
Objective: To investigate the effect of awareness of being monitored on wearing time and adherence -to wearing orthopaedic footwear. Quantitative assess-ment of wearing time was made using direct measure-ment with temperature sensors during the first 3 months after provision of footwear.
Design: Randomized controlled trial.
Intervention: Awareness that the temperature sensor is used for measuring wearing time.
Methods: All 55 participants had a temperature sensor built into the medial arch of the left insole of their orthopaedic footwear. Participants were assigned randomly to either an “awareness group” (n = 25, mean age 67 years) and knew they were being monitored for wearing time, or a “no awareness group” (n = 30, mean age 65 years) and only knew their shoe temperature was being measured. Differences were assessed with a linear mixed model.
Results: Mean (standard deviation; SD) wearing time in the intervention group was 7.32 h/day (SD 4.2), and 6.11 h/day (SD 4.1) in the control group (p = 0.017). A significant interaction effect was found between awareness and pathology group on wearing time (p = 0.036). The difference was especially large (7.0 (SD 4.7) vs 2.4 (SD 2.2) h/day) in the subgroup of people with diabetes.
Conclusion: Awareness of being monitored increases wearing time and wearing of orthopaedic footwear.
Key words: orthopaedic footwear; wearing time; adherence; use; temperature sensor; awareness; Hawthorne.
Accepted Oct 7, 2020; Epub ahead of print Oct 23, 2020
J Rehabil Med 2020; 52: jrm00127
Correspondence address: Thijs Lutjeboer, Department of Rehabilitation Medicine, University of Groningen, University Medical Center Groningen, 9713GZ Groningen, The Netherlands. E-mail: t.lutjeboer@umcg.nl.
Doi: 10.2340/16501977-2759
Orthopaedic footwear is prescribed for people with a wide variety of foot problems. This footwear helps people to prevent (diabetic) foot ulcers, to reduce pain, and to support their feet when of a different shape. Even if the or-thopaedic shoes are technically perfect, they need to be worn to be effective. Temperature sensors, placed in the inlays, can be used to measure wearing time of ortho-paedic footwear. This study investigated the effect of awareness of being monitored on wearing time and wearing of orthopaedic footwear. Participants in the “Awareness group” (intervention) knew they were being monitored for wearing time. The control group only knew their shoe temperature was being measured. The results showed that having awareness of being monitored increases wearing time and wearing of orthopaedic footwear by 1 h per day. The increase was especially large (4 h per day) in the subgroup of people with diabetes.
Orthopaedic footwear is prescribed to patients with a wide variety of foot disorders. Goals of such footwear are: prevention of (diabetic) foot ulcers; reduction in pain; support of anatomical foot deformities, providing stability and mobility; and redistribution of plantar pressure (1–3). The effectiveness of footwear depends, among others, on the technical prescription and realization of the footwear. But, even when shoes are technically perfect, they need to be worn. The required wearing time depends on the specific goals of the footwear. For some patients this means the footwear should be worn all the time, e.g. for prevention of diabetic foot ulcers, while other patients may only have to use them during specific activities. In daily practice, the user should make an agreement with the prescribing professional(s) about the intended daily wearing time of the shoes. Adherence is defined as the ratio of the actual wearing time of footwear to the intended wearing time. When the shoes are used in accordance with the intended wearing time, adherence is optimal (or 100%) (4). Both actual wearing time and adherence are important parameters when studying the efficacy of orthopaedic footwear.
Wearing time of footwear can be measured in, for example, h per day or days per week. Up to 2013, wearing time has been assessed with questionnaires, interviews or diaries (3, 5–16). These methods are all based on patients’ self-report and are therefore subjective and at risk of poor accuracy (17, 18). Due to technical developments, the use of temperature measurements as an objective method to quantitatively measure wearing time of orthopaedic footwear has become available (19–22). In studies applying this, patients were told that a sensor was placed in their footwear, but they were no informed about the goal of the sensor (19–22). This was done to avoid influencing patient’s wearing time by making them aware of the study purposes, known as the Hawthorne effect (23). However, it is unknown if awareness of being monitored has an effect on wearing time.
It is important to investigate the effect of awareness on being monitored on wearing time, as this has consequences for research and clinical practice. If such an effect is not present, it means that patients do not have to be kept uninformed of study-specific goals. On the other hand, if such an effect is present, it means that researchers should indeed be careful in disclosing the actual goal when asking for informed consent, to avoid influencing the outcome under study. But that also implies that simply putting a sensor in someone’s orthopaedic footwear and telling them they are being monitored might improve wearing time. That is an important outcome for clinical practice, as there are currently limited interventions known to improve adherence (24).
The primary aim of this study was to investigate the effect of awareness of being monitored on wearing time and wearing of orthopaedic footwear, with quantitative assessment of wearing time through direct measurement with temperature sensors, during the first 3 months after provision of footwear. We hypothesize that awareness about being monitored regarding wear-ing time will affect the subjects’ behaviour towards increased wearing time. Furthermore, this study aimed to investigate wearing time and wearing with regards to different pathologies.
The study was part of a larger project and received clearance from the Medical Ethical Committee (UMCG METc: 2016.512, Groningen, the Netherlands). All subjects gave their informed consent before participating. This trial was registered in Netherlands Trial Register (NL6186).
Participants
The inclusion criteria were: receiving a first pair of orthopaedic footwear at the subjects’ orthopaedic footwear company, being 18 years of age or older, being cognitively capable of completing a questionnaire and understanding the Dutch language. “Orthopaedic footwear” was defined as: “custom-made shoes and medical grade shoes with orthopaedic/pedorthic adaptations” (25).
Eleven orthopaedic footwear companies, from across the Netherlands, approached their patients for participation in this study. If a patient met the inclusion criteria, the orthopaedic shoe technician would inform the patient and ask, during the first contact, whether the patient wanted to read the general information about the study (see Appendix I, and see below under “Intervention”). If the patient was interested, an information package containing information about the study and an informed consent form was provided. The patient had the opportunity to read the information about the study and to consult the researcher or an independent physician before deciding to participate and providing their informed consent.
Based on the participants’ pathology, they were divided into 5 groups: diabetes mellitus, rheumatic diseases, degenerative foot disorders, central neurological disorders, and other pathologies.
Sample size
There are no data available in the literature on use of orthopaedic footwear where similar interventions were applied. Therefore no a priori power analysis was possible. The number of participants needed to test the effect of a simple intervention (in this case awareness of being monitored on wearing time) is estimated as approximately 100 per intervention group based on Kline (26). A sample size of 100+10% was chosen for both the “Awareness” group and “No awareness” group. This resulted in a target sample size of 220.
Temperature sensor
A small (9 × 13 × 4.5 mm) and dust- and water-tight temperature sensor (Orthotimer, Balingen, Germany; http://www.orthotimer.com), built into the insole of a person’s footwear, was used to measure the temperature inside the footwear. Time, date, and temperature were stored every 15 min and the sensor was equipped with a ring buffer with 100 days of storage capacity. The sensor has a temperature precision of ±0.1°C, Quartz-controlled time measurement, and wireless data transfer via radio frequency identification (RFID) technology (ISO 15693). The sensor is powered with a lithium dry cell battery (3.0 V/5.5 mAh) with a lifespan of at least 18 months. All of these components are moulded in a plastic casing that provides stability against high pressure. The sensor has been validated for measuring use and non-use of orthopaedic footwear (21).
The sensor data were collected at 6 and 12 weeks after delivery of the footwear with a wireless reading device (Orthotimer, Balingen, Germany) that transferred the data to the accompanying software on the computer. The reading device and computer were connected via a USB plug. The sensor, reader, and software are CE Class 1 (MDD 2007/47/CE) and Food and Drug Administration (FDA) approved.
Study design
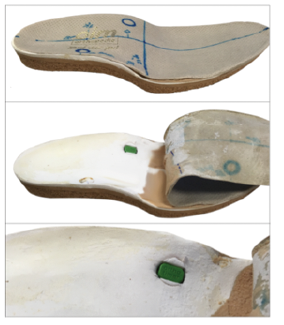
All participants had a temperature sensor built in the medial arch of the left insole of their orthopaedic footwear (Fig. 1). Before the delivery of their footwear, the participant was asked to complete the pre-version of the Monitor Orthopaedic Footwear (Monitor Orthopedisch Schoeisel; MOS) Questionnaire (27). This questionnaire was developed to identify factors that influence the use and usability of orthopaedic footwear and comes in a pre- (expectations of the user; MOS-pre) and a post- (experience of the user; MOS-post) version. Participants were also asked to complete the intended wearing time of their footwear. After 6 and 12 weeks, participants were asked to complete MOS-post. Appointments with the footwear company were scheduled 6 and 12 weeks after delivery of the footwear to check whether small adjustments had to be made to the footwear and to collect the data from the sensor.
Fig. 1. Custom-made inlay with built-in sensor.
Intervention
The general information letter provided to all participants stated that they participated in a study on “effectiveness and use of orthopaedic footwear” (see specific quote in Appendix I). They were informed of the involvement of a temperature sensor, but it was not specified or explained that this sensor could be used to measure footwear use and non-use. After the participants gave their written informed consent, they were randomly allocated to either the “No awareness” group (control) or the “Awareness” group (intervention) using the “rand” function in Matlab, using blocks based on participant’s pathology group. Participants in the “Awareness” group received additional information via postal letter or e-mail before their footwear was delivered (see quote in Appendix II). With this letter, these participants knew the purpose of the study: measuring the exact wearing time of their orthopaedic footwear. As such, these participants knew they were being monitored for wearing time. The letter also stated that they should not discuss the function of the sensor in the waiting room of their orthopaedic footwear company throughout the length of the study.
Wearing time
The collected temperature data were exported into Matlab (2014b The MathWorks, Inc, Natick, Massachusetts, USA). We used our previously developed and validated Groningen Algorithm to calculate wearing time based on the temperature measurements (23). Mean daily wearing time from weeks 6 to 12 was calculated as the primary outcome measure. The first 5 weeks were not included in the analyses, because we see this as a period to become familiar with the new footwear.
Adherence
Participants were asked to answer the following questions in MOS:
Based on the answers, an mean intended daily use was calculated. The actual use was obtained from the mean use in weeks 6 to 12, as measured with the sensor. Adherence was the ratio between intended use and actual use, expressed as a percentage. Adherence to wearing orthopaedic footwear has only been investigated quantitatively in people at-risk of diabetic foot ulcers (21, 22), where intended use was defined as “wearing the footwear 100% of the steps taken”. “Being adherent” was, in these studies, defined as an adherence of 80% or more. Based on these studies and our expert opinion, we chose to define 3 categories in the current study: non-adherent (<80%); adherent (80–120%); and super-adherent (>120%). The latter category was added, because, with our definition, patients can be wearing their shoes more hours per day than their intended use.
Statistical analysis
Descriptive statistics were used to describe the groups. Plots were made between week numbers (weeks 6–12 on x-axis) and wearing time (on the y-axis) for the potential predictors. Based on visual inspection of the plots, the independent variables awareness, sex, pathology and age were entered in a linear mixed model analysis (autoregressive first order covariance structure) with use (i.e. mean wearing time in hours per day) as a dependent variable. A predictor was removed from the analysis if the regression coefficient was not significant (p > 0.05). In SPSS (IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.), interaction effects were explored and residuals were checked for a normal distribution.
In total, 224 participants gave their informed consent (Table I and Fig. 2). Of these, 130 participants had a sensor built into their footwear, while 94 participants did not start the study because either no sensor was built into their footwear or they changed their mind after providing informed consent. The exact reasons for not starting, not building in the sensor, or not showing up are unknown and could not be registered. Data from 18 participants was not available because they did not return within the first 12 weeks, while 57 participants did not have a complete dataset for weeks 6 to 12, leaving 55 participants included in the study. Their characteristics are shown in Table I, and were similar to other studies in this population (6).
Table I. Participants’ characteristics
Participants with awareness had an mean wearing time of 7.32 h per day during weeks 6–12 (Fig. 3 and Table II), while those without awareness had an mean wearing time of 6.11 h per day, p = 0.017 (Table III). A significant interaction effect was found between awareness and pathology group on wearing time; p = 0.036 (Table III). This interaction effect means that the effect of awareness on footwear use was different for the pathology groups. The group with other pathologies was chosen as a reference category because it contained a mixture of multiple pathologies. Compared with the reference category, awareness increased wearing time for the other 4 groups (participants with diabetes mellitus, rheumatic diseases, degenerative foot disorders, and central neurological disorders; Table II).
Fig. 2. Patient flowchart.
Table II. Mean (standard deviation; SD) of the mean daily wearing time for participants with “No awareness” and “Awareness” for all groups and each individual pathology group
Fig. 3. Mean daily wearing time for participants with “No Awareness” and “Awareness” for all groups (large graph) and for each pathology group (5 small graphs).
Table III. Multilevel analysis for wearing time
A total of 33 participants completed MOS and reported their intended wearing time as hours of footwear use per day. Based on intended and actual wearing time, 18 participants were classified as non-adherent (< 80%), 9 as adherent (80–120%), and 6 as super-adherent (> 120%); see Fig. 4. Of the (super-)adherent participants, 60% had awareness of being monitored (9 out of 15); of the non-adherent participants, 39% had awareness (7 out of 18). The 18 non-adherent participants consisted of 5 (out of a total 7) participants with diabetes mellitus, 2 (out of 3) participants with rheumatic diseases, 6 (out of 10) participants with degenerative foot disorders, 3 (out of 6) participants with central neurological disorders and 2 (out of 7) participants with other pathologies (Fig. 4).
Fig. 4. Adherence, as ratio between intended wearing time and actual wearing time. Three categories: non-adherent (< 80%), adherent (80–120%), and super-adherent (> 120%).
Increasing wearing time of orthopaedic footwear is important, as footwear can only be effective when it is being worn. This study investigated whether awareness of being monitored for wearing has an effect on wearing time of orthopaedic footwear. We found that participants with awareness wore their footwear on mean 1 h more each day than control subjects in the period 6–12 weeks after provision. This suggests the presence of a Hawthorne effect (23). However, with the small numbers of participants for whom a complete dataset was available and the heterogeneity of the population (with multiple disorders included), the results should be seen as an indication and warranting further exploration.
Examining the effect of awareness between pathology groups, this study found that awareness increased daily wearing time in 4 of the 5 pathology groups, with only the group with a mixture of “other pathologies”’ showing a reversed effect. We cannot explain the reversed effect in this group, given the heterogeneity within this group. However, for the 4 pathology groups inclusive of only one pathology, a consistent effect of increased wearing time was found in participants with awareness of being monitored. Furthermore, the large variability in wearing time between and within groups was striking. Large standard deviations found indicate that large differences exist between participants. Despite this, statistically significant differences were found in multilevel analyses, with residuals checked for normality. We therefore still expect these results to be generalizable to larger populations.
The wearing time patterns of the total “Awareness” and “No Awareness” groups appear to be similar and stable over the weeks; however, if we zoom into the graphs and patterns of the individual pathology groups, it can be seen that wearing time changes per week. These differences between consecutive weeks indicate that measuring one week of wearing time might not be representative for a longer period of time. In previous research, one week of quantitative measuring of footwear use has been the maximum to date (18, 19).
The most vulnerable group are people with diabetes, being at high risk of foot ulceration and amputation. The difference in wearing time between the “Awareness” and “No awareness” groups was especially large in these patients; those with awareness had 4 h higher mean wearing time. An mean wearing time of 2.42 h a day for the “No Awareness” group is clearly insufficient to prevent an ulcer. And even though the “Awareness” group had a wearing time of 6.95 h a day, this may still not be enough to prevent foot ulcers if these patients are active outside these hours. Even more worrying in this group were participants’ answers regarding the required wearing time, with some of them indicating that less than 6 h wearing per day would be sufficient. This suggests a need for better education and more time from professionals to discuss adequate adherence in this population.
Study limitations
A major limitation of this study was the large dropout. While the sample size of 55 participants still allowed us to perform explorative multilevel analyses, the results should be interpreted with caution. The dropout was caused by a number of reasons, some known and others unknown. Probably the most important reasons for dropout were a difficult organization of the study. Orthopaedic footwear companies had to ask participants and had to build in the sensors, with both steps taking them more time than anticipated at the start of the study. Furthermore, participants experienced the extra visit required to read-out the sensor at 6 weeks as a burden, and a reason to decline to participate (or simply not show up). Apart from sex and age (which did not differ from those who participate), we were unfortunately not able to investigate other characteristics of dropouts. While involvement from commercial companies in recruitment might be seen as a limitation, we have cooperated with these companies in previous research successfully (with >500 participants recruited), and have not seen indications for selection bias in recruitment (8). We therefore have no reason to assume that this may have played a role in the current recruitment.
A minor limitation was that wearing time measured in this study did not differentiate between activity (sitting, standing, walking). However, Waaijman et al. (20) found a high correlation between wearing time (all wearing time – sitting, standing, walking) and adherence (weight-bearing steps) (20).
Another limitation was the unequal distribution between the pathology groups in the intervention and control group, and the relatively small numbers per category. However, since almost all 11 participants with diabetes mellitus had very limited wearing time, we argue that the conclusions about the absolute wearing time in this subgroup have validity. Furthermore, not all participants completed the questionnaire about their intended use. In some cases, participants completed “use all day” without specifying a number. These cases were excluded from the analysis.
This study was limited to patients receiving their first-ever pair of orthopaedic footwear (or their first pair of orthopaedic footwear at that specific orthopaedic footwear company), and to weeks 6–12 after provision of this footwear. It is unknown if the effect of being monitored will last beyond the first 3 months. However, the wearing time patterns throughout weeks 6–12 were relatively stable, suggesting that it might carry forward. Longer-term follow-up of patients is needed in future research, and investigation of seasonal influences.
Having awareness of being monitored may increase wearing time and adherence to use of orthopaedic footwear. This is important to take into account in future studies on footwear adherence, as researchers and clinicians should carefully consider how to instruct their patients. For clinical practice, it suggests that mon-itoring might be an intervention to improve wearing time of footwear, when patients are made aware that they are being monitored. However, mean use was still only 7 h per day, and many participants remained non-adherent; hence additional interventions to improve adherence are needed.
Appendix I. Quote from information letter to the participants.
Appendix II. Quote from information letter to the participants


 Click to show fullsize
Click to show fullsize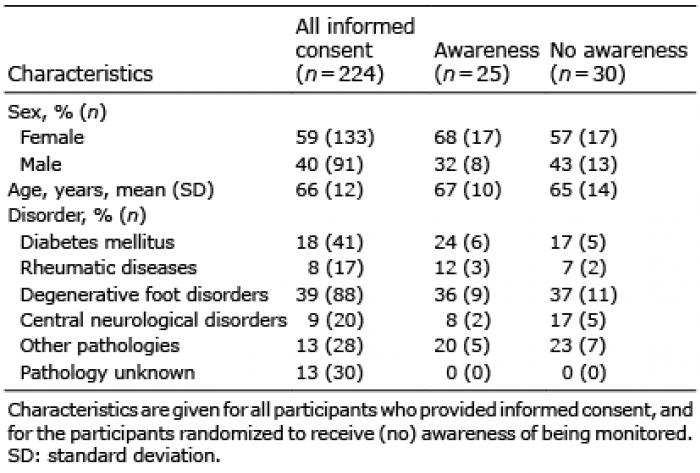 Click to show fullsize
Click to show fullsize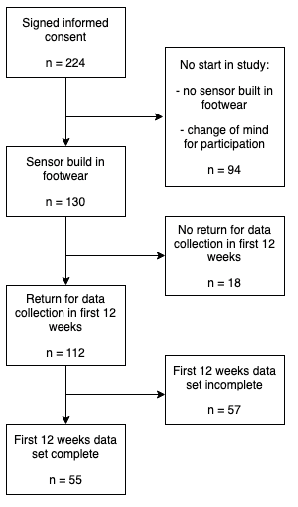 Click to show fullsize
Click to show fullsize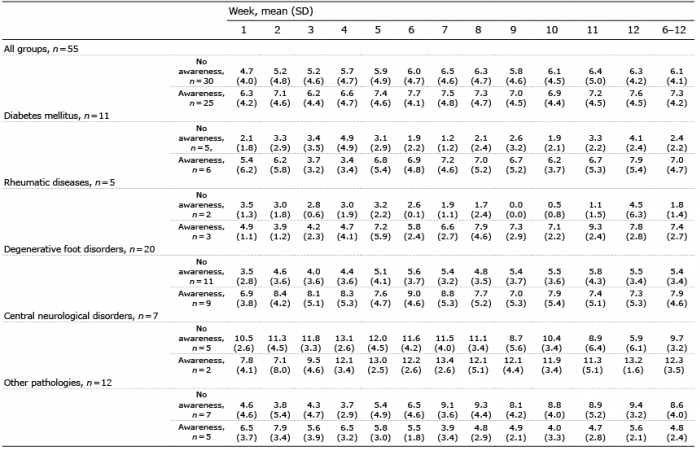 Click to show fullsize
Click to show fullsize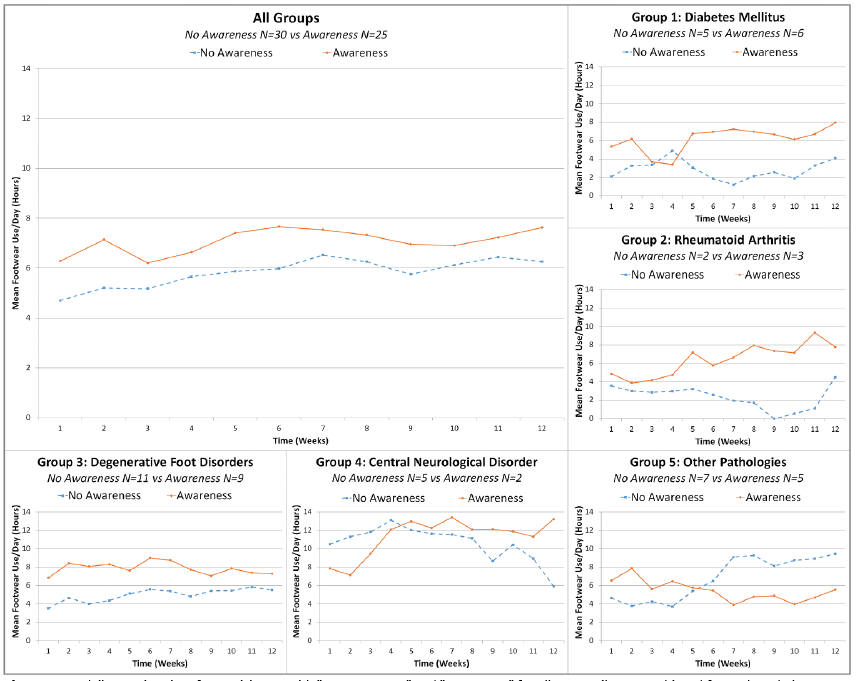 Click to show fullsize
Click to show fullsize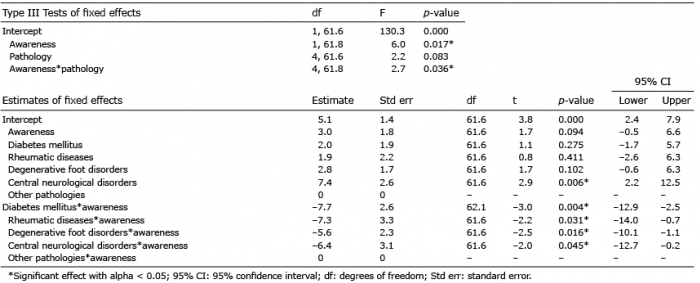 Click to show fullsize
Click to show fullsize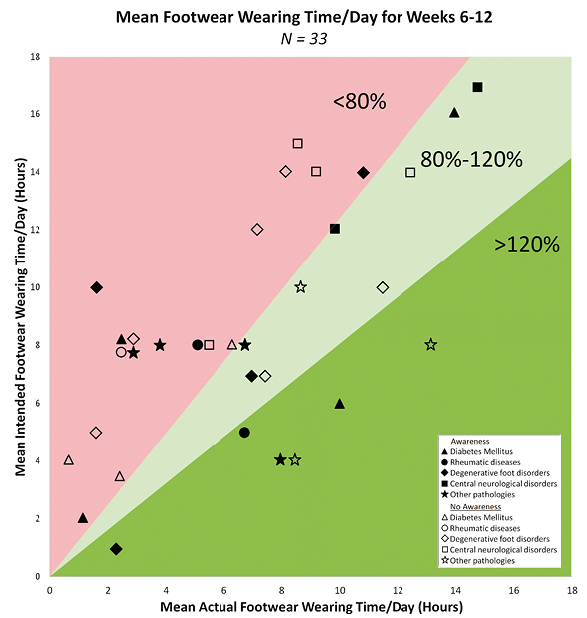 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize