
From the Department of Rehabilitation Medicine, Shenzhen Children’s Hospital, Shenzhen, China
Objective: The results of previous research into exercise interventions for children with cerebral palsy are inconsistent. The aim of this study is to assess the effectiveness of such exercise interventions.
Design: Systematic review and meta-analysis.
Methods: Systematic searches of the PubMed, Embase and Cochrane Library databases for randomized controlled trials involving exercise interventions for children with cerebral palsy, from inception to January 2020, were performed. Pooled weighted mean differences (WMDs) with 95% confidence intervals (95% CI) for gross motor function, gait speed, and muscle strength were calculated using random- effects models.
Results: A final total of 27 trials, including 834 children with cerebral palsy, were selected for quantitative analysis. Exercise interventions had no significant effect on the level of gross motor function (WMD 1.19; 95% CI −1.07 to 3.46; p = 0.302). However, exercise interventions were associated with higher levels of gait speed (WMD 0.05; 95% CI 0.00–0.10; p = 0.032) and muscle strength (WMD 0.92; 95% CI 0.19–1.64; p = 0.013).
Conclusion: These results suggest that exercise interventions may have beneficial effects on gait speed and muscle strength, but no significant effect on gross motor function in children with cerebral palsy.
Key words: cerebral palsy; child; exercise; meta-analysis; systematic review.
Accepted Nov 9, 2020; Epub ahead of print Nov 23, 2020.
J Rehabil Med 2021; 53: jrm00176
Correspondence address: Guojun Yun, Department of Rehabilitation Medicine, Shenzhen Children’s Hospital, Shenzhen, China. E-mail: 1440177232@qq.com
Doi: 10.2340/16501977-2772
Cerebral palsy is the most common cause of physical impairment in children. This study evaluated the effectiveness of exercise interventions for children with cerebral palsy. Exercise interventions were significantly associated with increased gait speed and muscle strength, while gross motor function was not affected. Exercise interventions should therefore be used for children with cerebral palsy.
Cerebral palsy is the most common cause of physical impairment in children and is characterized by gait abnormalities (1–3). The characteristics of cerebral palsy are associated with damage to the immature brain, which causes subsequent primary impairments, including decreased muscle tone, loss of selective motor control, and impaired balance. Secondary impairments include muscle shortening or weakness and decreased range of motion (4, 5). The prevalence of cerebral palsy is approximately 2.1 in every 1,000 births, and children account for 74% of cases worldwide (6, 7). Children with cerebral palsy are significantly affected by epilepsy and by disorders in motor function, sensation, perception, communication, and behaviour, which significantly affect quality of life and result in huge economic and psychological burdens (8–11).
Currently, the primary therapeutic goals for cerebral palsy are aimed at improving mobility and upper limb function (12). Exercise interventions may also play an important role in improving muscle strength, endurance, and cardiorespiratory fitness. Several systematic reviews and meta-analyses have illustrated the potential role of exercise interventions for children with cerebral palsy; however, results regarding gross motor function, gait speed, and muscle strength are inconsistent (13–15). Exercise programmes usually include resistance and/or aerobic training. Children with cerebral palsy have reduced muscle strength, and resistance exercise can maintain or increase muscle performance (16, 17), while aerobic training can improve cardiorespiratory fitness. Studies have found that muscle stretching can increase range of motion (18, 19). It is important to clarify the effectiveness of exercise interventions for treatment of cerebral palsy in children, and to determine the role of the type of training for children with cerebral palsy. A meta-analysis of randomized controlled trials (RCTs) of exercise interventions for children with cerebral palsy was therefore performed in order to assess the effectiveness of this treatment.
Data sources, search strategy, and selection criteria
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement was applied to guide this meta-analysis (see checklist, Table SI) (20). The study was designed as a meta-analysis of RCTs, with the aim of determining the effectiveness of exercise interventions for children with cerebral palsy. No restrictions were applied regarding published language and status of RCTs. The electronic databases of PubMed, EmBase, and Cochrane Library databases were systematically searched from their inception to January 2020. The core search terms were “cerebral palsy” AND “exercise” AND “randomized controlled trial”. Details of the search strategy for each database are shown in Appendix S1. The reference lists of relevant reviews or original articles were also searched manually to select any new eligible studies.
The literature search and study selection was conducted following a standardized flow, comprising 3 steps: (i) an initial literature screening, through reviewing title and abstracts, was conducted separately by 2 of the authors of this paper (ZT and GY); (ii) inconsistencies between author findings were checked and discussed; (iii) the full text of retrieved studies were independently reviewed by 2 authors (XL and JC), and inconsistency between authors was discussed to reach a consensus. The inclusion criteria for this meta-analysis was based on PICOS criteria: (i) Patients: children (< 18.0 years of age) with cerebral palsy, and diagnosed criteria of cerebral palsy was based on individual trial; (ii) Intervention: exercise intervention with no restrictions placed on exercise programme; (iii) Control: usual care, including background treatment and exercise strategies, which was also given in the intervention group; (iv) Outcomes: gross motor function, gait speed, and muscle strength; and (v) Study design: RCTs only. Studies designed as observational studies were excluded owing to various confounding factors that could overestimate the treatment effectiveness.
Data collection and quality assessment
Two authors (XL and JW) independently extracted the data from the included studies, and any disagreement was settled by group discussion. The extracted information included first authors’ surname, publication year, country, sample size, mean age of patients, percentage of male patients, disease status, measurement tool, intervention, control, follow-up duration, and reported outcomes. The Eastern countries was defined as East and Central Asia, and the Western countries including Europe, Australia, America, and South Africa. Study quality was assessed with the Jadad scale, which is based on randomization, concealment of the treatment allocation, blinding, completeness of follow-up, and use of intention-to-treat analysis (21). The Jadad scale ranges from 0 to 5, and studies scoring 4 or 5 were regarded as high quality.
Statistical analysis
The investigated outcomes were assigned as continuous data, and the weighted mean differences (WMDs) with 95% confidence intervals (95% CIs) was calculated based on mean, standard deviation (SD), and sample size for each individual trial. Then, the pooled WMDs and 95% CIs for gross motor function, gait speed, and muscle strength were calculated using the random-effects model (22, 23). I2 and p-value for Q statistics were applied to assess the heterogeneity across included trials, and I2 > 50.0% or p < 0.10 was considered as significant heterogeneity (24, 25). Sensitivity analyses for gross motor function, gait speed, and muscle strength were conducted by excluding trials one by one, and then performing a pooled analysis of the remaining studies using the random-effects model (26). Subgroup analyses for gross motor function, gait speed, and muscle strength were conducted on the basis of country, mean age, proportion of male subjects, exercise type, follow-up, and study quality. The difference between subgroups was then assessed by interaction p-test (26). Publication biases were assessed by both qualitative (funnel plot) and quantitative (Egger and Begg tests) methods (27, 28). The inspection level for pooled outcomes are 2-sided, and p < 0.05 was regarded as statistically significant. STATA software (version 10.0; Stata Corporation, College Station, TX, USA) was used to conduct all statistical analyses.
Literature search
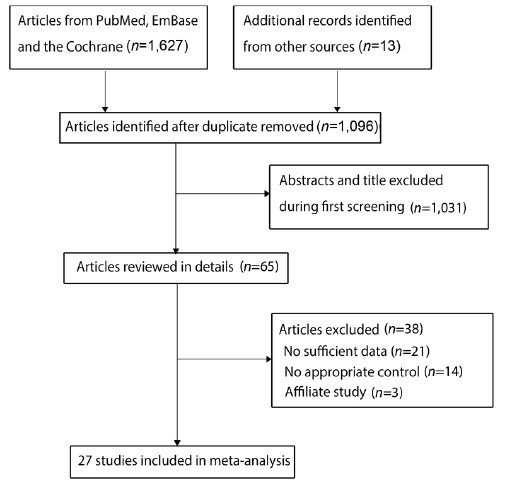
A total of 1,627 articles were identified from electronic searches, and 531 were excluded owing to duplicate topics. A total of 1,031 articles were excluded due to irrelevancy. A total of 65 studies were retrieved for further full-text evaluations, and 38 studies were excluded due to either insufficient data (n = 21), no appropriate control (n = 14), or affiliate study (n = 3). No new relevant reviews or original articles were found through manual searches of the reference lists. As a result, a final total of 27 RCTs met the inclusion criteria and were selected for the meta-analysis (29–55). Details of the literature search and study selection are shown in Fig. 1.
Fig. 1. Flow diagram of study selection process.
Study characteristics
The baseline characteristics of the included studies are summarized in Table I. A total of 834 children with cerebral palsy were included from 27 separate trials. The included studies were all published between 2003 and 2019, and between 12 and 101 children were included in each individual trial. The mean age of included children ranged from 1.8 to 16.0 years, and the follow-up duration ranged from 1 to 12 months. Twenty-one studies were conducted in Western countries, while the remaining 6 studies were conducted in Eastern countries. Five trials scored 4 on the Jadad scale, 7 trials scored 3, 6 trials scored 2, and the remaining 9 trials scored 1 (Table II).
Table I. Characteristics of studies included in the meta-analysis
Table II. Quality assessment of included studies
Gross motor function
Data regarding the effect of exercise intervention on gross motor function were available in 17 of the selected trials. There was no significant difference between exercise and control for the level of gross motor function (WMD 1.19; 95% CI −1.07 to 3.46; p = 0.302; Fig. 2), and no evidence of heterogeneity was detected (I2= 0.0%; p = 0.998). The conclusion was robust and not altered by sequential exclusion of individual trials (Table III, Appendix S2). The results of subgroup analyses were consistent with the overall analysis in all subsets (Table IV). No significant publication bias for gross motor function was detected (p-value for Egger 0.738; p-value for Begg 0.174; Appendix S3).
Fig. 2. Effect of exercise intervention on gross motor function in children with cerebral palsy. 95% CI: 95% confidence interval.
Table III. Effect of exercise intervention on gross motor function, gait speed, and muscle strength when a study is omitted
Gait speed
Data regarding the effect of exercise intervention on gait speed were available in 16 of the selected trials. Exercise intervention was associated with higher gait speed than those in control groups (WMD 0.05; 95% CI 0.00–0.10; p = 0.032; Fig. 3), and non-significant heterogeneity was detected across these trials (I2 = 29.6%; p = 0.127). This conclusion was altered when excluding the studies conducted by Fowler et al., 2010 (37), Gharib et al., 2011 (40), Smania et al., 2011 (42), Pandey et al., 2011 (44), Chrysagis., 2012 (45), or Peungsuwan et al., 2017 (52) (Table III, Appendix S2). Subgroup analysis revealed that a more significant effect of exercise intervention on gait speed was detected if the study was conducted in an Eastern country, if follow-up was< 6.0 months, and in studies with lower quality (Table IV). There was no significant publication bias for gait speed (p-value for Egger 0.541; p-value for Begg 0.893; Appendix S3).
Fig. 3. Effect of exercise intervention on gait speed in children with cerebral palsy. 95% CI: 95% confidence interval.
Table IV. Subgroup analyses for investigated outcomes
Muscle strength
Data for the effect of exercise intervention on muscle strength were available in 17 trials. The pooled result found exercise intervention was associated with an improvement in muscle strength (WMD 0.92; 95% CI 0.19–1.64; p = 0.013; Fig. 4), and significant heterogeneity was seen among the included trials (I2 = 83.7%; p < 0.001). This conclusion was changed into non-significant difference after excluding the study conducted by Pandey et al., 2011 (44) (Table III, Appendix S2). Subgroup analyses revealed that the significant effect of exercise intervention on muscle strength was observed mainly when the proportion of males was ≥50%, when patients had received resistance training, and when follow-up was < 6.0 months, and in studies with lower quality (Table IV). No significant publication bias for muscle strength was detected (p-value for Egger 0.115; p-value for Begg 0.387; Appendix S3).
Fig. 4. Effect of exercise intervention on muscle strength in children with cerebral palsy. 95% CI: 95% confidence interval.
This meta-analysis of RCTs of children with cerebral palsy assessed the effectiveness of exercise interventions on gross motor function, gait speed, and muscle strength in these patients. The quantitative analysis was based on 834 children with cerebral palsy from 27 RCTs, and the broad characteristics of patients were included. The meta-analysis revealed that exercise interventions are not associated with improved gross motor function in children with cerebral palsy, but were associated with increased gait speed and muscle strength. Meta-analysis also revealed that the effect of exercise intervention on muscle strength could be affected by country, mean age, proportion of male subjects, exercise type, and study quality.
Several systematic reviews and meta-analyses have been conducted previously to investigate the effectiveness of exercise interventions for patients with cerebral palsy. Bania et al. conducted a meta-analysis of 9 studies to investigate the effect of activity training in children with cerebral palsy (13), and reported that activity training did not result in significant effects on activity or participation. A meta-analysis by Booth et al., based on 11 RCTs, found that functional gait training conferred a significant increase in walking speed in children and young adults with cerebral palsy (14). A Cochrane review found that aerobic exercise could improve gross motor function, but did not affect gait speed, and that resistance training did not result in any beneficial effect on gait speed, gross motor function, participation, or quality of life in children with cerebral palsy (15). However, several outcomes were not addressed in Bania et al.’s study (13), and the other 2 studies included both children and adults (14, 15). Several additional studies have since been published, which should be taken into account when evaluating the effectiveness of exercise interventions for children with cerebral palsy.
Although the results of the current meta-analysis showed that exercise intervention has no significant effect on gross motor function, a trend of improvement was observed in the pooled conclusion and sensitivity analysis. All the studies included in the meta-analysis reported similar results, and no significant difference in the level of gross motor function between the exercise and control groups. Potential reasons for these results are that the effectiveness of exercise interventions on gross motor function could be affected by the type and intensity of the exercise programme, the amount of exercise could be affected by the age of the children, and the effectiveness of exercise interventions could be affected by compliance and by guardians. These factors could induce potential non-significant differences for children after long-term exercise interventions.
This meta-analysis revealed that exercise intervention could significantly increase gait speed in children with cerebral palsy. Most studies reported no significant effect of exercise intervention on gait speed, but 2 of the included trials reported a conclusion similar to the pooled conclusion. Pandey et al. found that task-specific strength training of the lower limbs was associated with a significant increase in gait speed after one month (44). The study conducted by Chrysagis et al. included 22 adolescents (age range 13–19 years) and found that a treadmill programme was associated with increased gait speed compared with conventional physiotherapy (45). The potential reason for this is that manual correction by the physical therapist could enhance walking ability, and the exercise programme involved repetitive movements in the lower limbs during training (56). Moreover, the change in weightbearing from the pelvis could improve hip extension, knee collapse, and foot clearance (56). Sensitivity analysis found that the pooled conclusion was not stable after sequentially excluding individual trials. The potential reason for this could be the lower or upper limit of 95% CI was close to zero and further RCTs are needed to verify this result.
The pooled results of this study reveal that exercise interventions are associated with increased muscle strength in children with cerebral palsy. Although most included trials reported that exercise interventions had no significant effect on muscle strength, 4 of the studies found that exercise intervention could significantly increase muscle strength. Scholtes et al. found that children with 12 weeks of functional progressive resistance exercise had increased muscle strength (39). Pandey et al. reported that task-specific strength training of the lower limbs could significantly increase muscle strength (44). Mitchell et al. found that web-based training for activity capacity and performance could significantly increase functional strength and walking endurance in children with unilateral cerebral palsy (57). Peungsuwan et al. reported that children with cerebral palsy had increased muscle strength after following a combined strength and endurance training programme (58). Subgroup analyses revealed that exercise intervention significantly enhanced muscle strength when the proportion of males was ≥50%, when patients received resistance training, when follow-up was < 6.0 months, and in studies with lower quality. These results could be explained by the amount of exercise, and the type of exercise programme is significantly related to the increased muscle strength. Moreover, the effect of exercise intervention was more evident after shorter follow-up. , the results of this study should be recommend cautiously because of the significant difference between groups was observed in the subgroup of studies with low quality.
Study limitations
This study has several limitations. First, the types of exercise intervention were different across included trials, making direct comparisons problematic. Secondly, the disease status ranged from I to V (Gross Motor Function Classification System; GMFCS), and there were differences in baseline gross motor function, gait speed, and muscle strength. Thirdly, the heterogeneity for muscle strength among the included trials was not fully explained by sensitivity and subgroup analyses. Fourthly, most of the included trials had low to moderate quality, and the results of these studies should be viewed with caution. Finally, meta-analyses based on pooled data have inherent limitations, including inevitable publication bias and restricted details.
This study found that exercise interventions in children with cerebral palsy were significantly associated with increased gait speed and muscle strength, but had no significant effect on gross motor function. Further large-scale RCTs are needed to verify the findings of this study.
This study was supported by Research on the application of integrated services for the disabled (four square step test; FSST), grant number JB2017-16-2.
The authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize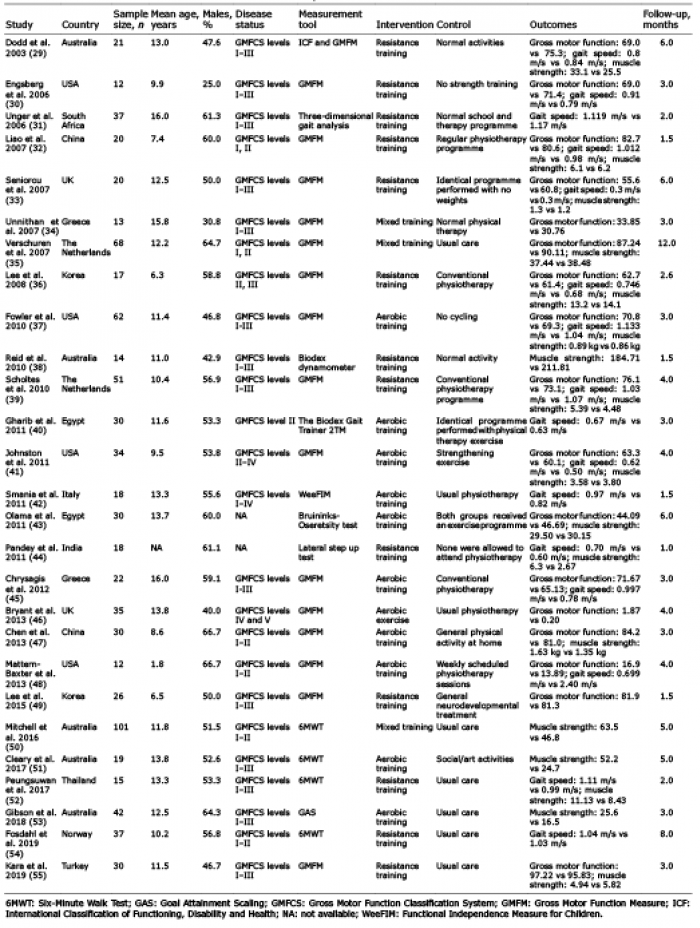 Click to show fullsize
Click to show fullsize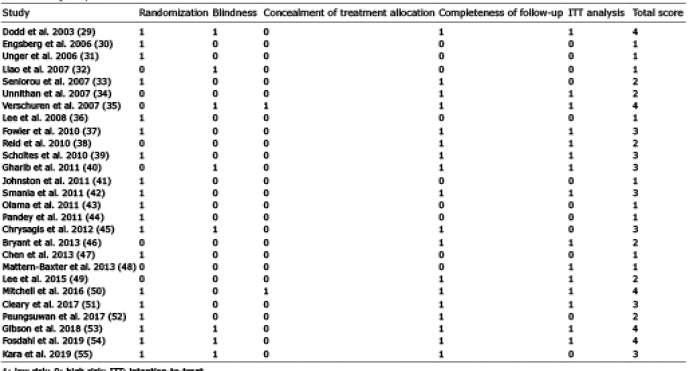 Click to show fullsize
Click to show fullsize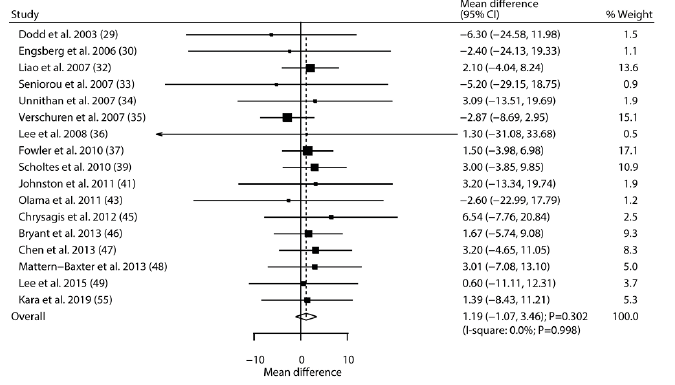 Click to show fullsize
Click to show fullsize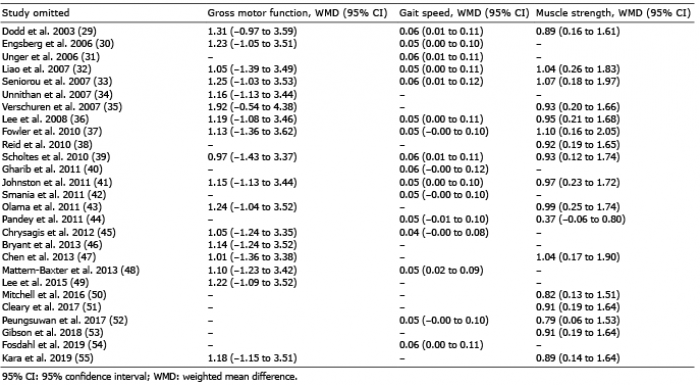 Click to show fullsize
Click to show fullsize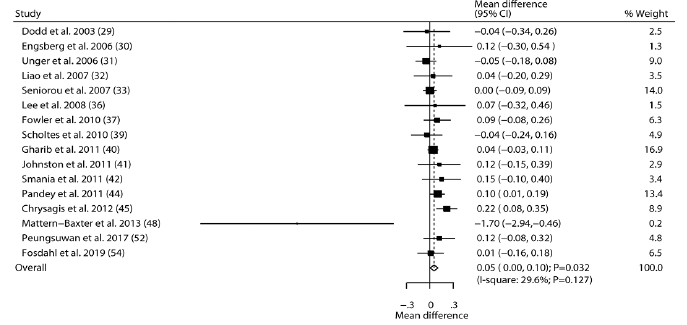 Click to show fullsize
Click to show fullsize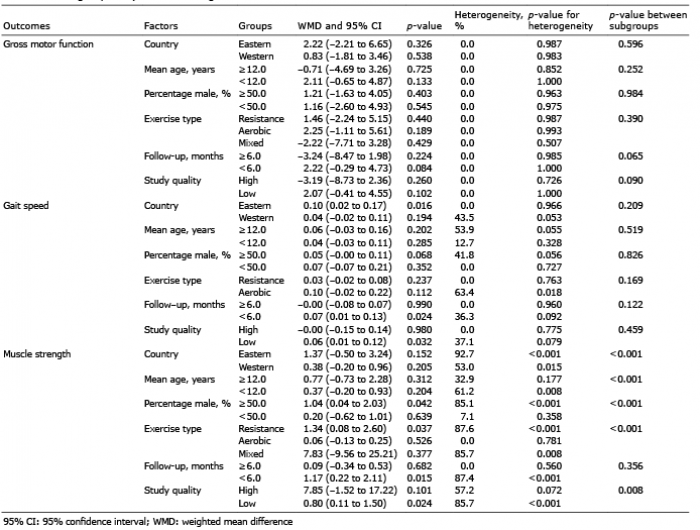 Click to show fullsize
Click to show fullsize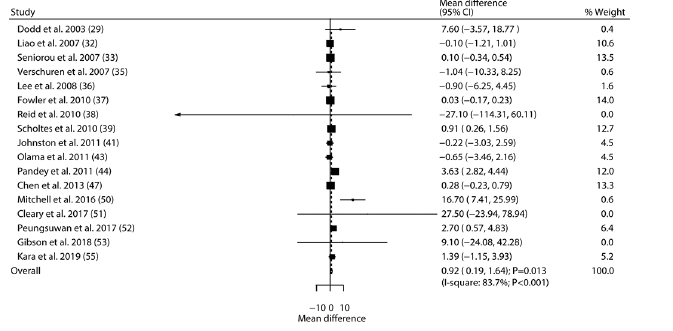 Click to show fullsize
Click to show fullsize