
From the 1Department of Physical Education and Physiotherapy, Opole University of Technology, Opole, Poland, 2Azienda ULSS 3 Serenissima, Physical Medicine and Rehabilitation unit, Venice, Italy, 3Laboratory of Neurorehabilitation Technologies, San Camillo IRCCS s.r.l., Venice, Italy, 4Institute of Physical Education, Tourism and Physiotherapy, Faculty of Pedagogy, Jan Długosz University, Czestochowa, Poland, 5Department and Division of Medical Rehabilitation, Wroclaw Medical University, Wroclaw, Poland, 6Department of Physiotherapy, University School of Physical Education, Wroclaw, Poland
Objectives: To analyse the effectiveness of virtual reality-based interventions within several fields of rehabilitation, and to investigate whether the outcomes of virtual reality-based interventions, in terms of upper or lower limb function, gait and balance, differ with respect to the virtual reality system used.
Methods: A search of PubMed database resulted in an initial total of 481 records. Of these, 27 articles were included in the study. A final total of 20 articles, with neurological, orthoapedic, geriatric or paediatric patients, published between 2012 and 2019, were included in the study. Two independent reviewers selected potentially relevant articles based on the inclusion criteria for full-text reading. They extracted data, and evaluated the methodological quality of each study.
Results: Seventeen studies were included in the meta-analysis. Eight studies analysed upper limb function, with no significant evidence that specialized VR is superior to conventional treatment. Regarding Fugl-Meyer scale results, the effect of specialized virtual reality therapy was found to be significantly better than conventional treatment. No significant differences between specialized VR and conventional treatment were observed in effects on hand dexterity and gait. There was a significant difference in effects on balance in favour of specialized virtual reality as compared to conventional treatment. Gaming virtual reality was significantly better than conventional treatment for upper limb function, but not for hand dexterity, gait and balance.
Conclusion: Use of specialized virtual reality and gaming virtual reality can be advantageous for treatment of the upper extremity, but not for hand dexterity and gait in all pathologies considered. Specialized virtual reality can improve balance in neurological patients.
Key words: virtual reality; rehabilitation; upper limb; hand dexterity; lower limb; gait, balance.
Accepted Oct 6; 2020; Epub ahead of print Oct 19, 2020
J Rehabil Med 2020; 52: jrm00121
Correspondence address: Pawel Kiper, Azienda ULSS 3 Serenissima, Physical Medicine and Rehabilitation unit, Venice, Italy. E-mail: pawel.kiper@ospedalesancamillo.net; pawelkiper@hotmail.com
Doi: 10.2340/16501977-2755
Virtual reality is an innovative technology consisting of interaction between a user and a computer that involves real-time simulation. The objectives of this review were to analyse the effectiveness of virtual reality interventions within several fields of rehabilitation, and to investigate whether the outcomes differ with respect to the type of virtual reality system used. From an initial search of the literature, 481 records were retrieved. Of these, 20 articles were selected for qualitative analysis. Two independent reviewers selected relevant studies based on the inclusion criteria. Furthermore, 17 studies were included for meta-analysis (i.e. quantitative analysis). The results showed that upper limb function can improve with the use of both specialized and gaming virtual reality. Balance disorders improved with specialized virtual reality, but not with gaming virtual reality. However, no improvements were evident in hand dexterity or gait for either specialized or gaming virtual reality. In conclusion, interventions using specialized virtual reality and gaming virtual reality can be advantageous for treatment of the upper extremity, but not for hand dexterity and gait in all pathologies considered. Specialized virtual reality can improve balance in neurological patients.
Virtual reality (VR) is an innovative technology consisting of a high-end user–computer interface that involves real-time simulation and interactions through visual and auditory sensorial channels (1, 2). Computer-based 3-dimensional (3D) environments provide sensory information in a form similar to that received from real-world objects and events. VR allows individuals to experience and interact with or within environments with enhanced feedback (3, 4). The definition of VR is based on a concept of “presence”, which refers to the sense of being in a surrounding environment. Four branches are currently defined in relation to VR technology, characterized by their different sense of “presence” within virtual worlds, i.e. non-immersive VR, immersive VR, augmented VR, and mixed VR (3). Thus, what determines the sense of “presence” is the level of immersion provided (i.e. VR interaction level), which in turn depends on the system used.
Since VR technology has been introduced into clinical practice, its importance and usefulness have increased significantly. This meaningful progress in the use of VR systems for patient recovery, which has important favourable results, has led to interest in studying the impact of VR on motor recovery. VR technology is widely used in recovery from neurological disease (5), and in paediatrics (e.g. cerebral palsy) (6, 7), orthopaedics, (8) and psychiatry (e.g. for phobia treatment) (9). In the last decade, VR has also been used successfully in telemedicine and telerehabilitation, opening up a new mode of health delivery (10). Furthermore, a wide range of VR systems are available, which can be used for treatment both in clinical and home-based environment. These are grouped as so-called “specialized” VR (i.e. specifically developed therapeutic VR systems) and gaming VR (i.e. commercial VR-game consoles that can be used in clinical practice) (5, 11, 12).
Objectives
The objectives of this systematic review were to analyse the effectiveness of VR-based interventions within several fields of rehabilitation, and to investigate whether the outcomes of VR-based interventions differ, in their effects on upper or lower limb function, gait and balance, with respect to the type of VR system used.
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews (13).
Search strategy
Studies related to VR training were considered eligible for review. PubMed database was searched for appropriate articles, using the following criteria: ((virtual reality [Title/Abstract] OR virtual environment [Title/Abstract]) OR virtual therapy [Title/Abstract]) AND rehabilitation [Title/Abstract] AND (“loattrfree full text”[sb] AND (“2012/01/01”[PDAT] : “2019/12/31”[PDAT])). Articles were filtered by date of publication, with the aim of including only those published within the last 7 years, due to the large available literature on the topic of VR. Only randomized controlled trials (RCTs) were included. All treatments provided to participants were reported with as much detail as possible. If needed, the trials’ author was contacted for clarification and to obtain missing data.
Eligibility of studies
Rehabilitative interventions for the upper and lower limbs in the virtual environment, in different clinical fields (e.g. neurology, orthopaedics, paediatrics, etc.) were considered for review. Both specialized VR and VR gaming systems were included.
Data collection
Screening of research records was conducted by 2 independent reviewers, with the intervention of a third researcher in case of disagreement. A data extraction form was created and applied by the reviewers to extract relevant data. All articles included in the review underwent methodological assessment for risk of bias using Review Manager 5.3 (RevMan) (Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) “Risk of bias” (Appendix 1).
Assessment of risk of bias in included studies
Risk of bias for the included studies was assessed independently by 2 reviewers, who were supported by a third researcher in case of disagreement. Assessment was conducted following the criteria set out by the Cochrane Collaboration in the Cochrane Handbook for Systematic Reviews of Interventions (14). The following domains were evaluated: (i) selection bias: sequence generation, allocation concealment; (ii) detection bias: blinding of outcome assessment; (iii) attrition bias: incomplete outcome data; and (iv) reporting bias: selective reporting. It was decided to omit the domain that assesses the blinding of participants, as blinding is not possible in most cases and because it was deemed that this domain related to the nature of the intervention, instead of to study quality, as Laver et al. already stated (15). Risk of bias for each domain was coded as “high risk”, in case of a high possibility in the occurrence of bias; “low risk”, in case of a low possibility of bias; and “unclear risk”, when the real incidence of bias could not be defined exactly.
Statistical analysis
A review was conducted using Review Manager 5.3 (RevMan) for statistical analysis. The methodological quality of studies was recorded in the risk of bias tables. Outcome measures were assigned to each domain assessed (upper limb function, hand dexterity, balance and gait) for both specialized and gaming systems. Treatment effect was evaluated using mean difference (MD) in case of homogeneous outcome measures, or standardized mean difference (SMD) when the outcomes were assessed with different scales, and 95% confidence intervals (95% CI) were calculated. A meta-analysis was carried out based on a random-effects model or fixed effect model with 95% CIs.
Heterogeneity was assessed considering intervention and outcome measures, pooling data for the most clinically homogeneous trials. Statistical heterogeneity was assessed with the I² statistic, establishing the cut-off value as 50%.
Analysis of subgroups was planned in relation to the different types of rehabilitation (e.g. neurorehabilitation, paediatric rehabilitation) and according to the different aetiologies of motor impairments (i.e. stroke and tetraplegia)
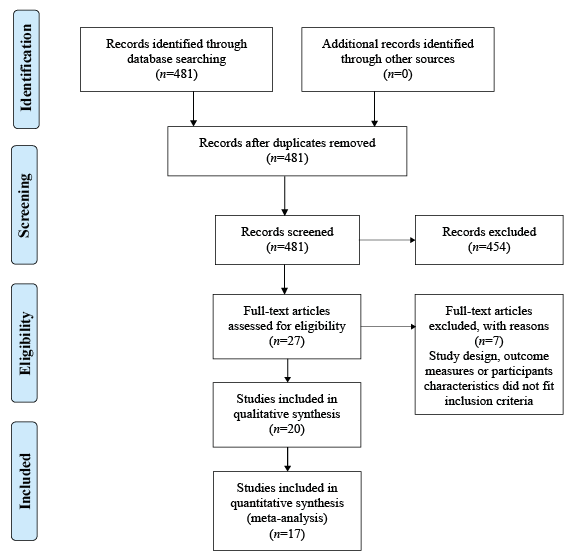
Electronic searching of the PubMed database identified 481 records (Fig. 1). After screening the abstracts, 27 papers were selected for full-text reading. Of these, a final total of 20 papers were included in the review. Of the 20 included studies, 16 (with 518 participants) related to treatment of neurological disorders, 1 (with 30 participants) related to treatment of orthopaedic impairment, 1 (with 70 participants) related to geriatric patients, and 2 (with 128 participants) related to treatment of paediatric patients. Table I shows the characteristics of the included studies. Fig. 2 shows the risk of bias in the included trials.
Fig. 1. Study flow diagram.
Fig. 2. Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
Table I. Characteristics of included studies
Table I. Cont.
Table I. Cont.
Table I. Cont.
Summary of included studies
All studies focused on VR treatment for the upper or lower limb. Within the neurological diseases 14 studies assessed the effects of VR treatment in patients after stroke for both upper and lower limb impairment (12, 16–26). The following studies focused on upper limb recovery (12, 17–19, 21, 23, 25–28). Ballester et al. showed between-group significant improvement in upper limb function in chronic stroke patients in the Fugl-Meyer upper extremity (FMUE) test (p = 0.037), Chedoke Arm and Hand Activity Inventory (p < 0.552), Barthel Index (p < 0.241) and Hamilton Scale (p < 0.05) (12). Kiper et al. studied kinematics of the upper limb and demonstrated a significant difference between training groups for both kinematic parameters (i.e. time p = 0.008; peak p = 0.018; except speed p = 0.140), and clinical scales (i.e. FMUE p = 0.030; FIM p = 0.021). The authors showed that patients after ischaemic or haemorrhagic stroke can benefit similarly from VR training (27), whereas Saposnik et al. did not find statistical differences between VR gaming compared with conventional rehabilitation. Authors suggest that the type of task used in motor rehabilitation post-stroke might have no importance, as long as it is sufficiently intensive and task-specific (25). Another study that assessed the effect of VR on upper limb function was by Shin et al. The authors conclude that combining occupational therapy with specific VR training can be beneficial for hand recovery. However, this was not confirmed by between-group analysis for distal upper limb function, i.e. FMUE (p > 0.05), Jebsen-Taylor hand function test (p > 0.05), Purdue Pegboard Test (p > 0.05), or Stroke Impact Scale (p > 0.05) (19), or for whole upper limb assessment, i.e. FMUE (p < 0.61) and Modified Barthel Index (p < 0.16) (23). Home-based VR intervention for the upper limb was studied by Standen et al. The authors analysed the feasibility of this training, showing statistically important changes in comparison between VR and control group (Wolf Grip test p < 0.01, Motor Activity Log p < 0.05) (18). Thielbar et al. showed statistically significant improvements for both measures of impairment (FMUE: p = 0.048) and measures of task performance (Jebsen-Taylor Hand Function Test: p = 0.021). The authors suggest that using VR may increase the effectiveness and efficiency of therapy following stroke (21). Finally, Zondervan et al. showed significantly greater improvements in an experimental group using VR home-based therapy than in conventional exercise in the Motor Activity Log Quality of Movement (p = 0.007) and Amount of Use (p = 0.04) (17). The effects of VR therapy on lower limb recovery in stroke survivors were presented by Cho et al., In et al., Karasu et al. and McEwen et al. Specifically, studies by Cho et al. showed that, after 4 weeks of intervention in dual-task conditions, greater improvement in walking function was observed in the VR group than in a control group (gait analysis system p < 0.05) (20). The authors concluded that VR therapy is also a feasible treatment for patients with chronic stroke in terms of balance improvement (Berg Balance Scale p < 0.05, Timed Up and Go test p < 0.05) (24). In et al. assessed the influence of VR environment on gait and balance in people after stroke. The results showed statistically significant improvement between training groups in Berg Balance Scale p < 0.05, Timed Up and Go test p < 0.05, Functional Reach Test p < 0.05, and 10-m walking test p < 0.05. These results were confirmed by kinematics obtained from the static balance assessment (16). Karasu et al. aimed to evaluate the efficacy of balance gaming system as an adjunctive therapy to conventional rehabilitation in stroke patients (31). The results showed significant improvement in the Berg Balance Scale (p < 0.001) and Functional Reach Test (p < 0.001). Finally, McEwen et al. showed that VR balance and mobility exercise are positive additions to inpatient stroke rehabilitation (Timed Up and Go test p < 0.05, Two-Minute Walk test p < 0.05, Chedoke McMaster Stroke Assessment Scale Leg domain p < 0.04) (22). Only Lee et al. investigated the effects of game-based VR training in both upper limb and postural balance (26). They concluded that game-based VR canoe paddling training is an effective rehabilitation therapy that enhances postural balance and upper extremity function in patients with subacute stroke when compared with the control group (p < 0.05).
One study evaluated upper and lower limb developmental coordination disorder in children (11). The authors showed that the Movement Assessment Battery for Children test (p < 0.0001), the Bruininks Oseretsky test (p < 0.0001) and Functional Strength Measure (p < 0.0001) changed significantly within groups. However, they concluded that skills acquired within VR-game scenarios did not necessarily transfer into the real world (11). One study evaluated VR treatment in relation to cerebral palsy, showing a statistically significant difference between groups in muscular strength flexion and extension (p < 0.05), in the Pediatric Balance Scale (p < 0.01), 10-m walking test (p < 0.001) and 2-min walking test (p < 0.001). The authors suggest that VR treadmill training is effective for gait and balance improvement (6). One study involved patients affected by multiple sclerosis. Both groups showed a main effect of time on the centre of pressure (CoP) path length with eyes open (p < 0.024), sway rate with eyes open (p < 0.035), Functional Reach Test (p < 0.001), Four Square Step Test (p < 0.031) and the Fear of Falls self-reported questionnaire (p < 0.023) (29). One study assessed effects of VR therapy on upper limb impairment in patients with spinal cord injury (SCI). Both groups demonstrated clinical, but no significant, changes related to arm function. Moreover, all patients from the experimental group showed high levels of satisfaction with the VR system (28). Within orthopaedics only one study was included, which assessed the effects of VR therapy in recovery of subacromial impingement syndrome. The authors demonstrated that intensity of pain can be reduced with VR training (p < 0.05) (8). One study evaluated the effect of VR on lower limb in geriatric patients, showing improvement in balance disorders and fall prevention (p < 0.01) (30).
The total dose of VR therapy varied between studies. Single sessions lasted from 20 min to 3 h, and a minimum of 10 sessions of training were provided. VR treatments were administered 3–5 times a week. Different types of VR systems were used. Thirteen studies used so-called specialized VR systems (12, 16–23, 27–30), and 7 studies used commercially available gaming consoles (i.e. Nintendo Wii, Nintendo Co., Ltd, Kyoto, Japan) (6, 8, 11, 24–26, 31). Interventions were delivered in inpatient, outpatient, or home settings. Outcome measures were focused on motor skills improvement, and a wide range of clinical scales were used to assess motor and ADL changes (Table I). All studies measured outcomes at the beginning and soon after the interventions were completed. Twelve studies presented outcomes for upper limb function (8, 11, 12, 17–19, 21, 23, 25–28), and 10 presented outcomes for lower limb function (6, 11, 16, 20, 22, 24, 26, 29–31).
Risk of bias in included studies
Fig. 2 shows the risk of bias in the included trials.
Random sequence generation (selection bias). Thirteen studies were assessed as having a low risk of bias for this domain, as the authors described a random component in the sequence-generation process. Five studies did not report information about the randomization process, resulting in an unclear risk of bias. The remaining studies were assessed as having a high risk of bias, with inappropriate randomization methods used.
Allocation concealment (selection bias). Thirteen studies were assessed as having a low risk of bias in this domain, as the allocation methods used were appropriate. Six studies did not report information about the allocation method used, and one study presented a high risk of bias, as therapists were not blinded to the patients’ assignment.
Blinding of outcome assessment (detection bias). Seventeen studies were at low risk of bias, as outcome measures were assessed by therapists who differed from those who provided treatment sessions. Two studies did not state whether assessors were blinded, hence the risk of bias was unclear. One study was judged to be at high risk of bias, as evaluations and treatment programmes were both carried out by the same therapist.
Incomplete outcome data (attrition bias). Sixteen studies were at low risk of bias, as most of the participants were included in the final analysis. Four studies reported a high risk of bias due to the large number of drop outs.
Selective reporting (reporting bias). All studies reported all the pre-specified outcomes. Only the study of Zondervan et al. (17) did not publish all outcome measures registered in the study protocol, resulting in a high risk of bias for this domain.
Comparison of conventional treatment vs specialized virtual reality
Upper limb function (all measures). A total of 8 studies, with an overall total of 204 participants, who were divided into subgroup analysis with regard to aetiology, were analysed (i.e. 7 studies with post-stroke patients and one study with patients after SCI. The meta-analysis did not provide significant evidence that specialized VR is superior to conventional treatment. However, it should also be noted that the analysis was influenced by high heterogeneity. The analyses were performed using standardized mean difference (SMD) with random effects model, since 6 studies used the Fugl-Meyer upper extremity scale, one used the Wolf Motor Function test and one used the Motricity Index. No significant differences were found between specialized VR and conventional treatment in stroke patients (SMD 0.80; 95% CI –0.19 to 1.80, I2 = 88%) in SCI patients (SMD –0.13; 95% CI –0.83 to 0.58), or in total comparison (SMD 0.68; 95% CI –0.18 to 1.54, I2 = 87%) (Fig. 3).
Fig. 3. Upper limb function (all measures): conventional treatment vs specialized virtual reality (VR). SD: standard deviation; 95% CI: 95% confidence interval.
Upper limb function (Fugl Meyer). A total of 5 studies, with an overall total of 138 stroke survivors, were analysed in relation to upper limb function measured with the Fugl Meyer test. Mean difference (MD) with a fixed effect model was used for analysis. Significant differences (MD 8.41; 95% CI 7.13 to 9.68, I2 = 46%) were observed between specialized VR and conventional treatment (Fig. 4).
Fig. 4. Upper limb function (Fugl Meyer): conventional treatment vs specialized virtual reality (VR). SD: standard deviation; 95% CI: 95% confidence interval.
Upper limb hand dexterity function (all measures). Five studies, with an overall total of 110 post-stroke patients, were analysed in relation to upper limb hand dexterity. SMD with random effects model was used for analyses, since 1 study used the Chedoke Arm and Hand Activity Inventory, 2 used the Fugl Meyer upper extremity hand section, and 2 used the Nine Hole Peg Test. No significant differences were found between specialized VR and conventional treatment (SMD 0.98; 95% CI –0.51 to 2.47, I2 = 91%) (Fig. 5).
Fig. 5. Upper limb hand dexterity function (all measures): conventional treatment vs specialized virtual reality (VR). SD: standard deviation; 95% CI: 95% confidence interval.
Lower limb function (gait). For gait, 3 studies, with an overall total of 106 post-stroke patients, were analysed. SMD with a fixed effect model was used for analyses, since 2 studies used a Timed Up and Go test, and one used temporal gait speed parameter. No significant differences were found between specialized VR and conventional treatment (SMD –0.36; 95% CI –0.74 to 0.03, I2 = 0%) (Fig. 6).
Fig. 6. Lower limb function (gait): conventional treatment vs specialized virtual reality (VR). SD: standard deviation; 95% CI: 95% confidence interval.
Lower limb function (balance). For balance, 2 studies, with an overall total of 55 patients, were analysed. Mean difference (MD) with a fixed effect model was used for analyses. Significant differences (MD 3.07; 95% CI 1.11–5.03, I2 = 0%) were observed between specialized VR and conventional treatment (Fig. 7).
Fig. 7. Lower limb function (balance): conventional treatment vs specialized virtual reality (VR). SD: standard deviation; 95% CI: 95% confidence interval.
Comparison of conventional treatment vs gaming virtual reality
Upper limb function (all measures). For upper limb function, 2 studies, with an overall total of 171 participants, were analysed. The analysis was performed using SMD with random effects model, one study used Manual Function test and one used Wolf Motor Function. Significant differences (SMD 0.34; 95% CI 0.04–0.64, I2 = 0%) were observed between gaming VR and conventional treatment (Fig. 8).
Fig. 8. Upper limb function (all measures): conventional treatment vs gaming virtual reality (VR). SD: standard deviation; 95% CI: 95% confidence interval.
Upper limb hand dexterity function (all measures). For upper limb dexterity function, 2 studies, with an overall total of 171 participants, were analysed. For hand dexterity function, SMD with a fixed effect model was used for analyses, since one study used Manual Function test hand section and one used Box and Block Test. No significant differences were observed between gaming VR and conventional treatment (SMD –0.12; 95% CI –0.42 to 0.18, I2 = 74%) (Fig. 9).
Fig. 9. Upper limb hand dexterity function (all measures): conventional treatment vs gaming virtual reality (VR). SD: standard deviation; 95% CI: 95% confidence interval.
Lower limb function (gait). For lower limb function, 8 studies, with an overall total of 63 participants, were analysed, with subgroup analysis in relation to aetiology (i.e. one study with post-stroke patients and one study with cerebral palsy (CP) patients). SMD with a fixed effect model was used for analyses, since 2 studies used the Timed Up and Go test and one used a 10-m walk test. No significant differences were noted between gaming VR and conventional treatment in post-stroke patients (SMD –0.03; 95% CI –0.62 to 0.56, I2 = 25%), CP patients (SMD 0.60; 95% CI –0.35 to 1.55) or in total comparison (SMD 0.15; 95% CI –0.36 to 0.65, I2 = 22%) (Fig. 10).
Fig. 10. Lower limb function (gait): conventional treatment vs gaming VR. SD: standard deviation; 95% CI: 95% confidence interval.
Lower limb function (balance). For balance, SMD with random effects model was used for analyses, since 2 studies used the Berg Balance Scale and one used the Pediatric Balance Scale. No significant differences were noted between gaming VR and conventional treatment in post-stroke patients (SMD 0.41; 95% CI –0.75 to 1.57, I2 = 73%), CP patients (SMD 0.29; 95% CI –0.64 to 1.22) or in total comparison (SMD 0.37; 95% CI –0.32 to 1.06, I2 = 46%) (Fig. 11).
Fig. 11. Lower limb function (balance): conventional treatment vs gaming VR. D: standard deviation; 95% CI: 95% confidence interval.
VR therapy has been shown to result in improvements in analysed parameters, but not with statistical significance for all conditions in comparison with conventional treatment. Significant differences were observed between specialized VR and conventional treatment for upper limb function (Fugl Meyer) and lower limb function (balance). Comparative analysis of conventional treatment vs gaming VR, found significant differences only within upper limb function (all measures).
This review shows that most recipients of VR therapy are patients with neurological disorders, mainly stroke. All studies of patients after stroke showed improvement after VR therapy in comparison with conventional therapy in both upper and lower limbs (11, 14–26). The results of the studies included in this review reveal that stroke patients benefit from this innovative treatment, probably through enhanced stimulation provided by an artificially generated environment leading to the activation of motor learning processes. According to the motor learning paradigms, the efficient movement should be repeated, emulating a reference model as exactly as possible, with the aim of achieving the best motor performance (32). Thus, motor learning paradigms can be seen as a basis for movement re-learning and, according to the results of analysed studies, the VR environment has the potential to stimulate both supervised and reinforcement learning, based on augmented visual, acoustic and sensitive feedback.
VR therapy was also used to treat people with developmental coordination disorder and cerebral palsy, showing improvement in learning new movements from VR environments. VR therapy was also shown to be effective for treating people with multiple sclerosis and SCI. These findings demonstrate a wide range of applications for VR in rehabilitation interventions, and its possible advantage in different clinical settings. In addition, studies included in this review did not find any contraindications to the use of this form of therapy. Only one study was published within the orthopaedic field, in which authors evaluated the effect of a VR programme for recovery of subacromial impingement syndrome (SAIS), showing that the VR training was more effective than home exercise programmes in the short-term in subjects with SAIS (8).
Most of the included studies focused on upper limb treatment, whereas training for the lower limb concentrated mostly on balance. This difference may be due to the complexity of treating upper limb function after stroke, relying on changes in muscle synergies of the upper extremity leading to stereotyped voluntary movements. This change is related to both disrupted motor pathways and altered neural reorganization especially following a stroke. Importantly, approximately 60% of stroke survivors do not recover their upper limb function, conversely less than 25% are unable to walk without full physical assistance (33, 34). Another reason can be related to patient safety during gait or balance treatment, which requires specialized VR systems.
It was observed that the specialized VR systems were used both for treatment and assessment of patients. This was especially common in the neurological field, probably due to the fact that neurological patients require specific and individual training programmes, and only a directed in clinical settings system can be beneficial for these kind of patients. On the other hand, gaming systems were used with children, which can be advantageous because some boring or repetitive exercises can be substituted by more interactive activities. This may help both clinicians and parents to motivate children effectively to comply with their daily therapy.
VR is a growing technology that can provide an important addition to traditional rehabilitation modalities. Research shows that most disabled patients experience not only physical disorders, but also mental health problems (e.g. depression or cognitive impairment) (35, 36). Thus, it could be interesting to combine different motor training aspects with psychological and cognitive ones (e.g. mood improvement, strengthened motivation to active engagement in rehabilitation process, visual-spatial orientation and cognitive stimulation). Future studies should consider this translational aspect for VR therapy.
Study limitations
This study has some limitations that need to be addressed. Firstly, only one database was searched for studies, due to the wide number of publications related to the rehabilitation field. Secondly, only full free-text articles were included, providing an overview of accessible clinical outcomes for a wide audience. In addition, no information was obtained from authors related to p-values for the results of included studies.
Conclusion
Implications for clinical practice
Rehabilitation based on VR therapy is emerging as an effective modality for the treatment of balance as well as the upper extremity. VR-based therapy is widely used in the neurological field, especially for rehabilitation after stroke. To date, studies have shown some efficacy of VR-based approach with both specialized and gaming VR systems for gait and hand dexterity; however, this was not significant. Future research into the use of VR in neurological patients should utilize larger samples assessed over time, in order to investigate long-term effects and psychological aspects of the therapeutic intervention. Specialized VR and gaming VR can be advantageous for the upper extremity, but not for balance treatment. There is insufficient evidence across free available articles to reach conclusions about the effects of specialized VR and gaming VR on hand dexterity and gait speed.
Implications for further research
This systematic review highlights the need for further research into VR-based approaches for rehabilitation interventions for gait and hand dexterity. Furthermore, due to the differences in outcome measures, in order to better compare data from different trials specific protocols with equal outcome measures should be developed. Finally, improvements in the methodological quality of evidence are needed, by increasing the number of participants in trials, and correctly randomizing them, in order to minimize the possible effects of confounding factors.
The authors thank Dr Katie Palmer for language revision.
The authors have no conflicts of interest to declare.
Appendix 1. Risk of bias in included studies.
Appendix 1. Cont.
Appendix 1. Cont.


 Click to show fullsize
Click to show fullsize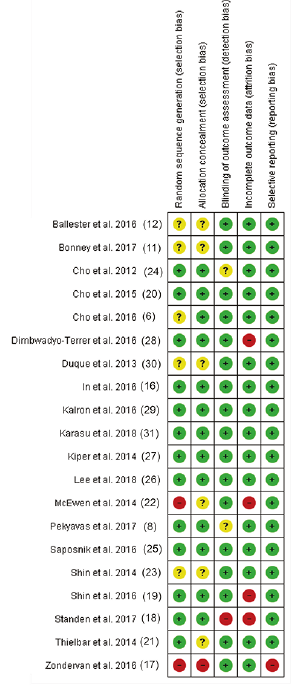 Click to show fullsize
Click to show fullsize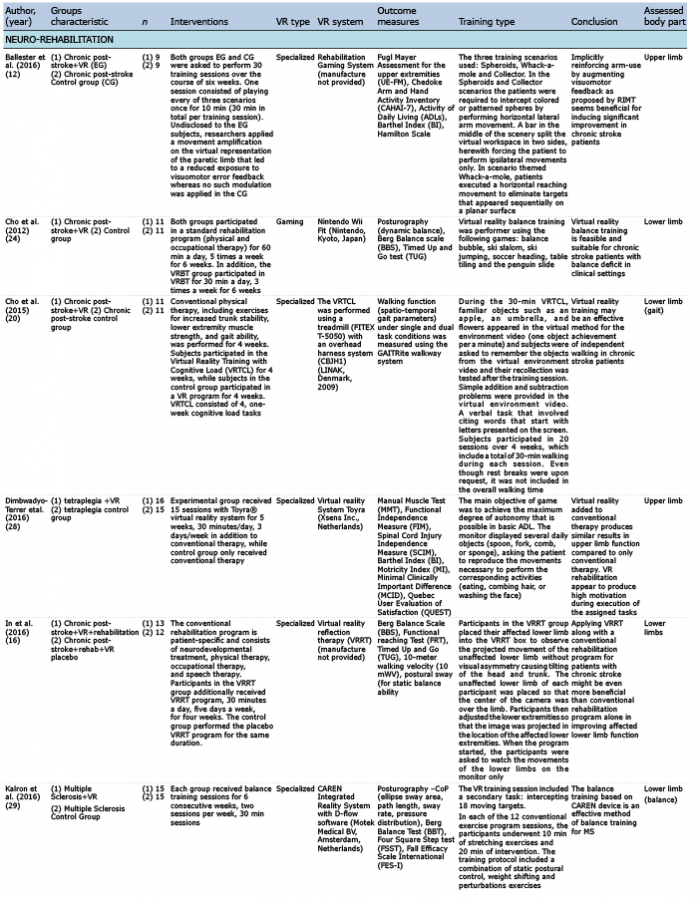 Click to show fullsize
Click to show fullsize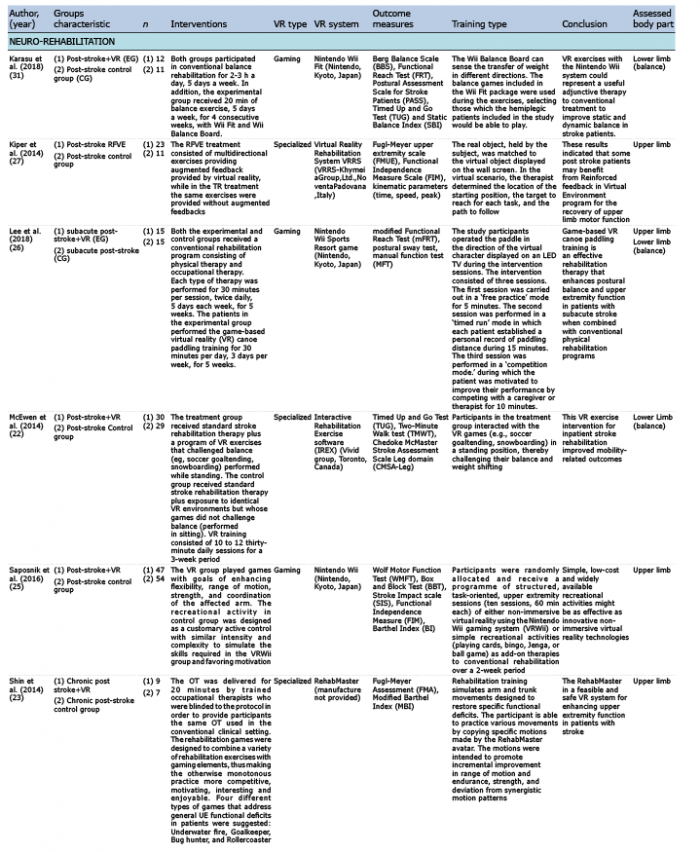 Click to show fullsize
Click to show fullsize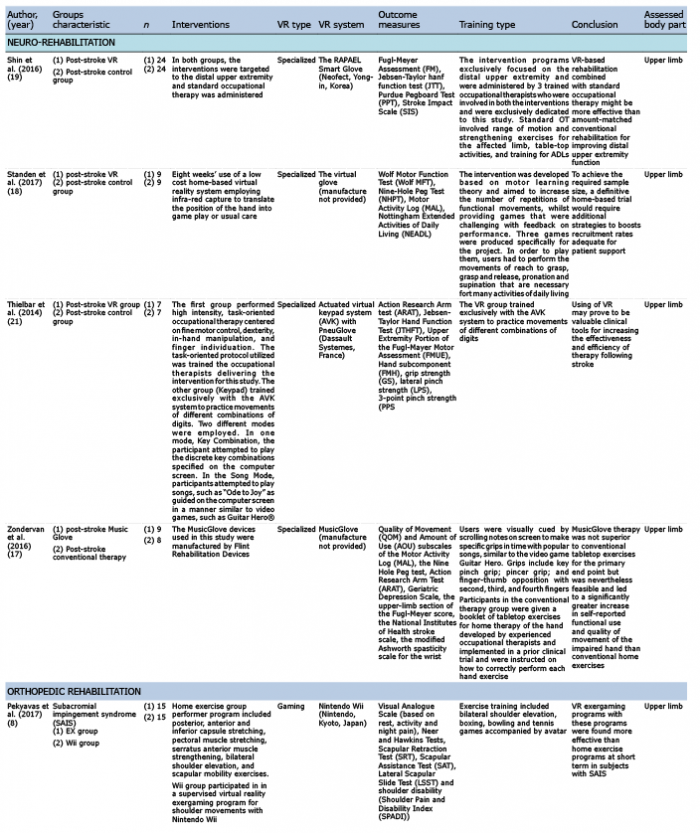 Click to show fullsize
Click to show fullsize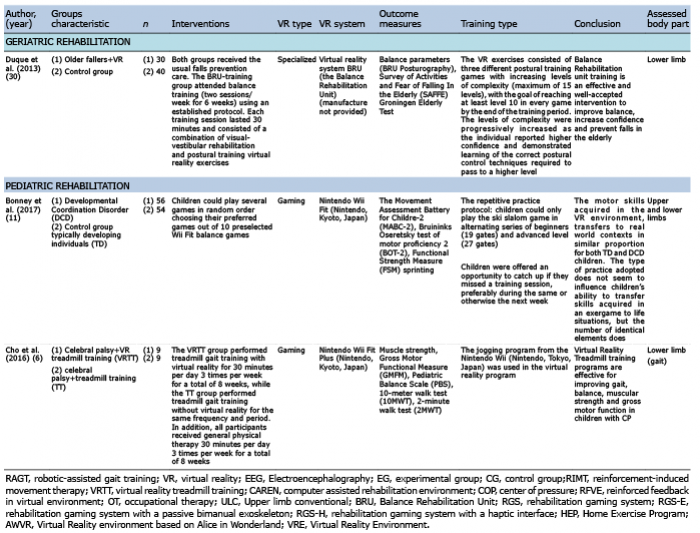 Click to show fullsize
Click to show fullsize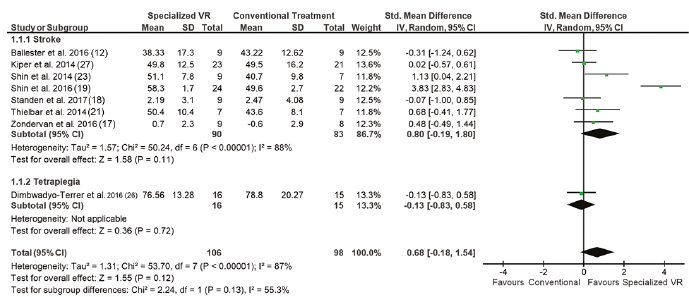 Click to show fullsize
Click to show fullsize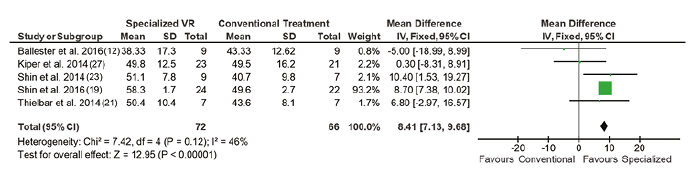 Click to show fullsize
Click to show fullsize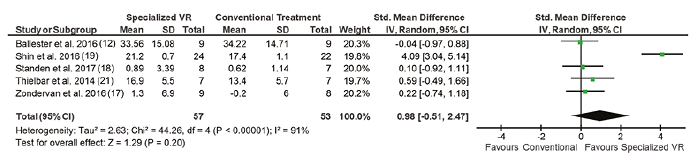 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize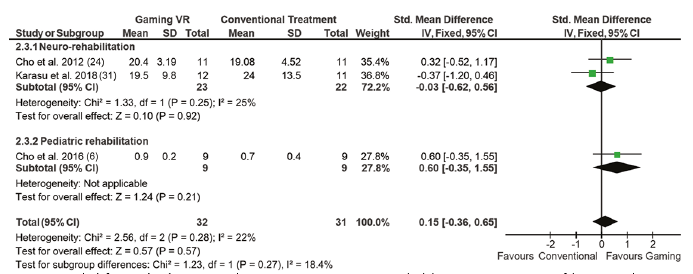 Click to show fullsize
Click to show fullsize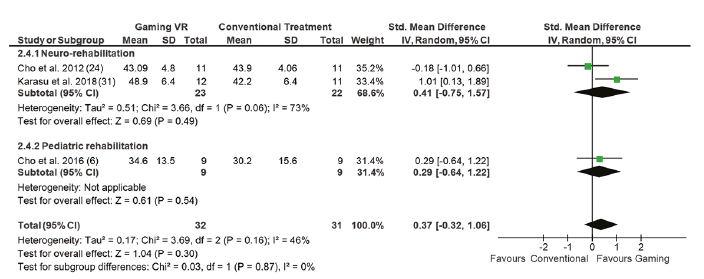 Click to show fullsize
Click to show fullsize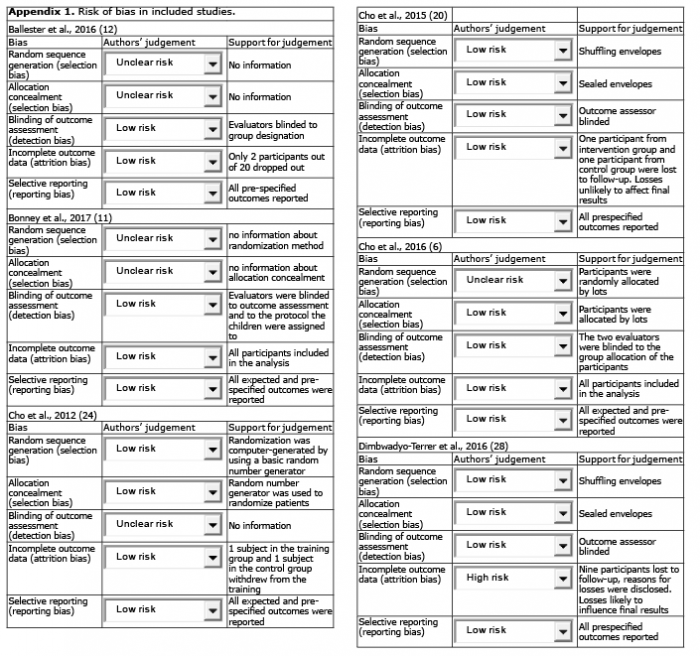 Click to show fullsize
Click to show fullsize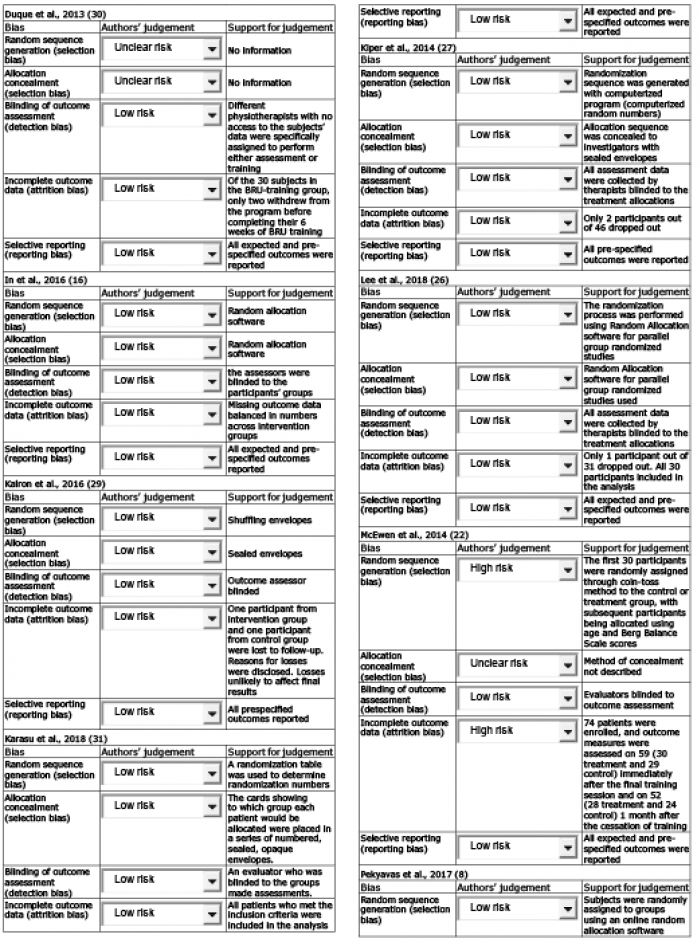 Click to show fullsize
Click to show fullsize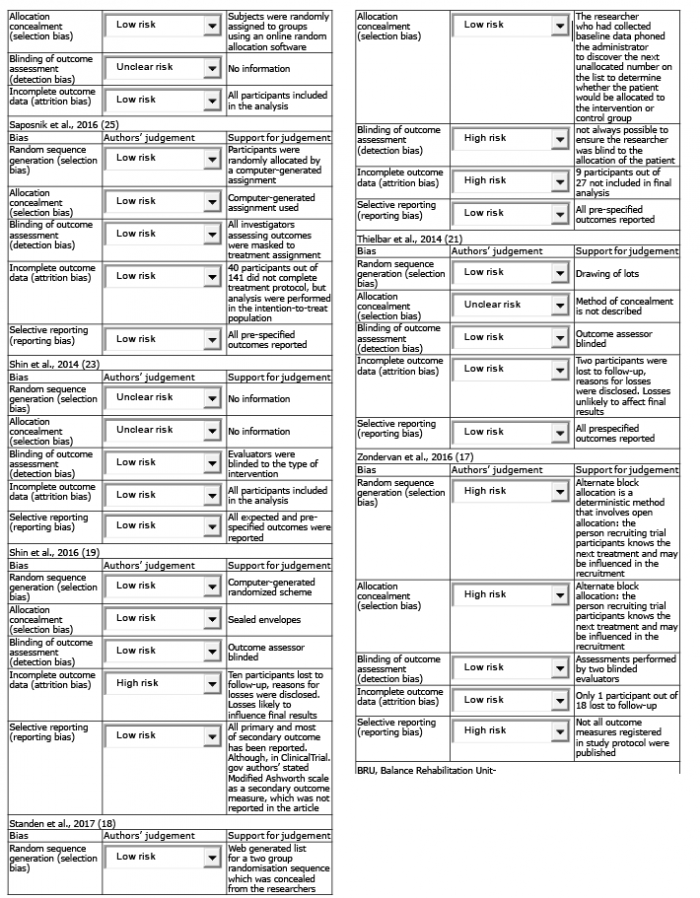 Click to show fullsize
Click to show fullsize