
From the 1Department of Cardiology, Wuhan Fourth Hospital, Puai Hospital, Tongji Medical College, Huazhong University of Science and Technology, Huazhong University of Science and Technology, Wuhan, 2School of Chemistry and Chemical Engineering, Guangzhou University, Guangzhou , 3Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, 4Department of Ultrasound, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 5Department of Rehabilitation, The First Affiliated Hospital of Jinan University, Guangzhou and 6Department of Rehabilitation, Wuhan Fourth Hospital, Puai Hospital, Tongji Medical College, Huazhong University of Science and Technology, Huazhong University of Science and Technology, Wuhan, China. *These authors contributed equally to this work.
Objective: To investigate the effect of progressive resistance training using resistance (elastic) bands on subacromial bursitis following triamcinolone acetonide injection.
Design: Randomized clinical trial.
Patients: A total of 68 patients with subacromial bursitis were randomized to a triamcinolone acetonide group or a triamcinolone acetonide plus resistance band training group.
Methods: Visual analogue scale, Constant scores, range of motion, proprioception, and muscle strength were evaluated at pretreatment and at 3, 12 and 24 weeks’ follow-up. Re-treatment ratio was calculated at one-year follow-up.
Results: At 3 and 12 weeks, both the triamcinolone acetonide group and triamcinolone acetonide plus resistance band training group showed a significant improvement in Visual analogue scale score, Constant score, range of motion, proprioception and muscle strength. Although the scores in the triamcinolone acetonide group had not increased at 24 weeks compared with baseline, the scores in the triamcinolone acetonide plus resistance band training group showed continued improvement at 24 weeks. A lower proportion of patients in the triamcinolone acetonide plus resistance band training bands group than in the triamcinolone acetonide group had received re-treatment at one-year follow-up (12.1% vs 82.9%).
Conclusion: Progressive resistance training with resistance (elastic) bands has the advantages of extending the benefits of corticosteroid injection and maintaining long-term effects on shoulder function in patients with subacromial bursitis.
Key words: triamcinolone acetonide; elastic band training; resistance band training; subacromial bursitis.
Accepted Sep 23, 2020; Epub ahead of print Oct 12, 2020
J Rehabil Med 2021; 53: jrm00140
Correspondence address: Yu Cai, HanZheng Street 473, QiaoKou District, 430030, Wuhan, China. E-mail: caiy_kf@163.com
Doi: 10.2340/16501977-2752
Subacromial bursitis is characterized by pain and stiffness of the shoulders. Corticosteroid injection is widely used in treating subacromial bursitis; however, with differing views on its long-term effects in preventing shoulder symptoms. Resistance (elastic) band training is commonly used to promote muscle activation during shoulder rehabilitation. The aim of this study was to investigate the effect of progressive resistance training with elastic bands on subacromial bursitis following triamcinolone acetonide injection. Patients with subacromial bursitis were randomized to a triamcinolone acetonide group or a triamcinolone acetonide plus resistance band training group. The triamcinolone acetonide group received triamcinolone acetonide injection only. Meanwhile, the triamcinolone acetonide plus resistance band training group received triamcinolone acetonide injection and resistance band training. At 3 and 12 weeks, both the triamcinolone acetonide group and triamcinolone acetonide plus resistance band training group showed a significant improvement in pain relief, mobility, and muscle strength. A lower proportion of patients in the triamcinolone acetonide plus resistance band training group than in the triamcinolone acetonide group had received re-treatment at the one-year follow-up (12.1% vs 82.9%). Thus, training with resistance (elastic) bands has the advantages of extending the benefits of corticosteroid injection and maintaining long-term effects on shoulder function in subacromial bursitis.
Subacromial bursitis (SB) is one of the most common clinical conditions characterized by anterior shoulder pain and restriction of range of motion (ROM) of the shoulder, which usually occurs during abduction and sometimes during rotation of the shoulder (1).
Corticosteroid injections are widely used to treat shoulder pain in conditions such as rotator cuff disease, bursitis, and adhesive capsulitis, reducing inflammation and relieving pain (2–4). In some clinical studies, corticosteroid injections are defined as an effective short-term treatment and have potential side-effects with repeated injection. A controlled trial investigating the correlation between injection schedule and shoulder benefits found that the therapeutic effect lasted only 6 weeks after the injection and that the clinical improvements disappeared by 12 weeks, with more than half of patients experiencing recurrence of symptoms (5). Similarly, a study of methylprednisolone injection in the treatment of impingement syndrome also showed significant improvement in activities of daily living (ADL) variables and a decrease in sleep-disturbing pain, although these differences disappeared by 3 months (6). In addition, a review by Buchbinder et al. concluded that corticosteroid injection can be beneficial for shoulder pain, although its effect may be slight and temporary (7). In agreement with the above studies, our clinical practice has found that corticosteroid injection alone does not produce long-term benefits. Therefore, the clinical effect of corticosteroid injection in SB requires discussion and reconsideration.
The muscles around the shoulder joint contribute to maintaining shoulder stability. Weakness or imbalance in shoulder muscle strength causes excessive stress on the joint and may lead to changes in shoulder biomechanics and shoulder disease. Muscle strength-training exercises are used to increase muscular development and improve neuromuscular control (8, 9). Progressive resistance training with a gradually increasing load is recommended to achieve neuromuscular activation and muscle strengthening and hypertrophy. Resistance training has been shown to enhance muscle strength and may be important in preventing shoulder injuries (10–12). Elastic bands (EB), a type of resistance training apparatus, can provide variable resistance and allow changes over a range of motions, which can prevent the risk of excessive weight loading during strength-training exercises. In addition, EB can provide efficient resistance and promote high levels of muscle activation for enhancing muscle strength in treating shoulder disease (13–15). Because of their simplicity and their economic and safety advantages, EB are commonly used during rehabilitation programmes and are available in most rehabilitation centres.
Based on the above observations, this study aimed to examine the effect of EB training after triamcinolone acetonide (TA) injection on the treatment of SB. It was hypothesized that resistance training with EB could effectively treat SB with long-term benefits.
Study design
The study was approved by Puai Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China; and informed consent was obtained prior to the study. Ninety patients with SB diagnosed by physical examination (Neer and Hawkins tests) and magnetic resonance imaging (MRI) (findings include bursal thickness > 2 mm, the presence of fluid medial to the acromioclavicular joint or fluid in the anterior aspect of the bursa) were recruited into the study from May 2015 to January 2017. Inclusion criteria were: first-time diagnosis of SB; history of overhead activity for > 2 months; and shoulder pain and ROM limitation for > 1 month. Exclusion criteria were: analgesic medication, physical therapy, or previous injection; history of shoulder trauma; osteoarthritis, rotator cuff tear, subacromial impingement syndrome, and tendinitis of the long head of the biceps brachii; diabetes, cardio-cerebrovascular disease, and history of mental disorders; and concomitant immune inflammatory disease, such as rheumatoid arthritis, systemic lupus erythematosus, or ankylosing spondylitis.
The patients were randomly divided into a TA group and a TA plus resistance band training (TA+EB) group by a simple randomization method using computer-generated random tables. The person giving the injections and the outcome evaluator were blinded to the study. Trial registration: Chinese Clinical Trial Registry ChiCTR1800020421.
Ultrasound-guided injection
Ultrasound (US) examinations and injection guidance were carried out using a LOGIQ E9 (General Electronic Company, Milwaukee, WI, USA) machine. Patients were asked to relax their affected shoulder and maintain a lateral decubitus position on the contralateral side. After disinfecting the probe and patient’s skin with the same disinfectant, a 26-gauge needle was inserted into the subdeltoid bursa between the deltoid muscle and the supraspinatus tendon under US guidance. After aspiration of any effusion, 2 ml (2 mg/ml) of TA (Zhejiang Xianju Pharmaceutical Co., Ltd, China) and 2 ml (2 mg/ml) of lidocaine hydrochloride (Hebei Tiancheng Pharmaceutical Co., Ltd, China) were injected into the subacromial bursa under US guidance.
Resistance band training
The subjects were instructed on all EB training by a professional physical therapist. Before use of the EB (Hygenic Corp. Akron, Ohio, USA), the appropriate EB for each subject was selected. The colour-coded EB have different resistance levels, supplying a different tension force. The EB of appropriate colour was selected as the one with which the patient did not feel pain during resistance training; this was reassessed and adjusted at each session. The initial length of the EB was 1.0–1.5 m, and the tension force was determined at 100% elongation (16). EB training was performed for 9 weeks. The maintained time was 3 s at the end position. All movements were performed at a constant speed. In all repetitions, the joint was moved through the entire maximum tolerated ROM. The EB training programme began with 3 sets of 10 repetitions every day for the first 3 weeks, progressed to 3 sets of 15 repetitions in the fourth week, and extended to 3 sets of 20 repetitions in the seventh week.
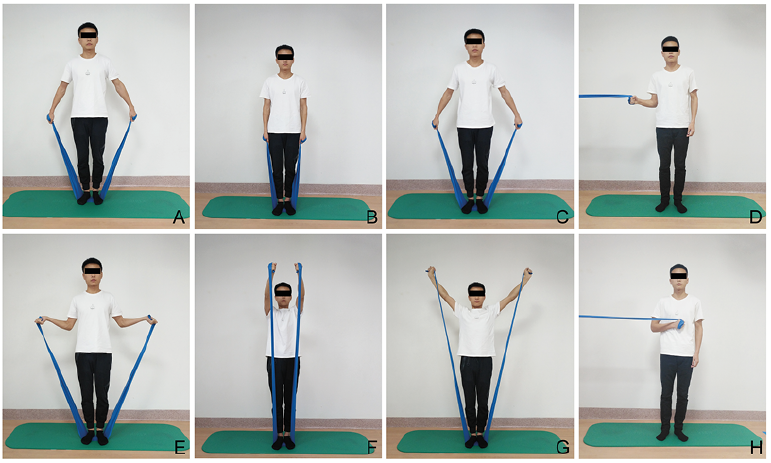
For the external rotation exercise, the start position was 30° abduction; the end position was 30° abduction and 50–60° external rotation, and the elbow bend angle was 90°. For the forward flexion exercise, the start position was 0° abduction and the end position was 150–160º flexion. For the abduction exercise, the start position was 30º abduction; and the end position was 130–140º abduction. For the internal rotation exercise, the start position was 0º abduction and 10º external rotation, and the elbow bend angle was 90º; the end position was 0º abduction and 60–70º internal rotation (Fig. 1).
Fig. 1. Exercises in the resistance band strength-training programme. (A–D) Start positions; (E–H) end positions.
Outcome measures
The primary outcome was evaluated using the Constant and visual analogue scale (VAS) scores. The VAS, ranging from 0 for no pain to 10 for severe pain, was used to evaluate pain during motion. The Constant score was used to assess the functional state of the shoulder (17). The secondary outcome measures were ROM, proprioception, and isometric muscle strength.
Range of motion
The ROM for shoulder rotation was assessed by measuring the degrees of maximum flexion, abduction, internal rotation, and external rotation using a standard goniometer. All measurements were performed 3 times at 1-min intervals, and the results were averaged.
Proprioception
A continuous passive motion (CPM) apparatus was used to evaluate shoulder proprioception for both joint position sense (JPS) and kinesthetic sense (Fig. 2). The shoulder was initially positioned at 90° of abduction, and the elbow was positioned at 90° of flexion. The reference angle in the JPS test was set as 50% of the maximum ROM. Before the JPS test, the participants were given 3 exercises to reproduce the reference angle and become familiar with the testing procedure. Then, the CPM rotated the shoulder at a rate of 1°/s into the internal rotation position from the start position to the joint position previously experienced. When the patient perceived that his/her shoulder had reached the reference position, the actual angle was measured. The error between the reference angle and the actual angle was calculated. The test procedure was repeated 3 times. The kinesthetic sense was detected by measuring the threshold to detection of passive motion (TTDPM). The CPM rotated the shoulder at a rate of 1°/s into the internal rotation position. The patient was asked to push the stop button when movement was first felt. The angle between the initial position and the position at which the patient felt the movement was recorded. All tests were repeated 3 times, and the results were averaged. The order of the test trials was randomized to minimize the effects of fatigue.
Fig. 2. Patient’s position for assessment of joint position sense and kinesthetic sense.
Muscle strength
A hand-held dynamometer was used to assess isometric muscle strength. Shoulder muscle strength was measured in 45° flexion, 45° abduction, and internal and external rotation. All measurements were repeated 3 times at 10-s intervals, and the mean value was calculated. Standardized instructions and verbal encouragement were given.
Follow-up
Outcome measures were evaluated at study entry and at 3, 12, and 24 weeks of follow-up. At the 24-week follow-up, 5 patients were no longer in the study (intolerance, 2 patients; loss to follow-up, 3 patients). At the one-year follow-up, a total of 68 patients (33 in the TA group; 35 in the TA+EB group) were contacted by telephone to determine whether they had undergone further treatments, such as repeated corticosteroid injection, massage, pain medications, or physical therapy, since their last visit (at 24 weeks).
Data analysis
Statistical analyses were completed using SPSS 21.0 (International Business Machines Corporation, Armonk, New York). Baseline differences between groups were analysed by analysis of variance (ANOVA) for continuous data and by the χ2 test for categorical data. Continuous data are expressed as the mean (standard deviation (SD)), and the normality of distribution was tested by a QQ plot. The data were analysed using a paired Student’s t-test and repeated measures analysis of variance (ANOVA). As for repeated measures ANOVA, post-hoc test of p-value was adopted by Bonferroni correction and effect size was expressed as eta-square. A value of p < 0.05 was considered statistically significant. The sample size was calculated based on the Constant score. The SD was established as 3.5 from existing medical records. With a type 1 error rate of 0.05 and a type 2 error rate of 20%, a sample size of 35 patients per group was determined to be sufficient to detect a 20% difference in Constant score at final follow-up.
A total of 90 patients were screened from 2015 to 2017, and 14 patients were excluded because they declined to participate in the study (Fig. 3). Eight (10.5%) patients did not receive the allocated treatment (Fig. 3). Patient data is shown in Table I. No complications occurred in wither group. At the one-year follow-up, 12.1% patients in the TA+EB group and 82.9% patients in the TA group had received re-treatment.
Fig. 3. Study flow diagram. TA: triamcinolone acetonide; EBs: elastic resistance bands.
Table I. Patient data
The Constant and VAS scores were similar between the 2 groups at pretreatment and had a similar downward trend at 3 weeks (Table II). In the TA group, the Constant and VAS scores were significantly improved at 3 weeks, but no change was observed after 3 weeks (Table II). In the TA+EB group, the Constant and VAS scores were significantly improved at 3 weeks and until the 24-week follow-up (Table II).
Table II. Constant score and visual analogue scale (VAS) score
The proprioception and active ROM (flexion, abduction, external rotation, and internal rotation) in both groups was significantly improved at 3 weeks (Tables III and IV). In addition, sustainable increases in proprioception and active ROM were found in the TA+EB group (Tables III and IV). However, no improvement in proprioception and active ROM was observed after 3 weeks in the TA group (Tables III and IV). In the group comparison, after 3 weeks, the proprioception and active ROM in the TA+EB group were noticeably improved compared with those in the TA group (Tables III and IV).
Table III. Range of motion and proprioception
Table IV. Isometric muscle strength
This study demonstrated the following outcomes: (i) in treating SB, a single injection of TA had a short-term effect in alleviating pain and improving shoulder function; (ii) progressive resistance training on the basis of pain alleviation resulted in a persistent effect in preventing the recurrence of SB, and reduced the rates of corticosteroid re-injection and re-hospitalization due to its simplicity and safety.
Injection of corticosteroids into the subacromial bursa allows patients to achieve improved shoulder function and pain relief, but the clinical effects of corticosteroid injection are restricted to a relatively short time-period and are accompanied by various adverse side-effects, including glucose intolerance, osteoporosis, immunosuppression, etc., especially with repeated use (18). The usefulness of corticosteroid injections for the long-term treatment of shoulder diseases has been questioned (5, 19–21). The current results also showed that the greatest therapeutic benefit occurred at the third week after injection and deteriorated thereafter, similar to the results of a previous study of corticosteroid injection in patients with supraspinatus impingement (22).
During the progression of SB, pain and inflammation can impair muscle function, and studies have shown that pain alters muscle recruitment strategies and strength (23). Individuals with SB are at substantial risk of shoulder muscle weakness, which results in shoulder instability and then causes shoulder pain and dysfunction. Indeed, previous studies have shown that exercise can suppress inflammation (24, 25) and improve shoulder function in terms of strength and pain in patients with rotator cuff tears or shoulder impingement (26–28). Thus, in addition to corticosteroid injection for pain relief, exercise is essential to strengthen the shoulder muscles, maintain the ROM and appropriately prevent the recurrence of SB after corticosteroid injection. Progressive resistance training provides efficient improvements in shoulder stability, strength, and motion by neuromuscular activation and muscle strength enhancement (11, 12, 15, 29). As a convenient rehabilitation tool, EB offer resistive force and are beneficial for improving muscle strength and increasing joint stability (30–32). Resistance training with EB, focusing on the shoulder muscles (deltoid, teres minor, supraspinatus, infraspinatus and subscapularis), was carried out in our study and included exercises covering 4 directions: flexion, abduction, external rotation, and internal rotation. In agreement with the results of the above studies, the patients in the current study experienced significant improvement in shoulder muscle strength after 9 weeks of EB training. Moreover, the passive ROM was significantly improved in terms of flexion, abduction, external rotation, and internal rotation at 12 and 24 weeks. In addition, a significant correlation was observed between increased muscle strength and reduction in VAS score in the TA+EB group. The positive relationship between an increase in muscle strength and a reduction in musculoskeletal pain has been reported previously, consistent with the current results (33).
An ideal exercise programme should not only improve muscle strength, but also proprioception. Studies have proven that proprioception is essential to joint stability during daily activities and that deficits can be a mechanism of shoulder instability and shoulder disease (14). The results of the current study support the current clinical practice of strength training to improve proprioception deficits in patients with shoulder disease (34, 35). Based on the principle of resistance training, we believe that the EB generated a consistent and controlled force that could be customized to the needs of the patient to provide both a resistive force for exercise and a suitable stretch. This progressive resistance training allows repetitive stimulation of the articular mechanoreceptors and Golgi tendon organs, which may modify the sensitivity of the muscle spindle, muscle length, and sensors (36–38). These adaptions are responsible for enhanced proprioception, resulting in better detection of position (36–38).
Study limitations
A limitation of this study is the difficulty of selecting the most appropriate EB, due to their characteristics; for instance, the various lengths, strain rates, repetitions, cyclic loading, or preconditioning of the tubing. We believe that quantification of the resistance properties of the material is important, because inappropriate use of the material could be harmful. Excessive force, torque, or pressure may cause inflammation, scarring, or deformity; insufficient force may prevent the patient from reaching their full rehabilitation potential. In addition, by comparing different frequencies per week or treatment cycle for this intervention strategy, clinicians may be able to develop more efficient rehabilitation strategies with this rehabilitation tool.
Another limitation of this study is that resistance training includes variables related to the magnitude of force, moment arm, and angle between the moving segment and the direction in which the resistance is acting. Although the subjects were instructed to perform slow, controlled movements, it is possible that they accelerated the limb, thus placing additional inertial strain on the gauge and inflating the recorded values. We believe that the control of exercise intensity is key to ensuring the safety and efficacy of physical activity in any context, including athletic, recreational, and therapeutic settings. Furthermore, whether patients have underlying shoulder diseases, such as impingement syndrome, rotator cuff tendinopathy, or bicipital tendinitis, should also be considered.
Conclusion
In conclusion, resistance training has the advantages of extending the short-term benefit of corticosteroid injection and maintaining long-term effects on pain relief and the enhancement of shoulder function in patients with SB. This study showed that the incremental resistance training exhibited a “dose response” effect on alleviating joint pain, i.e. the more exercise was performed (with an appropriate recovery period) the greater was the improvement in pain. In addition, progressive loading appears to be more effective than other loading schemes for long-term muscular strength training (39). Accordingly, pharmacological suppression of inflammation and pain prior to exercise may enhance the effect of the exercise. In addition, exercise may suppress inflammation and exert additional effects on the pharmacological treatment of inflammation (25, 40).
The authors thank Jinyun Pu, Department of Pediatrics, Tongji Hospital, Huazhong University of Science and Technology, and Ruoyu Zhao, Department of Anesthesiology, University of Mississippi Medical Center, for advice on the article.
Funding. This study was funded by National Natural Science Foundation of Wuhan (grant numbers WX18Q21 and WX19Q24); Health commission of Hubei Province scientific research project (number WJ2019H371); The National Natural Science Foundation of Hubei (numbers 2019CFB806 and 2018CFB568); The National Natural Science Foundation of China (number 81701716).
Ethical approval. All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize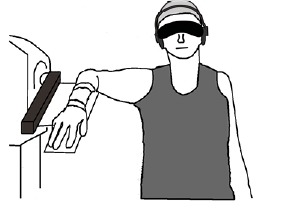 Click to show fullsize
Click to show fullsize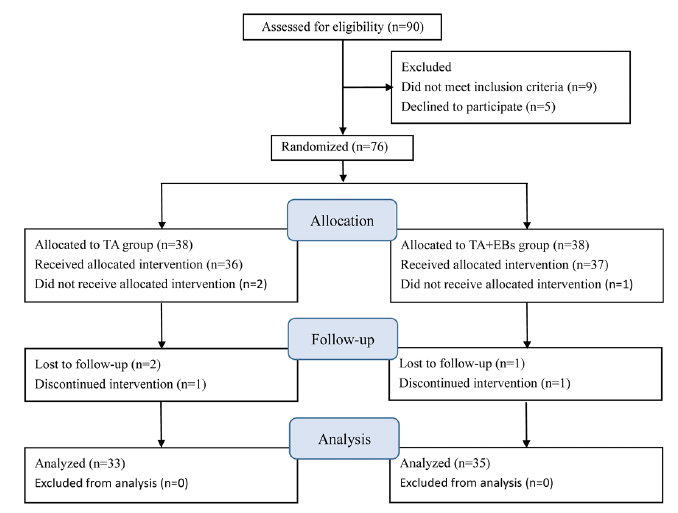 Click to show fullsize
Click to show fullsize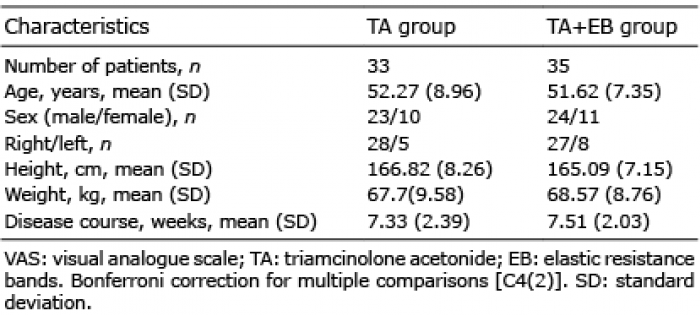 Click to show fullsize
Click to show fullsize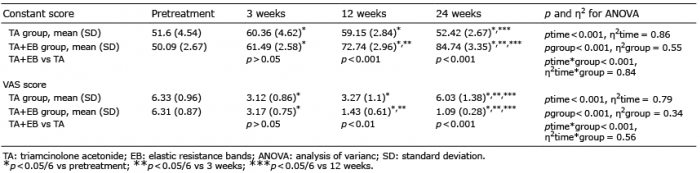 Click to show fullsize
Click to show fullsize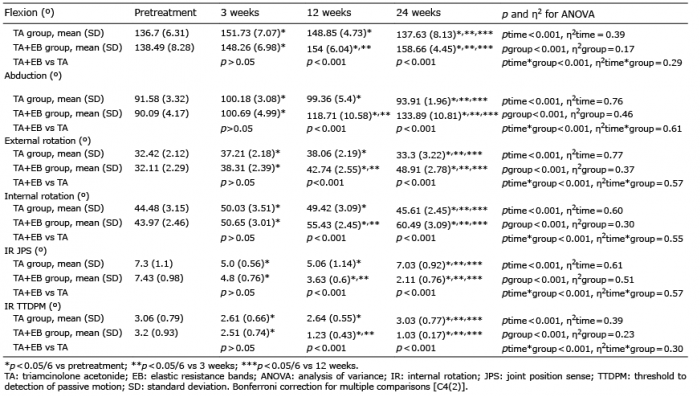 Click to show fullsize
Click to show fullsize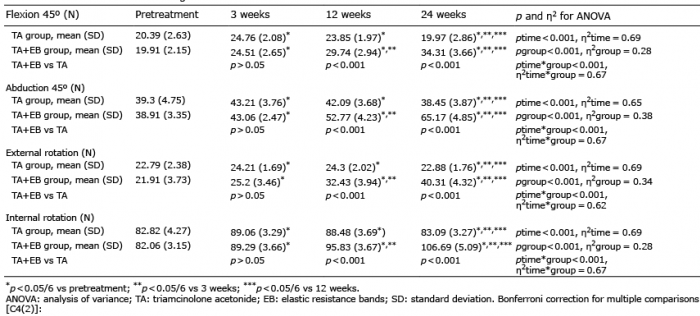 Click to show fullsize
Click to show fullsize