walk after the rehabilitation. Their mobility scores at discharge were 5 (0–10) and their total score was 5 (0–25). Twelve patients who could previously walk were unable to walk stably until their symptoms disappeared. These patients were all from the ICU ward and were transferred to the isolation wards after extubation. Their mean mobility score at the start of rehabilitation was 5 (0–10), and mean total score 40 (30–60). The mean mobility score at discharge was 10 (5–10), and the total score at discharge was 70 (40–85). There were no serious adverse events, including deep venous thromboses, pulmonary emboli, arrhythmias, hypertension or hypotension, and falls, in any of the rehabilitation groups during the study period. No cases of acute tubular necrosis were found.
Table IV. Barthel Index at discharge
Of 43 COVID-19 patients who underwent rehabilitation, 88.4% tested positive for SARS-CoV-2 at the start of rehabilitation, with the rate decreasing to 32.6% at discharge. PCR testing for SARS-CoV-2 was performed regularly during the disease course, and patients were kept in dedicated COVID-19 wards until their discharge, even if PCR testing for SARS-CoV-2 during their hospital stay was negative.
Firstly, early remote rehabilitation was performed in 32.6% of cases using Wi-Fi-connected iPads® to establish communication between the patient’s bedside and the physical therapist, who stayed outside the contaminated area. In addition, 4 patients were transferred from direct to remote rehabilitation when their mobility scores on a level surface improved to the maximum possible score. Therefore, 41.9% of the patients finally received remote rehabilitation. Remote rehabilitation minimizes contact with COVID-19 patients in terms of frequency of staff entering the red zone and their duration of stay in the red zone, which could prevent transmission of infection and reduce the amount of PPE needed. In fact, in our hospital, PPE supply was relatively abundant because the number of COVID-19 patients did not increase as much in Japan as in the USA or Europe (11).
In order to safely continue providing rehabilitation for COVID-19 patients and other patients simulta-neously, it was important that the therapy teams should not overlap. They were divided into 2 groups to prevent nosocomial infections. In the case of nosocomial infections, contacts were to be traced, regardless of the limitations of the physiotherapy and rehabilitation staff workforce. Using a mobile terminal, rehabilitation could be delivered remotely, either by therapists in the COVID-19 team or by therapists who do not belong to the COVID-19 team. This regime minimized contact and PPE use.
The patients’ mean age was significantly lower in the remote rehabilitation group. The mobility score on a level surface at the start of rehabilitation was 15 in the remote rehabilitation group. The ability to stand up stably without heart fluttering during squatting was required as the criterion for initiating remote rehabilitation. Elderly patients did not have this ability; thus, they only met the criteria for direct rehabilitation.
In the current study, men outnumbered women. However, the rate of remote rehabilitation did not vary by sex. Previous reports have shown that male sex is a risk factor for severe COVID-19 (12–15), which is consistent with the data in the current study.
Peak D-dimer and CRP levels and D-dimer levels at the start of rehabilitation were significantly higher in the direct rehabilitation group. Moreover, the most severe cases belonged to the direct rehabilitation group.
The Barthel Index of all patients increased or re-mained at 90 after rehabilitation, although they remained isolated in private rooms, except for 2 patients with a score of zero at the start of rehabilitation. The mobility scores of patients who were transferred to the rehabilitation hospital after discharge did not reach 15 or remained low at discharge. The patients who could walk before the SARS-CoV-2 infection and were discharged to the rehabilitation hospital were all from the ICU wards, after intubation, and had a very low mobility index at the start of rehabilitation. Both mobility and total Barthel Index scores improved, although a longer duration of rehabilitation was necessary for independent walking, which was needed before patients were discharged home or to a hotel. The Barthel Index did not increase in 10 institutionalized or hospitalized patients living in long-stay hospitals, who could not walk before the SARS-CoV-2 infection. These patients returned to the nursing home or long-stay hospitals, or were provided with appropriate home services before discharge home.
No serious adverse events were noted in either rehabilitation group during the study period. Risk management is extremely important in remote rehabilitation. One severe complication to be avoided is falls. Without the assistance of a doctor or a physical therapist, patients are at risk of falls, which may cause fractures of the lower extremity requiring immediate surgery. Also, from the viewpoint of infection transmission and possible nosocomial infections, it is difficult to transfer COVID-19 patients to the clean zone of the operating room. Two oxygen therapy-free patients who could stand stably from the remote rehabilitation group were excluded because of knee pain and the past history of cervical cord injury, respectively.
During remote rehabilitation, SpO2 and heart rate were monitored remotely, but ECG and blood pressure measurements were not monitored. The aim of remote rehabilitation was to reduce the risk to, or duration of, medical and nursing staff exposure to the infection (red) zone. Nurses were therefore not permitted to perform ECGs or to measure blood pressure; they only monitored vital signs daily on the patients’ medical charts. Therefore, patients with arrhythmia, ischaemic disease, hypertension or hypotension should be excluded from remote rehabilitation. For 2 oxygen therapy-free patients who could stand stably, general rehabilitation was selected because they had atrial fibrillation and hypotension. A wearable device placed in the earlobe that could check the SpO2 levels and heart rate from maxillomandibular bone conduction was used to improve patient monitoring during remote rehabilitation. ECG monitoring was not done, as this cannot be set up by the patient. Although ECG and blood pressure monitoring by a nurse with PPE is available and meaningful, risk management of arrhythmia or significant changes in blood pressure is difficult when using remote rehabilitation from the clean zone. In this study, in order to reduce contact between the nurses and the patients, the criteria for remote rehabilitation were set and ECG and blood pressure were not monitored.
No symptomatic pulmonary embolism was observed after starting the rehabilitation programme. Anti-coagulant therapy was administered after 2 cases of pulmonary embolism were experienced immediately after the hospital began to accommodate patients. In patients with hypercoagulability, anti-coagulants (oral rivaroxaban 10–15 mg/day or continuous intravenous heparin treatment 10,000–20,000 U/day) were provided according to D-dimer and CRP levels. The effect of rehabilitation to its hypercoagulability. The bias are multilpe elements to the effect to the hypervcoagulability: the use of coagulants, its amount, the initial D-dimer or the severity of COVID-19 infection. Nevertheless, rehabilitation is recommended because patients experienced general malaise and dyspnoea, regardless of the presence or absence of hypercoagulability (16).
Remote rehabilitation may be effective even during isolation at home or in a hotel. In Japan, some hotels were rented by the government to accommodate -COVID-19 patients with no or mild symptoms, in order to prevent transmission of infection to their families, while not occupying hospitals or aggravating their medical condition.
Considering the high risk of infection transmission, nosocomial infections, and the global shortage of medical resources, including PPE, physicians, nurses, physiotherapists and other rehabilitation staff, it is understandable that the physiotherapy guidelines do not recommend providing interventions for moderate-to-severe COVID-19 patients. However, if medical resources are available, physiotherapy should be considered for all COVID-19 patients, regardless of disease severity. Remote rehabilitation could be an option for preventing pulmonary embolism in patients with mild disease who do not require therapy or those who can fully perform ADL. Rehabilitation tools must be developed in preparation for a possible second wave of SARS-CoV-2 infection. If COVID-19 patients in the second wave far outnumber those in the first wave in Japan, they will not be managed in the hospital, as one-to-one remote rehabilitation can be provided, and multiple deliveries can be performed, using monitoring devices. Preparation of such devices is necessary in readiness for the next phase.
Today, many people have access to the internet and most have smartphones. Remote work via video, Facetime and Skype, etc. is also common. In the near future, not only for a second wave of SARS-CoV-2 infection or for other infectious diseases, but also for patients in remote locations who have limited access to medical care services in hospital, this remote rehabilitation programme will enable physio-therapy to be provided interactively via devices using multiple delivery systems, with vital sign monitoring, including blood pressure or ECG. Remote rehabilitation is therefore a promising modality for expansion in Japan and other countries, using modified communication tools.
Study limitations
This study has several limitations. It is a single-centre, retrospective, observational study. A longer study is needed to further validate the effectiveness and safety of remote rehabilitation in COVID-19 patients. Although only a small number of patients were analysed, the study is clinically meaningful, as it investigated the characteristics of COVID-19 patients. The lessons regarding the urgent need for rehabilitation should be shared rapidly, given the prospect of a second wave of COVID-19. Long-term follow-up of patients undergoing remote rehabilitation and of COVID-19 patients undergoing rehabilitation is necessary. This study did not measure the duration from the start of infection, because the course of COVID-19 varies and our cases included those with mild to severe symptoms. Finally, COVID-19 data vary by country, region, and governmental policy.
Conclusion
In conclusion, 41.9% of rehabilitation therapies in dedicated COVID-19 wards were delivered by remote rehabilitation. No serious adverse events were observed. With modified communication tools, remote rehabilitation is promising for providing rehabilitation in various situations in the near future, including cases with a high risk of infection or those that can be treated at a distance, such at home or in remote locations.
The authors sincerely thank all doctors at the Trauma and Acute Critical Care Medical Center and the Department of Integrated Pulmonology, Tokyo Medical and Dental University, for their dedication in treating COVID-19 patients.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize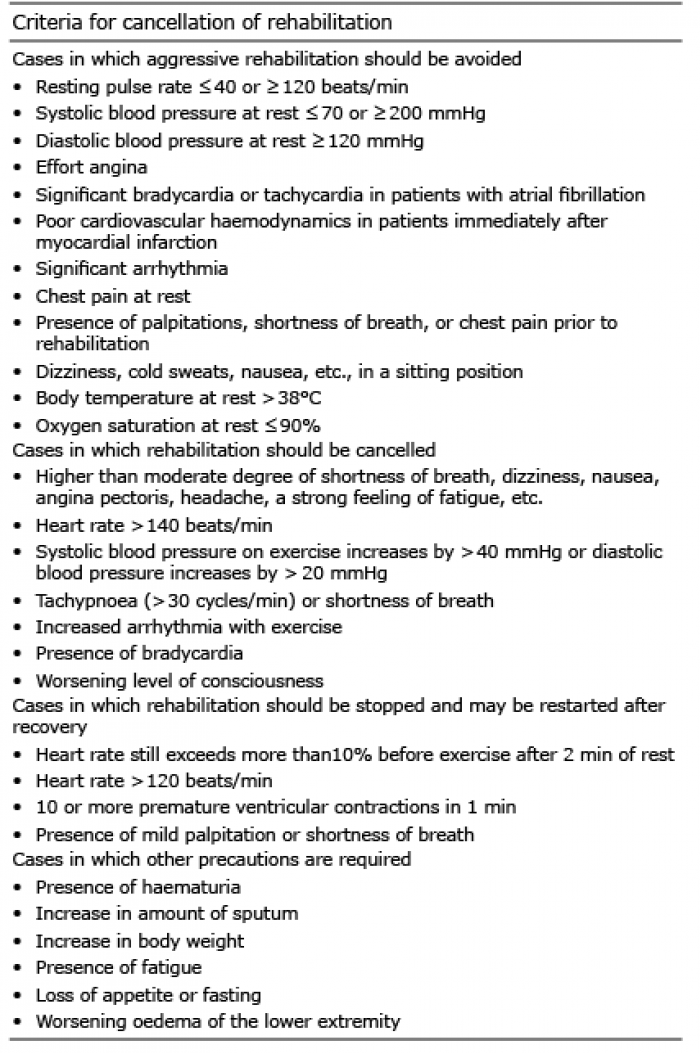 Click to show fullsize
Click to show fullsize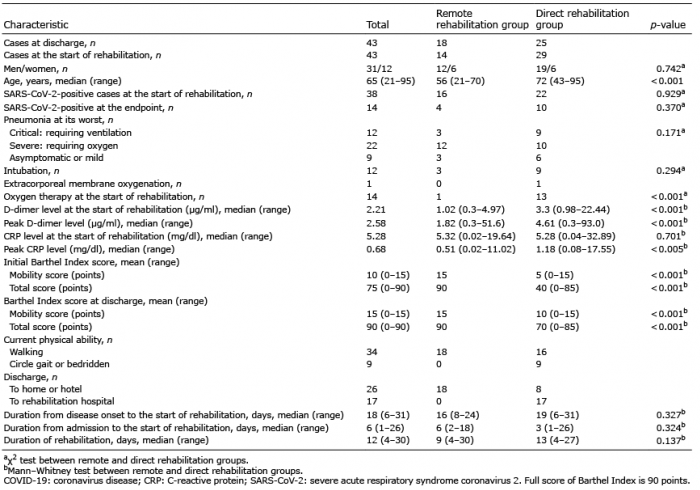 Click to show fullsize
Click to show fullsize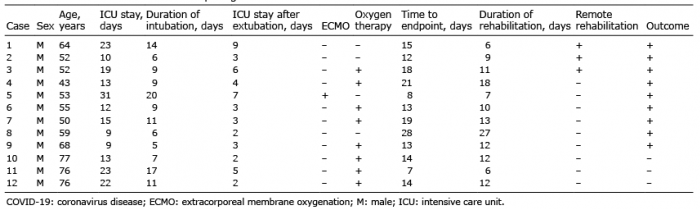 Click to show fullsize
Click to show fullsize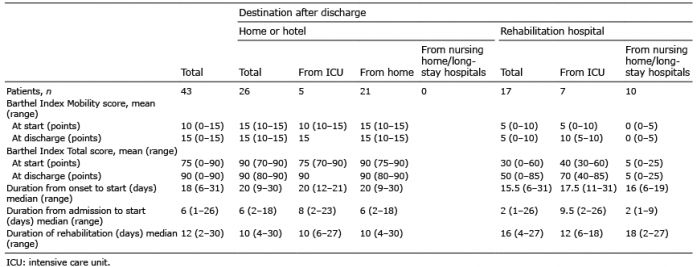 Click to show fullsize
Click to show fullsize