
From the 1University of Texas Health Science Center McGovern Medical School, Department of Physical Medicine and Rehabilitation, and The Institute for Rehabilitation and Research (TIRR) Memorial Hermann Hospital, Houston, Texas, USA, 2Department of Adaptive Physical Training, Ural University of Physical Education, Sverdlovsk regional hospital for war veterans. Yekaterinburg, Russia, 3Department of Rehabilitation Medicine, The Walton Centre National Health Service Trust, Lower Lane, Liverpool, UK, 4Raymond Poincaré Hospital, Assistance publique - Hôpitaux de Paris, University of Versailles Saint-Quentin, Garches, France, 5Service of Neuropsychology and Neurorehabilitation, Department of Clinical Neurosciences, Lausanne University Hospital (CHUV), Lausanne, Switzerland, 6Medecine Physique & Readaptation, Centre Hospitalier Universitaire UCL Namur site Godinne, Yvoir, Belgium, 7Libra Rehabilitation & Audiology, Eindhoven, The Netherlands, 8JFK-Johnson Rehabilitation Institute, New Jersey, USA, Rutgers – Robert Wood Johnson Medical School, Hackensack Meridian Health School of Medicine at Seton Hall University, New Jersey, USA, 9Nantes Université, Centre Hospitalier Universitaire de Nantes, Movement - Interactions – Performance (MIP), Nantes, France, 10Alcoitão Medical Rehabiliation Centre, Rua Conde Barão, Alcabideche, Portugal, 11Medical College of Wisconsin, Department of Physical Medicine and Rehabilitation, Milwaukee, Wisconsin, USA, 12Valduce Hospital ”Villa Beretta” Rehabilitation Center, Costa Masnaga, Italy, 13Physical Medicine & Rehabilitation Department, La Paz University Hopital, Madrid, Spain, 14Weill Cornell Medicine, New York, USA, 15Department of Medicine, Division of Physical Medicine and Rehabilitation, University of British Columbia, Vancouver BC Canada , 16Rehdo Rehabilitation Centre, Gothenburg, Sweden, 17Joe R. & Teresa Lozano Long School of Medicine at UT Health San Antonio, San Antonio, Texas, USA, 18Medical University of South Carolina Health Rehabilitation Hospital of Charleston an Affiliate of Encompass Health, Medical University of South Carolina, Charleston, South Carolina, USA and 19Neurological Rehabilitation and Physical Therapy, Vivantes Hospital Spandau, Berlin, Germany
This consensus paper is derived from a meeting of an international group of 19 neurological rehabilitation specialists with a combined experience of more than 250 years (range 4–25 years; mean 14.1 years) in treating post-stroke spasticity with botulinum toxin A. The group undertook critical assessments of some recurring practical challenges, not yet addressed in guidelines, through an extensive literature search. They then discussed the results in the light of their individual clinical experience and developed consensus statements to present to the wider community who treat such patients. The analysis provides a comprehensive overview of treatment with botulinum toxin A, including the use of adjunctive therapies, within a multidisciplinary context, and is aimed at practicing clinicians who treat patients with post-stroke spasticity and require further practical guidance on the use of botulinum toxin A. This paper does not replicate information published elsewhere, but instead aims to provide practical advice to help optimize the use of botulinum toxin A and maximize clinical outcomes. The recommendations for each topic are summarized in a series of statements. Where published high-quality evidence exists, the recommendations reflect this. However, where evidence is not yet conclusive, the group members issued statements and, in some cases, made recommendations based on their clinical experience.
Key words: spasticity; botulinum toxin; consensus guideline.
Accepted Sep 29, 2020; pub ahead of print Oct 15, 2020
J Rehabil Med 2021; 53: jrm00134
Correspondence address: Gerard E. Francisco, McGovern Medical School, Department of Physical Medicine & Rehabilitation, TIRR Memorial Hermann Hospital, Physical Medicine and Rehabilitation, Houston, USA. E-mail: gerard.e.francisco@uth.tmc.edu
Doi: 10.2340/16501977-2753
A group of doctors from around the world, who are experts in treating muscle stiffness and spasm (also called spasticity), reviewed the current scientific evidence supporting the effectiveness of using botulinum toxin injections in treatment of spasticity that results from a stroke. When evidence is not available, they discussed and agreed on the best way to treat spasticity using botulinum toxin. The recommendations made by these expert doctors can be used by less-experienced doctors as a guide to how best to use botulinum toxin injection in treating spasticity after a stroke.
Botulinum toxin A (BoNT-A) has been in clinical use for treating post-stroke spasticity for approximately 30 years and is the accepted standard of care for focal post-stroke spasticity (1). It is currently known that BoNT-A treatment is safe and effective for use in both upper and lower limb spasticity, where it can result in both active and passive functional gains (2). Furthermore, BoNT-A is a first-line pharmacological treatment in the management of post-stoke focal and multi-focal spasticity, which, along with a multidisciplinary team (MDT) approach, should be part of a rehabilitation programme to promote optimal clinical effect (3–5). In addition, the Royal College of Physicians’ (RCP) guidelines for management of adult spasticity using BoNT-A (6) recommend that patient selection and management should be based on individualized criteria, resulting in a patient-centred approach to management.
Despite the ever-expanding literature base on this topic, it is clear that further clinical research is necessary to increase understanding and fill gaps in post-stoke spasticity treatment protocols. The group felt that, in the intervening time, there remained a need to provide practical advice on how best to tailor treatment regimens using BoNT-A for individual patients in order to optimize care.
Although BoNT-A is an established treatment for focal spasticity, there is little consensus on how to improve efficacy, and there is a need to increase prescribers’ confidence in its use, share current best practice, and identify reasons for sub-optimal responses (e.g. injection technique, dosing, muscle selection).
The group agreed 3 key areas in which additional practical guidance and/or personal training and supervision is required: (i) individualized approach to spastic upper limb in stroke; (ii) optimal injection technique and preparation of the toxin; and (iii) adjunctive treatments. They examined the evidence for each topic, obtained from literature searches using the College of College of Physicians and Surgeons of British Columbia review, Medline, CINAHL and PubMed databases. They subsequently met on 2 separate occasions for full-day discussions to agree consensus statements on the topics. The gaps in the literature were filled with the knowledge acquired from the combined clinical experience of the group (Table I). Some topics, such as the assessment of spasticity and measurement of the effects of the treatment, have not been addressed by this review, as the authors felt that they have been adequately evaluated elsewhere. However, the authors agree that the Ashworth/Modified Ashworth scale, in spite of its limitations, is currently the preferred scale for assessment of spasticity, due to its simplicity of use. Whilst there is increasing interest in the Tardieu scale, due to its consideration of the velocity-dependent nature of the condition, it is more complex to implement and, therefore, more difficult to interpret. The measurement of treatment effects has not been included in this review, as it has been addressed in many guidelines (6).
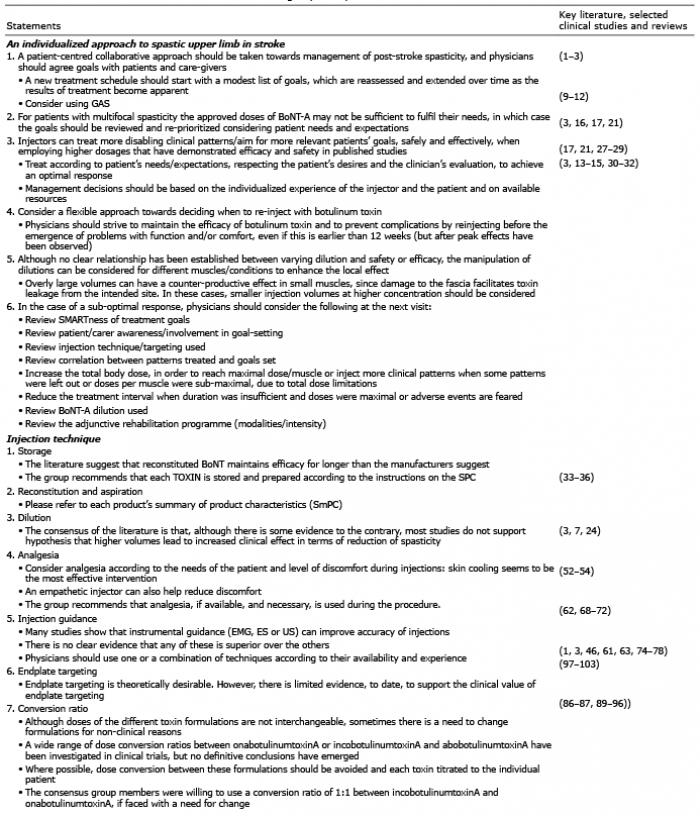
Table I. Consensus statements from the international group of experts
Table I. Cont.
The need for an individualized approach is well established (2, 7, 8). While randomized controlled trials (RCTs) have become the accepted gold standard for directing treatment, their strict protocols may not allow an individualized approach or treatment interventions that are applicable to real-life clinical scenarios.
Goal-setting
Patients and caregivers have wide-ranging goals and expectations from treatment, and optimal management plans should accommodate these variables whenever possible.
Goal-setting, as measured by the Goal Attainment Scaling (GAS), in which individual goals for intervention are tailored to individual patients (9, 10), has merit. It sets targets for intervention and provides a standardized measure of outcome (11). GAS has been shown to be sensitive to changes in areas of symptoms/impairment and function/participation, following focal interventions, which are not detected by more global measures (12). Approximately half of the group involved in this analysis stated that they use GAS always or often.
However, consideration must also be paid to how goals are defined and prioritized. For example, a goal may be “reduction in pain”, but we must define whether this is a reduction in intensity or duration of pain. In addition, while a patient may consider being able to sign his or her name or shake hands as desirable functional goals, the physician might regard the manual dexterity improvement as insufficient if they cannot unscrew a bottle cap.
It is undecided if a new treatment schedule should start with a modest list of goals that are gradually extended, or if the patient and physician should strive from the outset to accomplish an ambitious list of desired outcomes.
Throughout the continuum of care, goals need to be re-evaluated and re-prioritized as it becomes clear what can be achieved, considering the outcome and the limitations of treatment.
Optimal dose of botulinum toxin A
The optimal dose of BoNT-A per injection session is not clear. Although Summaries of Product Characteristics (SPC) give recommendations regarding dosage, it is not known if these are optimal. Clinical experience and recent guideline updates (3) have identified opportunities to tailor treatment to increase the benefits for patients. Several patient/practitioner surveys conducted during the last few years have highlighted a requirement for more tailored treatment options and more flexibility in dose (and/or injection intervals) than those currently approved (13–15).
Increasing the toxin dose can reduce the Modified Ashworth Scale (MAS) score (3, 16–18). Most physicians who administer BoNT to patients with post-stroke spasticity believe that greater flexibility regarding dosing and treatment intervals for injections might benefit some patients (8,19). Approximately 60% of physicians would use higher doses if there were no label restrictions (20).
The use of higher than approved doses of BoNT-A has been investigated in the TOWER study (21). This prospective, open-label, single-arm, multicentre, dose-titration study investigated the safety and efficacy of increased incobotulinumtoxinA total-body doses (up to 800 U); this is a higher limit than studied previously. Doses of up to 800 U allowed the treatment of an increasing number of spasticity patterns at a single treatment session without compromising safety or tolerability, enabling patients to achieve more goals. A dose of 800 U of incobotulinumtoxinA enabled more than 97% of patients with cerebral-origin spasticity to receive simultaneous treatment of the upper and lower limb, and more patients achieved 3 or 4 goals (87%) with 800 U than with the lower dose (25% in the 400 U group). The higher dose also increased the number of patients with no quality of life (QoL) impairment on the EuroQol-5D (EQ-5D) scale. Importantly, in the TOWER study there was no development of clinical non-responsiveness and no development of neutralizing antibodies. The majority (82%) of the clinicians in the consensus group stated that they were comfortable using 800 U of incobotulinumtoxinA in routine clinical practice.
A recent study (18) assessed the effects of repeated injections of abobotulinumtoxinA in doses of 500, 1,000, or 1,500 over a period of one year. Although the incidence of treatment-emergent adverse events (TEAEs) decreased across cycles, the investigators’ evaluation identified 2 cases (constipation, diplopia) in which possible remote spread of toxin effect could not be ruled out and 8 patients seroconverted for neutralizing antibodies up to the study end.
Whilst it could be hypothesized that higher-than-approved doses of onabotulinumtoxinA would also be safe and effective, the group felt that it was important to first demonstrate this in clinical trials.
Initiation and frequency of botulinum toxin A administration
There are also considerations about the optimal time to start treatment and treatment intervals. In lower limb studies in patients with stroke and traumatic brain injury, there is some evidence that earlier treatment of patients with BoNT-A in the post-stroke period achieves better outcomes than is seen in those treated later (17, 22–24). Wein et al. have compared treatment at < 24 months with > 24 months post-stroke and show greater improvement in MAS in the < 24-month post-stroke group, but comment that this is perhaps due to the use of higher doses and more muscles being injected during the open-label phase (Wein et al., personal communication). In an exploratory study, early abobotulinumtoxinA treatment significantly delayed time to reach re-injection criteria compared with placebo in patients with post-stroke upper limb spasticity (ULS) (25).
Duration of effect of BoNT-A can influence the choice of treatment intervals. The duration of effect of BoNT-A can vary between patients, depending on numerous parameters (e.g. clinical condition, age of patient) (13). Although the duration of action is correlated to the amount injected at lower doses, at higher doses of BoNT-A, the duration of action is thought to saturate at approximately 3 months (26).
Flexibility in treatment protocols is determined by individual product licenses, which often lag behind real-world experience (17, 21, 27–29). It may be better to select treatment intervals based on individual patient needs rather than pre-defined regimens.
In a survey of post-stroke spasticity patients (13), while 55% of patients were re-injected at 13–14 weeks or later, 79% actually preferred shorter injection intervals (35.5% at 11–12 weeks). Patient satisfaction decreased as the effects of the previous injection wore off. Thus, patients live with a roller-coaster effect, having treatment that declines in effectiveness with time and then increases again after another injection, suggesting that attempts should be made towards maintaining a near steady-state level of patient satisfaction. To date, unlike in cervical dystonia (CD) (30–32), there are no prospective safety and tolerability data available to support flexible injection intervals in spasticity. However, more than half (53%) of the consensus group members stated that they were confident to re-inject patients when they reported that the maximum effects have worn off, irrespective of common practice (12-week intervals).
A number of different methods and techniques are commonly employed to perform BoNT-A injections and there is much variability in practice for preparing and handling the toxin and in techniques used for localization, analgesia, dilution and muscle targeting. The practical recommendations made by the group are summarized below. The authors recommend that personal hands-on training and supervision is mandatory for inexperienced clinicians.
Storage
Before reconstitution, the manufacturers’ recommendations regarding storage should be followed (as detailed in the package inserts) (33–36).
The group recommends that each toxin is stored and prepared according to the SPC instructions.
Reconstitution and aspiration
Manufacturers’ package inserts recommend that BoNT-A should be reconstituted with preservative-free normal saline. Usual practice is to shake gently and avoid aggressive agitation, since one study suggested that mechanical effects of reconstitution were potentially damaging to toxin structure and efficacy (37). However, further studies have shown that constant agitation of the reconstituted solution did not decrease efficacy up to 42 days (38) and vigorous vs gentle agitation made no impact on efficacy (39).
A more recent study concluded that shaking and use of small-bore needles can damage the toxin, as measured by the response time of mouse hemidiaphragm to reduction in force of muscle contraction (40). Since aspiration leaves a small volume of toxin in the vial, use of small-bore needles can be helpful in increasing aspiration efficiency (balanced with the theoretical risk of toxin damage). Some suggest removing the vial stopper to access the maximum volume of toxin, but this risks vial breakage and contamination of the solution, especially if multi-use is planned (41). Residual volume in a capped vial is 0.127 ml, equivalent to almost 13 U per 100 U vial (in a 100 U/ 1 ml dilution). Alternatively, by using a 2” long 21G needle, it is possible to limit loss to 2.3–4.6 U/vial (assuming 100 U/ 1 ml dilution) (42). The group was supportive of this approach, awaiting further evidence.
Dilution
A wide range of dilution ratios may be used according to circumstances for common postures of the upper limb in post-stroke spasticity (3, 24).
Animal studies have shown that injections of higher volumes can increase denervation (43, 44). However, the situation is not so clear in humans due to unavailability of adequately powered studies. Higher volumes have been reported more effective in children with cerebral palsy (45). One study has considered both volume and end-plate targeting of the biceps brachii in 21 adults with spastic hemiplegia following stroke (46). Results showed that high-volume/non-targeted and low-volume/targeted were superior to low-volume/non-targeted. Higher volume and lower concentration has also shown a trend for better efficacy in patients with upper limb spasticity of various aetiologies (47). In a study of the upper limb, despite a trend for more improvement using higher volumes, the improvement was not statistically significant (48); a lack of significance was also seen in 3 studies of the lower limb, 2 of which investigated patients with spastic equinovarus foot (49–51).
The group advised that it may also be necessary to take individual muscle structure into account when injecting, and approximately half stated that they changed dilution to achieve an optimal effect. However, further recommendations are needed to identify the number and location of injection sites (7) required to achieve maximum toxin effect.
Analgesia
EMLA (eutectic mixture of local anesthetics, Aspen Pharma, Ireland) cream and ice packs are equally effective in reducing injection pain at the gastrocnemius, but ice is an easier and cheaper option (52). Vapocoolant has been found to be ineffective (55); however, the time lapse between use of vapocoolant and the injection itself could be a factor. Other authors found (on forehead injections or gastrocnemius for electromyography (EMG)) that vapocoolant is more effective than EMLA (53, 54).
An older study evaluated whether muscle temperature affects BoNT-A uptake (at least in vitro) (55) but firm conclusions cannot be drawn.
In considering more generalized anaesthesia, nitrous oxide was shown to be more effective than rectal midazolam in a double-blind, randomized placebo-controlled trial in 50 children with cerebral palsy (CP). Nitrous oxide had the advantage of less post-procedural sedation (56). However, a more recent study in children with CP, analgesia combining nitrous oxide and EMLA cream was less effective than expected for BoNT-A injections (57).
General anaesthesia (GA) can be used in patients with CP and adults, especially in those selected cases who show lack of cooperation, have severe conditions requiring extensive injections, or who have severe cognitive deficit (58).
To reduce injection discomfort, anaesthesia through skin cooling seems the most effective intervention. An empathetic injector may also help to alleviate discomfort (59).
The group recommends that analgesia, if available and required, is used during the procedure.
Injection guidance
Four main injection guidance techniques have been evaluated in clinical trials: needle placement under anatomical guidance (AG), electrical stimulation (ES), electromyography (EMG), and direct visualization by ultrasonography (US). Other techniques have been studied (fluoroscopy, computerized tomography (CT) scan, etc.), but data are sparse.
A number of descriptive studies have considered how to define anatomical landmarks that locate and target motor endplates (60–63).
Palpation, or manual identification of a muscle using anatomical landmarks is not accurate for all muscles; this has been demonstrated in both cadavers and patients (stroke and CP) (64–67).
The advantages of US over other guidance techniques include: direct and continuous visualization of the needle, the target, structures to be avoided and the injectate spread within the target structure. US has identified forearm muscles at distinctly different sites from those identified by anatomical guidance (62, 68, 69). Considering the results of injections, both US and EMG have been demonstrated to lead to better results compared with AG in wrist and finger flexor spasticity (70). US guidance seems to lead to better results on wrist and finger spasticity compared with AG (71). However, a recent study found no differences between US, ES and AG (72).
Supportive literature from lower limb studies show that the accuracy of injections in the gastroc-soleus muscle is higher with ES guidance than with AG. However, US guidance seems to lead to better results on triceps surae spasticity compared with AG and EMG (65)
Most studies show that instrumental guidance (EMG, ES or US) can improve accuracy of injections (73). Although there is no clear evidence that any of these is superior, the group strongly recommends the use of EMG and/or ES and/or US injection guidance to optimize muscle localization. Injection using only anatomical landmarks should be used only when other techniques are unavailable.
End-plate targeting
End-plate targeting considers the end-plate topography, but is also related to injection technique. Nerve and endplate distribution in some human muscles is quite well described (63, 74–77). It has been observed that the area of highest endplate density is an inverted V-shaped band 1 cm in width between the lower third and upper two-thirds of the muscle belly in human biceps brachii muscles (3, 61). A high-volume dilution (20 U/ml) and an endplate-targeted injection are superior to a low-volume, endplate non-targeted injection, when injecting the biceps brachii (46).
Although some muscles have well-defined motor endplate topography, others, such as the soleus and gastrocnemius, which have diffuse, or ill-defined endplates, may require a more even spread of injection, using multiple injections and larger injection volumes (1). Im et al. (78) demonstrated that a mid-belly injection in the gastrocnemius is no different in efficacy from injection in more anatomically endplate dense regions.
The consensus group acknowledged that end-plate targeting may be helpful for superficial muscles, such as the biceps or gastrocnemius, but none of the group is actively using this technique due to increased time to perform this procedure and the resultant increased pain for the patient.
Conversion ratio
Manufacturers’ product labels state that different formulations of toxin are not interchangeable or bioequivalent and conversion ratios have not been systematically studied between formulations. However, since real-world practice sometimes requires switching formulations, attempts have been made to investigate conversion ratios in both clinical studies and in practice. Conducted in variable patient populations, study results are wide-ranging and careful interpretation is recommended.
Conversion ratios of 1:1 to 1:11, between onabotulinum toxin-A and abobotulinum toxin-A, have been used in clinical studies (79–88). Although many authors considered 1:3 or 1:4 to be appropriate (89–95), some evidence suggests that conversion ratios differ between muscles (96).
Studies have shown a conversion ratio of 1:1 for incobotulinum toxin-A to onabotulinum toxin-A in CD and blepharospasm (97–103). This is reflected in the European SPC for incobotulinumtoxinA (35). In focal dystonia, a study showed that switching from abobotulinum toxin-A to incobotulinum toxin-A with a dose ratio of 4:1 was effective and well-tolerated (104).
Although no conversion ratio can be recommended at this time, if faced with a need to change formulations for practical reasons, the consensus group was comfortable using a conversion ratio of 1:1 between incobotulinumtoxinA and onabotulinumtoxinA; there was no agreement on a conversion ratio between onabotulinumtoxinA and abobotulinumtoxinA
BoNT-A injections are a part of spasticity management. The group agreed that BoNT-A injections should always be followed with a physiotherapy programme. Table II represents the techniques that are currently used by group members. However, we need to establish the optimal adjunctive therapy to be used alongside BoNT-A.
Table II. Adjunctive therapies: current use by group (n = 19)
Demetrios et al., in a Cochrane review, found only 3 RCTs (105–107) that assessed rehabilitation after BoNT-A (108).
Two recent reviews looked at adjunctive therapies post-BoNT-A in post-stroke spasticity (109, 110). Mills et al. performed a systematic literature review and concluded that there is high-level evidence suggesting that adjunct therapies may improve outcomes following BoNT-A injection. However, no results have been confirmed by independent replication; all interventions would benefit from further study.
Kinnear et al. also emphasized that the effectiveness of these therapies is uncertain, with the 95% CI sometimes spanning zero (110).
Casting, taping and splinting
Available literature on casting, taping and splinting for spasticity management post-stroke were reviewed, but due to the limited number of papers this review concentrates on casting (as there were more studies). A recent review (111) of the current evidence for casting as an adjunct therapy following botulinum toxin injection for adult limb spasticity concluded that adjunct casting of the lower limbs may improve outcomes following BoNT injections. The group also considered studies on casting/splinting and taping together, focusing on RCTs that had the highest impact and the highest PEDro scores (scale developed by the Physiotherapy Evidence Database to determine the quality of clinical trials: high quality=6–10; fair quality=4–5; poor quality=≤ 3) (112). The relevant studies are summarized in Table III. Four RCTs studied BoNT-A plus casting/taping/splinting in lower limb with positive results (113–116). Two studies (117, 118) investigated BoNT-A plus/minus taping in lower limb which a favourable trend towards the use of taping, but no long-term benefits. A retrospective study (119) concluded that serial casting may be an appropriate intervention following BoNT-A injection to prevent equinovarus deformity and improve quality of walking in chronic stroke patients. Another RCT (120) reviewed the use of BoNT-A plus casting/taping/splinting in the upper limb and found that adhesive taping was more effective than daily manual stretching combined with passive articular mobilization and palmar splint.
A common criticism of many papers is that they provide insufficient detail about injection technique (manual palpation, EMG, nerve stimulator or US guidance), the type of casting/splinting/taping or orthotics used. More robust studies are needed comparing BoNT-A and adjunctive therapy with casting/taping/splinting post BoNT-A with BoNT-A treatment alone. Future studies should also indicate the specific timeline and technique of casting/taping/splinting following injection of BoNT-A. Nevertheless, based on clinical experience, the group recommends the use of casting and/or taping and/or splinting, if available, especially if there is a high risk of soft-tissue shortening.
Table III. Summary of casting/taping/splinting studies plus botulinum toxin A (BoNT-A) in spasticity
Constraint-induced movement therapy
One study examined constraint-induced movement therapy (CIMT) in post-stroke patients in combination with BoNT (106). The PEDro score of this study was 6. Thirty-two patients were assigned to 2 groups and treated with BoNT plus CIMT or BoNT plus conventional rehabilitation (2 h per day, 3 days per week). In both groups, spasticity was better at 4 weeks and 3 months. There was a significant difference in the CIMT group at 6 months in terms of spasticity measured by MAS; utilization of the affected arm with a Motor Activity Log; and arm mobility assessed by the Action Research Arm Test. A weakness of this study was that there was no CIMT alone cohort.
The authors suggest that improvements could be attributable to several factors: improvement in strength and co-ordination in the affected upper extremity as a result of spasticity reduction and repetitive training, a change in learned non-use behaviours, or use-dependent cortical changes after the combination of BoNT-A and CIMT. Currently it is not known whether user-dependent cortical reorganization can occur in chronic patients with significant spasticity. Further research exploring CNS changes accompanying the observed motor gains is warranted (106).
The group recommends that physical and occupational therapy, particularly CIMT, is provided after toxin injection.
Extracorporeal shock wave treatment
The conclusion from the literature is that extracorporeal shock wave therapy (ESWT) reduces spasticity (alone and in combination with BoNT-A injections). A small meta-analysis of 5 studies showed that spasticity (as measured by MAS) improved immediately and at 4 weeks after ESWT compared with baseline (121). The usual target is middle belly or musculotendinous junction (1,500–3,200 I, 0.030 to 0.1 mJ/mm2 reported).
A recent randomized trial (122) investigating whether ESWT is non-inferior to BoNT-A for the treatment of post-stroke upper limb spasticity found that ESWT and BoNT-A caused similar reduction in spasticity of the wrist and elbow flexors (MAS); however, ESWT yielded greater improvement in wrist and elbow passive range of motion (PROM), and upper extremity Fugl-Meyer Assessment (UE-FMA) score. One RCT vs placebo showed that BoNT-A plus ESWT is more effective than BoNT-A plus electrical stimulation (ES) in the forearm (123). The mean outcome measure (MAS, SFS and VAS) in patients decreased in the BoNT-A plus ES group.
Used alone, ESWT can reduce spasticity at forearm and triceps surae following stroke (124–126). Three sessions provided a longer effect (16 vs 8–12 weeks) and greater hand function-wrist control improvement than one session (125). The mechanism behind ESWT is unknown, but it appears to be unrelated to a decrease in spinal excitability (127). The effects last up to 12–16 weeks (although no study with longer follow-up has been conducted). It appears to be well tolerated, with few or no adverse effects.
One publication in CP (128) compared BoNT-A injection plus 3 ESWT sessions with BoNT-A alone. At one-month, significant differences were found between groups in the injected muscles percentage of hardness (p = 0.021) and the MAS (p = 0.001), supporting the hypothesis that the combined effects of BoNT-A and ESWT derive from their respective action on neurological and non-neural rheological components in spastic muscles.
The group concluded that further standardization of treatment protocols including optimal sites, treatment intervals and intensities need to be established. In addition, long-term follow-up studies are needed to understand the mechanism of action and resultant muscle changes with repeated sessions.
Functional electrical stimulation
There are several advantages to combining functional electrical stimulation (FES) or electrical stimulation (ES) and BoNT treatment (129). Postulated mechanisms include: FES increases synaptic activity and increases BoNT-A uptake (short-term), FES increases mechanical spread of toxin (short-term); there is a direct effect of FES on spasticity (short- and long-term); or FES increases strength in antagonists, while BoNT-A decrease tone in agonists (long-term).
Two reviews (129, 130) have concluded that, overall, the studies have small sample sizes and varying quality, with PEDro scores ranging from 6 to 10. Thus, they lack the power needed to draw firm conclusions on the effect of FES as an adjunctive treatment with BoNT-A.
A recently published systematic review (109) provides a starting point for FES review of 8 clinical trials that have examined electrical stimulation in stroke in upper and/or lower limb spasticity. The authors concluded that “When compared with BoNT-A injection alone, we found evidence suggesting that the adjunct use of …electrical stimulation…(Level I)…resulted in improvement in Modified Ashworth Scores by at least one grade”.
It is not always possible to translate findings in one muscle to another at a different anatomical location, but, since we are considering effects on basic nerve functioning, it is likely that findings observed in one body region will be applicable to other areas. So, given the paucity of upper limb studies, reference should also be made to lower limb investigations.
It is not clear whether ES increases BoNT-A uptake or whether it modulates neural activity in the spinal cord or the brain. BoNT-A is taken up by neurones by binding to synaptic vesicle protein SV2. The intention of most of these studies would appear to be increasing toxin uptake by the SV2 receptors.
There is a need to define better the timing and duration of ES after BoNT-A injections. In their systematic review of electrical stimulation, Mills et al. (109) point out that the variables for the intervention (frequency, current pulse duration, intensity) as well as duration of treatment differed between the studies; as such, a meta-analysis could not be performed. Dosing ranged between 30 and 60 min per session, delivered between once daily to 6 times daily for 3 days up to 12 weeks.
Clinical outcomes have been mostly modified Ashworth scores, while physiological studies have considered drop in amplitude of compound muscle action potential.
The group recommends that ES of the injected muscles can be used, if available.
Other concomitant therapies
Two narrative reviews of repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) as spasticity treatment have recently been published (130,131). However, the group concluded that it is too early to include these techniques as adjunctive therapy in stroke.
Most relevant studies of robotics have been conducted in the lower limb. A recent study (132) was conducted in 17 post-stroke patients who participated in daily rehabilitation sessions using the NEUROExos Elbow Module exoskeleton (BioRobotics Institute of Scuola Superiore, Sant’Anna, Italy). Results showed that the robotic exoskeleton can be safely used for post-stroke spasticity rehabilitation and that intensive early rehabilitation treatment may prevent the spasticity occurrence at a later stage.
The group concluded that it is too early to make recommendations on the use of robotics in rehabilitation, due to the paucity of evidence. However, as repetition is important in rehabilitation, robotics are likely to gain more importance in the future.
Self-rehabilitation
A Cochrane review (133) of tele-rehabilitation in stroke stated that there is insufficient evidence to reach conclusions about its effectiveness after stroke. A systematic and meta-analysis of randomized trials (134) showed similar results for Barthel Index, Berg Balance, and Fugl-Meyer scoring in home-based rehabilitation vs conventional rehabilitation, but the studies lacked spasticity outcome measures.
Another study considering home-based tele-supervising rehabilitation (30 min per day for 5 days per week) on physical function in stroke survivors (135), but again not using spasticity outcome measures, concluded that home-based tele-supervising rehabilitation is most likely as effective as the conventional outpatient rehabilitation for improving functional recovery in stroke survivors.
An RCT (136) in 35 outpatients used a 10-m timed walk, the “Timed Up and Go” test, distance covered in 6 min over an ecological circuit, and the stair test. The results strongly suggested that a standardized self-rehabilitation programme constitutes a useful adjunct to BoNT-A injections in order to improve gait-related activities.
However, a survey (137) found that physical therapy professionals are less accepting (than physiotherapy students, professionals and physicians) of the need to engage patients with post-stroke hemiparesis into Guided Self-Rehabilitation Contracts (137) (designed to increase their exercise intensity and responsibility level). There is a need to investigate this topic further using spasticity outcome measures in the context of BoNT-A use.
Since positive benefits are seen with repetition and task-oriented exercise, home-based and tele- rehabilitation, it is recommended that patients are trained to follow a self-rehabilitation programme for spasticity (lower limb) and post-stroke recovery (in general) to supplement their clinician-administered physiotherapy.
The use of BoNT-A and innovative techniques has facilitated a more individualized approach to treatment of post-stroke spasticity, which provides physicians with the opportunity to optimize outcomes and address multiple goals. Table I outlines the consensus view of best practice on the optimal use of BoNT-A within a multidisciplinary context, including use of adjunctive therapies that are commonly employed with BoNT A. BoNT-A usage and choice of adjunctive procedures should be made according to individual needs and treatment goals.
The ToxNet Group is supported by an unrestricted educational grant from Merz. Medical writing support was provided by Brenda McCleary and Jan Hawthorn, who were paid from this grant.
All authors developed the concept for the paper, critically appraised the literature and contributed to the discussion to reach a consensus. The content of the manuscript was directed and reviewed by the authors, who approved the final version before submission.


 Click to show fullsize
Click to show fullsize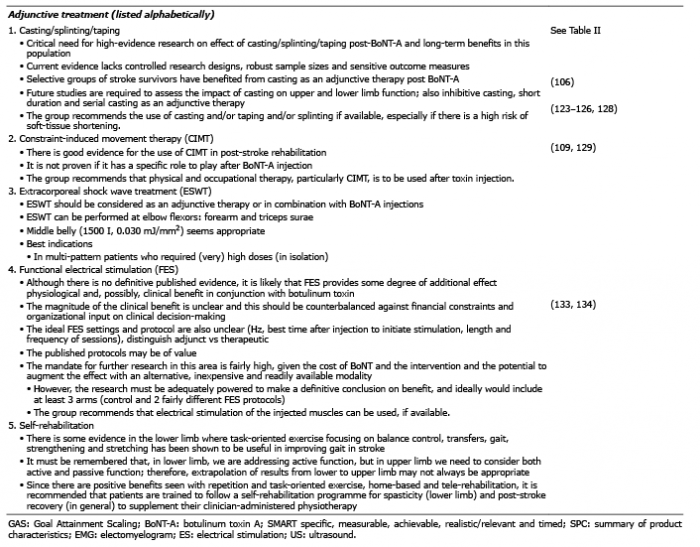 Click to show fullsize
Click to show fullsize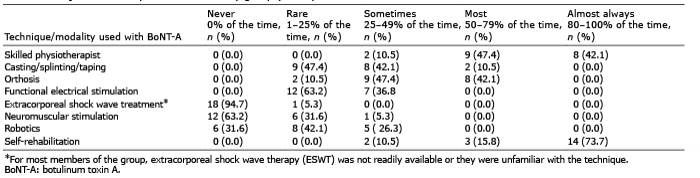 Click to show fullsize
Click to show fullsize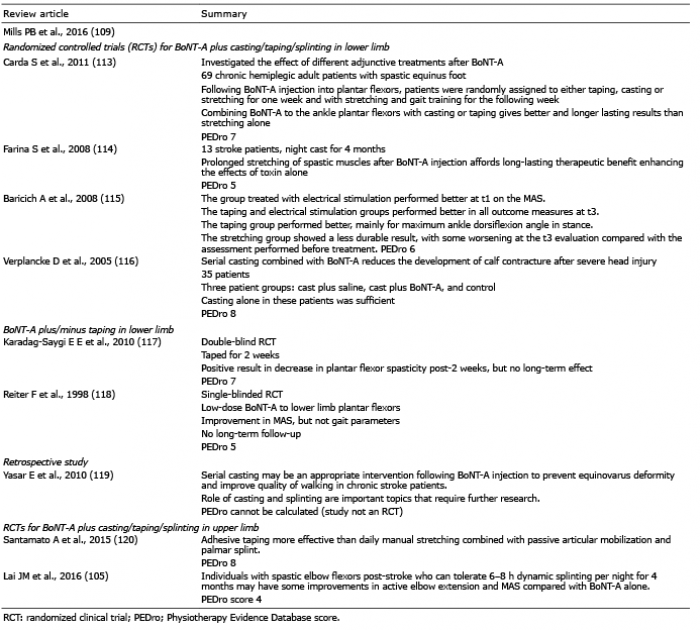 Click to show fullsize
Click to show fullsize