LAYING THE FOUNDATION FOR A PRIMARY CARE CORE SET OF THE INTERNATIONAL CLASSIFICATION OF FUNCTIONING, DISABILITY AND HEALTH (ICF) FOR COMMUNITY-DWELLING OLDER ADULTS: A QUALITATIVE STUDY

From the 1Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Institute of General Practice, 2Center for Health Services Research in Medicine, Department of Psychiatry and Psychotherapy, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Erlangen and 3Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Institute for Biomedicine of Aging, Nuremberg, Germany
Objective: To explore relevant areas of functioning from the perspective of community-dwelling adults aged 75 years and over, in order to develop a Core Set of the International Classification of Functioning, Disability and Health (ICF) for community-dwelling older adults for use in primary care.
Design: Qualitative study using semi-structured interviews and focus groups.
Participants: A total of 27 community-dwelling older adults participated in the interviews and 24 of them in the focus groups.
Methods: Following the proposed methodology of the ICF Research Branch, this is 1 of 4 preparatory studies in the Core Set development process. Within the transcripts, concepts of functioning were identified, based on Mayring’s qualitative content analysis using deductive category assignment with the ICF being the category system.
Results: Overall 6,667 concepts were identified. Most were linked to the Activities and Participation component. The most frequently identified categories were “recreation and leisure” and “family relationships”.
Conclusion: Categories from all ICF chapters were identified, demonstrating the complexity and multidimensionality of the ageing process, with a special emphasis on the component Activities and Participation. This qualitative study provides a list of relevant categories from the perspective of community-dwelling elderly people, which will be used to develop a Core Set for older primary care patients.
Key words: International Classification of Functioning, Disability and Health; aged; independent living; interviews as topic; focus group; cross-sectional study; geriatric assessment/methods; general practice/methods.
Accepted Nov 26, 2020; Epub ahead of print Dec 15, 2020
J Rehabil Med 2021; 53: jrm00150
Correspondence address: Johanna Tomandl, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Institute of General Practice, Universitätsstraße 29, 91054 Erlangen, Germany. E-mail: johanna.tomandl@gmail.com
Doi: 10.2340/16501977-2779
Physicians usually focus on diagnosing and treating diseases. In old age this might be less appropriate, and other biopsychosocial aspects (e.g. independent living) should also be considered. Therefore, we aim to develop an International Classification of Functioning, Disability and Health Core Set for older adults, which physicians can use to assess these aspects during consultations. In the development process several perspectives should be considered; one of them being the view of the target group. To explore this view, interviews and group discussions were conducted with community-dwelling adults aged 75 years and over. Almost 200 relevant aspects of functioning were identified. Leisure activities, family relationships and mobility were mentioned most often. Body functions, which are normally in the focus of physicians, seem to be less important to older adults. The results suggest that including biopsychosocial information in the consultation might help to better tailor medical interventions to the patients’ needs.
Traditionally, medicine focuses on the diagnosis and treatment of single diseases. However, with increasing age the prevalence of chronic conditions and multimorbidity increases (1, 2). In Germany, 82% of women and 74% of men aged 75–79 years have 2 or more chronic diseases (3). In this population, the treatment of isolated diseases based on disease-specific guidelines might no longer be appropriate, as it almost inevitably leads to a situation of polypharmacy and overtreatment (4–6). Inappropriate or conflicting medication might, especially in old age, lead to negative outcomes, such as adverse drug events, increased risk of fractures, hospitalization, and even death (7–9). Moreover, the changes accompanying the ageing process “can result in health states in older age that are not captured by traditional disease classifications” (10, p. 26). Thus, in guidelines and recommendations on the treatment of older, multimorbid, patients, the consideration of functioning is suggested to determine treatment goals (5, 10–13). The term “functioning” can be defined as a person’s intrinsic health capacity, as well as what the person actually does or is not able to do in everyday life (10, 14, 15). Functioning is determined by the interaction between the health capacity on the one hand and environmental factors on the other (10, 14, 15). Information on functioning, together with information on disease might be a better discriminator between necessary and unnecessary medicine in older persons than disease information alone.
The International Classification of Functioning, Disability and Health (ICF) offers a common defined language for describing functioning from a biopsychosocial perspective (16). It was launched by the World Health Organization (WHO) in 2001 and has become an internationally recognized reference framework for health and health-related states. Within the ICF, functioning can be described using the components Body Functions, Body Structures, Activities and Participation, and is influenced by Environmental Factors and Personal Factors. With more than 1,400 categories, the ICF is, however, too extensive to be used in daily practice. The development of shorter lists of categories (Core Sets) is one way of addressing this issue (17). These ICF Core Sets comprise categories that cover the typical spectrum of functioning aspects relevant to persons living with a given condition (18). ICF Core Sets for primary care and for geriatric patients have already been developed (19–22). However, none of these were developed according to the recommended process for developing ICF Core Sets (18). Thus, we aim to develop an ICF Core Set, covering the life and functioning of community-dwelling adults aged 75 years and older, following this standard. It comprises 4 studies to identify relevant ICF categories from different perspectives: a systematic literature review (research perspective), this qualitative study (perspective of the target population), an expert survey (experts’ perspective), and an empirical cross-sectional study (clinical perspective). It is important to capture these different perspectives in the development process in order to gain a holistic understanding of the functioning of people living with a specific health condition.
The specific aims of this study are: (i) to identify concepts contained in interviews and focus groups conducted with community-dwelling older adults; and (ii) to link these concepts to the ICF.
A qualitative study was conducted with community-dwelling older adults aged 75 years and older, consisting of semi-structured interviews and focus groups. The study is part of the ICF project of the Preventing Overdiagnosis in Primary Care (PRO PRICARE) research network (www.propricare.de). A more detailed description of the ICF project was published previously (23). The study is registered in Versorgungsforschung Deutschland Datenbank (VfD_17_003833) and in clinicaltrials.gov (NCT03384732).
Participants
Inclusion criteria were: at least 75 years of age; and living independently in the community. In Germany, nursing care needs are determined based on 5 care-grades, depending on physical, mental and psychological disabilities, ranging from care-grade 1 (little impairment of independence) to care-grade 5 (hardship cases) (24). Only persons with no care-grade or care-grade 1 were included in this study, as persons with higher grades were expected to be too impaired to live independently.
Recruitment and sample size
Convenience sampling was applied. Participants were recruited by primary care practices in Franconia, which were part of the PRO PRICARE research network. In addition, study participants were recruited by city departments and different senior clubs in the region of Erlangen/Nürnberg (Germany). Persons who indicated their interest in the study, were contacted via telephone to collect data on sociodemographic and health-related variables to ensure eligibility. Oral and written information about the study was provided by the researchers.
Ethical considerations
The study was approved by the Ethics Committee of the Faculty of Medicine of the Friedrich-Alexander-University Erlangen-Nürnberg (Re.-No.: 90_17 B). The participants were informed that they could end the interview if desired, and that their confidentiality would be assured. All participants provided written informed consent. Furthermore, no quotations in this paper can be traced back to the participants.
Data collection
In a first step, participants received a digital camera to take photographs of their daily life. These photographs served as a basis for the in-depth semi-structured interviews. To explore and understand which aspects of functioning are important to older adults a semi-structured interview guide was developed (Appendix SI1). Information that cannot be captured by audio recording was documented in a pre-structured interview record immediately after the interview (Appendix SII1). The interviews were conducted by 3 researchers (JT, SG, SB) at the homes of the study participants between June 2017 and January 2018. If couples who were living together participated in the study, only one interview was conducted with both of them. In addition, the participants were invited to participate in focus groups to stimulate discussion between them and produce further relevant concepts (25). To increase comparability among the focus groups, a focus group script was developed and used in all focus groups (Appendix SIII1). Similar to the interviews, pictures showing everyday activities were presented and discussed. Immediately after the focus group, the researcher completed a focus group record (Appendix SIV1). The focus groups were conducted by 2 researchers (JT, SG) at the Institute of General Practice (Erlangen) and the Institute for Biomedicine of Aging (Nürnberg) in March and April 2018. All interviews and focus groups were audio recorded. Each study participant received €75 as a representation allowance.
Data analysis
For the purpose of analysis, the audio records were transcribed verbatim. The original wording (e.g. short-cut articulation, dialect) and grammatical structure were retained; non-verbal aspects (e.g. laughter, low voice, pauses) were documented; utterances and decorating words were left out. Following the methodology proposed by the ICF Research Branch, the analysis process consisted of a qualitative analysis and a linking procedure to the ICF (18). Three researchers (JT, SG, AH), who had received training to become familiar with the structure and the content of the ICF as well as the linking rules, were involved in the analysis process.
Qualitative analysis
The transcripts were analysed based on Mayring’s qualitative content analysis, more precisely the structuring technique with nominal deductive category assignment, using the ICF as a category system (26). All text passages relevant for answering the research question were retrieved from the transcripts. These text passages could consist of one word or several sentences and were not defined by grammatical rules, but by a shift in meaning (27). Relevant concepts (i.e. themes) were assigned to these text passages and linked to an ICF category.
Linking to the ICF
The identified concepts were linked to the most precise ICF category following established linking rules (28). One concept could be assigned to one or more ICF categories. ICF categories are coded using an alphanumeric coding system. Each code consists of the letter of the respective component (“Body Functions” (b), “Body Structures” (s), “Activities and Participation” (d), “Environmental Factors” (e)), followed by the chapter number (1 digit), the second level (2 digits), and the third and fourth levels (1 digit each) (16). Concepts that did not belong to the universe of the ICF (e.g. health conditions) were coded as “not covered” (“nc”, e.g. nc-hc for health conditions). Concepts that could be assigned to an ICF component, but not to a more precise category (e.g. general health) were coded as “not defined” (“nd”, e.g. nd-gh for general health) (28). If a concept referred to a personal factor (e.g. attitudes or coping strategies) it was assigned a “pf”, as personal factors are not yet classified in the ICF. The ICF categories are presented at the second level in this paper. If a concept was linked to a third- or fourth-level category, the corresponding second-level category is reported. Descriptive statistics were used to report the most frequently identified ICF categories.
Quality assurance
Following the methodology of other qualitative studies in the ICF Core Set development process, 2 strategies were applied to ensure accuracy of data analysis: multiple coding and peer review (29–31). To enhance agreement between the researchers concerning the analysis process and the linking rules, the first interview was analysed and linked to the ICF by all 3 researchers independently (multiple coding). The remaining transcripts were analysed and linked to the ICF by just one researcher. Random samples of each transcript (on average 20% of the transcribed text) were analysed and linked to the ICF by a second researcher (peer review). The degree of agreement between the 2 researchers regarding the linked second-level ICF categories was calculated using Cohen’s kappa. The kappa analysis was performed using IBM SPPS Statistics 21 (IBM Corp, Armonk, NY).
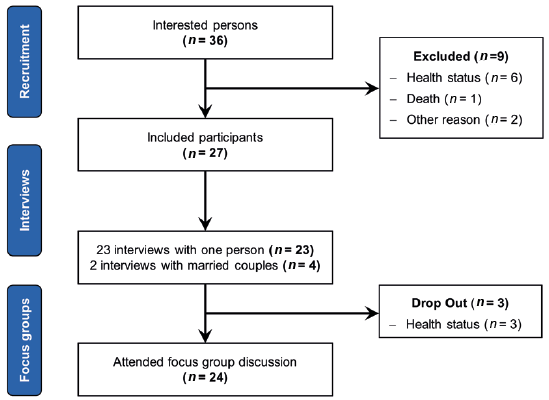
Twenty-seven people participated in this study (Fig. 1). Participants were all community-dwelling older adults, mean age 80.8 years (standard deviation (SD) 4.8; range 75–95 years). The proportion of women in the sample was 77.8%. One-third of participants lived alone and two-thirds lived in urban areas. More than one-third of the participants (37.0%) had a higher education. Participants’ characteristics are summarized in Table I. The interviews lasted on mean 67 min (range 36–140 min). In addition, 4 focus groups were conducted, lasting on mean 115 min (range 100–130 min).
Fig. 1. Recruitment flow chart.
Table I. Sample characteristics
Linking results
From the transcripts a total of 6,667 concepts were extracted. Out of these, 20 concepts were linked to first-level categories, 6,268 to second-level categories and 9 multidimensional concepts to 2 or more ICF categories. Another 370 concepts could not be assigned to a specific ICF category. The 6,268 concepts were linked to 189 different second-level ICF categories. All 30 chapters of the ICF were covered. The ICF categories “recreation and leisure (d920)”, “changing basic body position (d410)”, and “immediate family (e310)” were named in all 25 interviews. In all but one interview the ICF categories “family relationships (d760)”, “informal social relationships (d750)”, “doing housework (d640)”, “preparing meals (d630)”, and “products and technology for personal indoor and outdoor mobility and transportation (e120)” were mentioned. The 3 most frequently identified second-level categories of the respective ICF components, according to the counted frequency and number of interviews in which the category was mentioned, are described below. The 10 most frequently identified categories of each component are shown in Table II; all identified ICF categories are shown in Appendix SV1.
Table II. Top 10 categories of the components Activities and Participation (d), Environmental Factors (e), Body Functions (b) and Body Structures (s)
Second-level categories
Within the Activities and Participation component, the categories “recreation and leisure (d920)”, “changing basic body position (d410)”, and “family relationships (d760)” were the most important topics for the participants. The following quotes exemplarily illustrate concepts that were linked to one or more of these categories. The excerpts below were originally in German and have been translated into English for this paper by JT, for illustrative purposes only.
I can go play some card games or I can go to the coffee party or I can (.) go for a meal every (.) week or fourteen days with another group of people. (male, 79 years)
Regarding the ICF component Environmental Factors, the ICF categories “immediate family (e310)”, “products and technology for personal indoor and outdoor mobility and transportation (e120)”, and “products or substances for personal consumption (e110)” were identified most often:
When we were in town this Sunday, all grandchildren were there. I have three grandchildren (.) and they guided me and took my shoes off. They dressed me and I said to myself ‘that was touching’. (female, 88 years)
From the component Body Functions the ICF categories “emotional functions (b152)”, “higher-level cognitive functions (b164)”, and “sleep functions (b134)” emerged as the most relevant topics for the participants. The most frequently extracted ICF categories for Body Structures were” structure of lower extremity (s750)”, “structure of trunk (s760)”, and “structure of cardiovascular system (s410)”.
I should have had the right leg (.) right knee (.) operated (.) and I’m so afraid of that (.) I do not dare anymore. (female, 76 years)
First-level categories and code combinations
The assigned first-level categories were: “support and relationships (e3)”, “mental functions (b1)”, “communication (d3)”, “self-care (d5)”, “attitudes (e4)” and “structures related to movement (s7)”. Except for the first category, which was identified 15 times in 9 interviews, all of them were identified just once in one interview. Nine extracted concepts were not linkable to only one ICF category. For these concepts, 2 or more categories were chosen for each concept. These concepts referred to “fear of falling (b755, b2402, b152)” and “fatigue (b7402, b1300)”.
Personal factors, health conditions and not definable concepts
Out of the 370 concepts, which could not be assigned to a specific ICF category, 283 (76.5%) concepts were linked to the ICF component Personal Factors, which is not yet further specified in categories. The following 3 areas could be distinguished: “pf-coping” (n = 124), “pf-attitudes” (n = 63) and “pf-general” (n = 96). Concepts that focused mainly on how to cope with limitations in daily living were coded “pf-coping”. Overall, accepting and adapting were considered helpful strategies. In almost all interviews such strategies were reported.
Well, when I go up the stairs, I have to stop a few times. But I say to myself ‘I have time for that’. (female, 85 years)
From several interviews concepts were extracted that represent the mind-set of the participants (“pf-attitudes”). They mostly referred to attitudes regarding the ageing process and death.
Well, you also have to be happy with your life and – and you have to have a bit of (.) humility (.) and (.) have to accept it (.) and if I just have the attitude ‘I do not want to go to a retirement home (.) I do not want to go there’ (.) if you have this attitude then you will be disappointed once you really get there. (female, 77 years)
Concepts assigned to “pf-general” referred to independent living, satisfaction, living arrangements, (former) occupation, family status, and family’s origin. Out of the remaining concepts, which could not be assigned to a specific ICF category, 53 (14.3%) were health conditions (nc-hc) and 34 (9.2%) were characterized as “not definable (nd)”. The most commonly mentioned health conditions were musculoskeletal disorders and cancer. The “nd” concepts mainly included general health and physical activity.
Accuracy of the analysis
Kappa coefficients were respectively κ = 0.94 for SG and AH; κ = 0.93 for SG and JT and κ = 0.88 for JT and AH. These results can be interpreted as a strong level of agreement (32).
Focus groups
A total of 10 additional ICF categories were extracted from the transcripts of the focus groups (see Table III). These mainly referred to the component Activities and Participation, followed by Environmental Factors and Body Functions. Only one additional category was identified in the component Body Structures. The most frequently identified category was “individual attitudes of strangers (e445)”.
Table III. Additional categories identified in the focus groups
With this qualitative study, aspects of functioning were identified from the perspective of community-dwelling older adults using the ICF as a framework. From their perspective, the component Activities and Participation has shown to be the most relevant one, with the categories “recreation and leisure” and “family relationships” being mentioned most often. It was followed by the components Environmental Factors (mainly the category “immediate family”) and Body Functions (mainly the category “emotional functions”). Only few categories within the component Body Structures were considered relevant. Categories were identified for all 4 ICF components and all 30 chapters, demonstrating the complexity and multidimensionality of the ageing process.
“Recreation and leisure (d920)” was the most relevant ICF category from the patient perspective. Different kinds of activities (e.g. social, productive, or physical activities) have been proven to be positively related to wellbeing, health, functioning, and survival (33, 34). They might influence health and wellbeing through different pathways, e.g. by providing a sense of purpose, through mental or physical demands, or by reducing the risk of social isolation (33). “Mobility (d4)” played a major role for the participants. This is in accordance with the findings from our empirical study, which is also part of the ICF Core Set development process (35). Mobility is central to healthy ageing and independent living (10, 36). Immobile persons are more prone to adverse health outcomes due to fewer opportunities for social contacts, reduced access to grocery stores (leading to fewer nutritional options) and to healthcare services (37, 38).
Environmental factors were of major relevance for the current participants. The most frequently identified category was “immediate family (e310)”. Social support, especially from the family, not only has a major influence on several health outcomes, but is also a major prerequisite for independent living despite functional limitations (39). Surprisingly, the category “products and technology for communication (e125)”, which includes, among others, hearing aids or glasses, was not frequently mentioned, although hearing loss and vision impairment are common problems in older adults and, when not treated, are negatively associated with activities and participation (40).
Within the Body Functions component, most concepts were assigned to categories of the chapter “mental functions (b1)”. These functions are closely related to the execution of Basic Activities of Daily Livings (BADLs) and Instrumental Activities of Daily Livings (IADLs) and are consequently prerequisites for being able to live independently at home (39). Our participants rarely mentioned anatomical changes, as represented by the component Body Structures. The only categories that were mentioned somewhat frequently were assigned to the chapter “structures related to movement (s7)”. Here, again, the relevance of mobility becomes obvious.
Statements linked to personal factors referred mostly to coping strategies. These strategies are considered an important aspect of successful ageing and can have a positive impact on life satisfaction (41). Consequently, assessing, understanding, and improving coping skills might be a crucial aspect for improving functioning in old age and demonstrates the necessity of classifying personal factors within the ICF.
The emphasis of the component Activities and Participation might partly be explained by the fact that the interview was guided by the pictures taken by the participants. It might be easier to take pictures of activities than of other components of the ICF. However, the interview guide included questions aiming to elicit information about potential impairments in body functions or structures, which might underlie activity limitations or participation restrictions. It further included questions that addressed environmental and personal factors. We thus assume that not the impairments in body functions/structures per se are relevant, but the consequences they have for daily life.
The literature review, which is also part of the ICF Core Set development process, found that similar to the results of this qualitative study, the focus of frequently used assessment instruments for functioning is mostly on Activities and Participation1. Also, Body Functions played a major role, which were less frequently addressed in this qualitative study. In contrast, Environmental Factors, which seem to be of major relevance to our participants, were rather poorly addressed in the included assessment instruments. These findings suggest that the research and the patient perspective differ from each other in this regard and that those instruments that are frequently used within the scientific literature do not necessarily capture what is relevant to geriatric patients themselves.
1Tomandl J, Heinmueller S, Graessel E, Freiberger E, Kuehlein T, Hueber S, et al. Laying the foundation for a Core Set of the International Classification of Functioning, Disability and Health for community-dwelling elder adults in primary care: relevant categories of their functioning from the research perspective. A scoping review. (Unpublished observations).
Comparing our results with the already existing Core Sets mentioned in the introduction might be premature, as this is only 1 of 4 preparatory studies. However, it might be interesting to see what might be missing in the existing Core Sets from the perspective of the target group. We can see that, within the Core Set for geriatric patients in early post-acute rehabilitation facilities (22) and also the geriatric Core Set (19) almost half of all categories were selected from the component Body Functions, which was less relevant to our participants. In the ICF Primary Care set for patients with chronic conditions (20), most ICF categories belong to the components Activities and Participation, followed by Body Functions. Similar to our results the component Body Structures was the least relevant one in all of the other Core Sets, with no categories at all being included in the geriatric Core Set and the Primary Care set. There seem to be some differences between our preliminary Core Set from the perspective of the target population and the already existing Core Sets, especially the one for geriatric patients in early post-acute rehabilitation facilities and the geriatric ICF Core Set. We assume that there might be a need to adapt these existing Core Sets according to the patients’ needs.
Strengths and limitations
To our knowledge this is the first qualitative study examining functioning from the perspective of community-dwelling elderly adults using the ICF as a framework. A diverse range of participants was included, regarding socio-demographic variables, resulting in a broad range of different opinions. By asking the participants to take photographs of their activities and limitations as a basis for the interviews they had to think about these limitations, which facilitated talking about them in the interviews. Furthermore, the combination of interviews and focus groups enabled us to gather rich and meaningful data. In order to improve trustworthiness of the results 2 techniques for quality assurance have been used: multiple coding and peer review. The findings of this study have to be seen in light of some limitations. Our participants were not very limited in their independence, which might be due to our sampling technique. In addition, the study was conducted in Germany in areas with good healthcare and environmental structures. Thus, it cannot be concluded that the relevant areas presented and discussed in this paper are equally relevant to other elderly adults having more functional limitations, living in more deprived areas of Germany or in other countries. To address this limitation, future research including more participants from different areas is recommended. It is further important to notice that the primary objective of this study was to explore aspects of functioning that are important to older adults, using the ICF as a framework. In general, a broad range of concepts could be linked to the ICF. However, some experiences cannot be reproduced by linking them to an ICF code, but can be understood only when taking into account the interrelation between activities and contextual factors. As mentioned in another ICF Core Set development study, further in-depth qualitative content analysis would be required to achieve greater understanding of these experiences (29).
Implications for practice
From the results of this qualitative study we might conclude that those aspects of functioning that are relevant to older patients (i.e. Activities and Participation as well as Environmental Factors) are not necessarily captured by general practitioners. Thus, in order to improve functioning in this population, it might be warranted to include more biopsychosocial information in the consultation. This qualitative study provides a list of relevant ICF categories that will be used together with the results of the other 3 preparatory studies for developing the ICF Core Set for older primary care patients. In the long-term, this ICF Core Set is expected to support general practitioners in assessing functioning of their patients, defining treatment goals that are less deficit-oriented, and based on these goals, differentiating between necessary and unnecessary medical interventions.
In conclusion, this qualitative study demonstrates the complexity and multidimensionality of the ageing process, using the ICF as a framework. Despite some limitations experienced in the linking process, the ICF provides a useful reference to identify and cluster the concepts that emerged from the interviews.
The authors would like to thank all study participants. We would further like to thank the “Forschungspraxen Franken”, as well as our project assistant Karin Ertl and our student assistants, Carmen Friedrich and Raphaela Wallner, for their excellent support during the recruitment phase. Finally, we would like to thank our student assistants for transcribing the interviews and focus groups: Dominik Edel, Victoria Fey, Carmen Friedrich, Miriam Heß, Annalena Lang, Antonia Meyer, Raphaela Wallner and Lukas Worm.
The present work was performed in partial fulfilment of the requirements for Johanna Tomandl obtaining the degree “Dr. rer. biol. hum.”.
Funding. This work was supported by the German Federal Ministry of Education and Research grant number 01GY1605. The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Data availability statement. Due to the nature of the data (audio recordings and transcripts), we are not able to share the raw data. Only the de-identified transcripts used and analysed during the current study are available from the corresponding author upon reasonable request.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize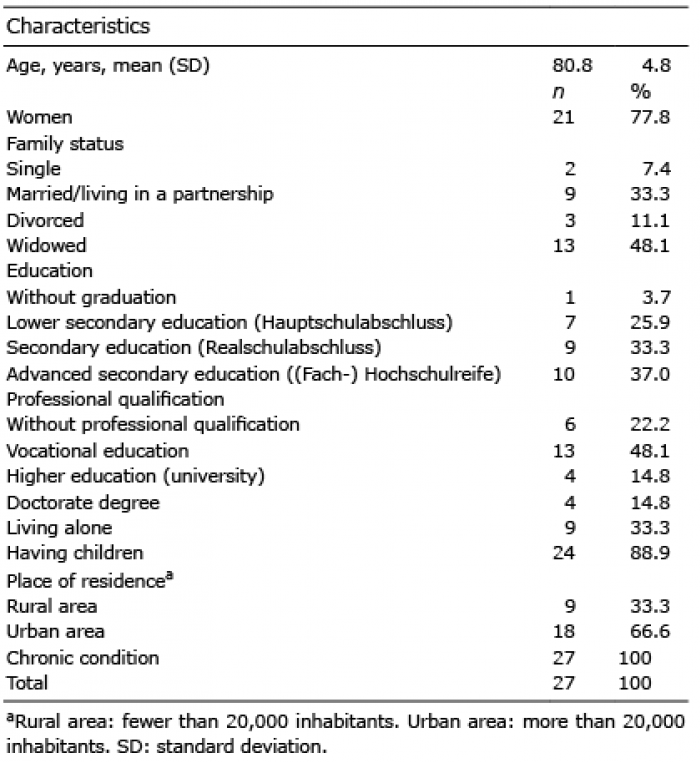 Click to show fullsize
Click to show fullsize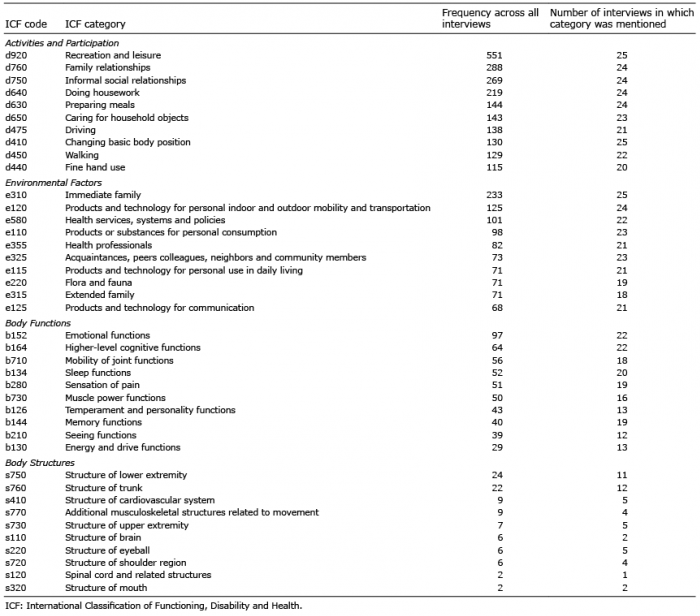 Click to show fullsize
Click to show fullsize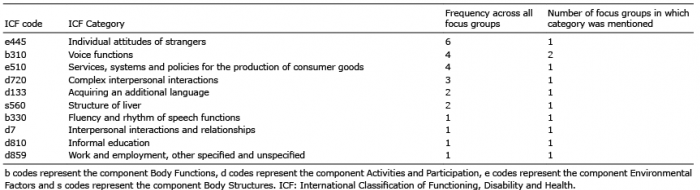 Click to show fullsize
Click to show fullsize