
From the 1Institute of Neuroscience and Physiology, Section of Health and Rehabilitation, Physiotherapy, Sahlgrenska Academy, University of Gothenburg, Gothenburg, 2Region Västra Götaland, Research and Development Primary Health Care, 3Region Västra Götaland, Primary Care Rehabilitation, Närhälsan and 4Department of Rheumatology and Inflammation Research, Institute of Medicine, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Objective: To determine the effectiveness of a person-centred intervention, including advice on physical activity, for improving pain intensity, physical activity, and other health-related outcomes in persons with chronic widespread pain , when delivered with digital eHealth support compared with standard telephone follow-up.
Design: Randomized controlled trial.
Subjects: Individuals with chronic widespread pain (n = 139), aged 20–65 years, who had previously participated in a pain educational programme at primary healthcare units, were contacted during the period 2018–19 and randomized to an intervention group (n = 69) or an active control group (n = 70).
Methods: Together with a physiotherapist, participants in both groups developed person-centred health plans for physical activity. The intervention group was supported via a digital platform for 6 months. The active control group received support via one follow-up phone call. Primary outcome was pain intensity. Secondary outcomes were physical activity and other health-related outcomes.
Results: No significant differences were found between the groups after 6 months, except for a significant decrease in global fatigue in the active control group compared with the intervention group. Conclusion: Future development of interventions supporting persons with chronic pain to maintain regular exercise is warranted.
Key words: physiotherapy; chronic pain; eHealth; person-centred; randomized controlled trial; physical activity.
Accepted Jan 18, 2021; Epub ahead of print Feb 12, 2021
J Rehabil Med 2021; 53: jrm00175
Correspondence address: Sofia Juhlin, Närhälsan Uddevalla Rehabmottagning Bävebäcksgatan 5, 451 50 Uddevalla, Sweden. E-mail: sofia.juhlin@vgregion.se
Doi: 10.2340/16501977-2796
Despite documented positive effects of physical activity in treating persons with chronic widespread pain, it is challenging for many individuals with chronic widespread pain to independently continue to be physically active over time. This study measured the effects of a person-centred health plan to promote physical activity, delivered using eHealth support compared with standard follow-up by telephone, in persons with chronic widespread pain. Participants with chronic widespread pain (n = 139) were randomized into 2 groups: an intervention group, in which participants created an individual health plan together with a physiotherapist and were provided with digital eHealth support for 6 months; and an active control group, who also created an individual health plan together with a physiotherapist, and received one follow-up support phone call. The results showed no significant difference between the groups regarding change in the primary outcome, pain intensity. The active control group showed a significant decrease in global fatigue compared with the intervention group. Future development of interventions supporting persons with chronic pain to maintain regular exercise is warranted.
Approximately 7–13% of the population of the Western world have chronic widespread pain (CWP) (1–3). CWP is defined as pain in both sides of the body, above and below the waist, and axial pain for at least 3 months (4); it is also characterized by symptoms such as increased tenderness, fatigue, reduced physical capacity and general health, and psychological distress (2, 5).
Physical activity is the first-choice treatment for patients with chronic pain conditions, such as CWP and fibromyalgia (FM), as it has been shown to have positive effects on pain and other symptoms (6, 7). Although several clinical trials have shown that persons with CWP can gain positive health effects from regular, individually adjusted physical activity (7–9), it is challenging for many individuals with CWP to continue to be independently physically active over time, and the improvements gained are often lost. A person-centred approach, in which physical activity is adjusted to the individual’s resources, can enable persons with CWP to become regularly physically active (10, 11). Persons with CWP often experience increased pain during and after physical and psychological loading, which could be related to dysfunction in endogenous pain inhibition (12, 13).
The use of eHealth interventions in healthcare is increasing rapidly (14). eHealth has been defined as “health services and information delivered or enhanced through the internet and related technologies” (15). eHealth interventions used to manage chronic pain in previous research have been based on providing information about pain, or used for communication between healthcare providers and patients, as an alternative to scheduled healthcare appointments (16). Studies on eHealth interventions in persons with chronic pain have found contradictory results, which may be due to differences in the type of eHealth interventions used. A systematic review of studies of persons with pain found promising evidence that internet-based peer-support programmes can lead to improvements in pain intensity, activity limitations, health distress, and self-efficacy (17). Another study found that persons with FM who received internet-delivered exposure treatment improved in symptoms and overall health status compared with a control group (18). However, a study of persons with CWP found no significant long-term improvements in terms of catastrophizing, daily functioning, symptom levels, acceptance of pain, or emotional distress, when using a smartphone-based intervention comprising diaries and therapist feedback (19).
Overall, there is a lack of studies on eHealth interventions in persons with CWP, and specifically, on eHealth as support for physical activity. Although eHealth support to manage chronic pain seems to show encouraging results (16), it is unknown which patients benefit the most (17) or which eHealth techniques are effective.
The aim was to determine the effectiveness of a person-centred intervention, including advice on physical activity, for improving pain intensity, physical activity, and other health-related outcomes in persons with CWP, when delivered with digital eHealth support compared with standard telephone follow-up.
Design
The study was a single-blinded multicentre randomized controlled trial (RCT). (ClinicalTrials.gov Identifier: NCT03434899).
Participants
Inclusion criteria were: persons with CWP, aged 20–65 years. The definition of CWP used was pain in both sides of the body, pain above and below the waist, and axial pain for at least 3 months (4). Presence of CWP was determined by the duration and localizations of pain reported by the participant during phone screening.
Exclusion criteria were: other severe somatic or psychiatric disorders, dominating causes of pain other than CWP, or other severe disease interfering with the ability to be physically active, pregnancy, not having access to a smartphone or a computer, inability to speak or understand Swedish, ongoing physiotherapy treatment, and already exercising regularly.
Recruitment
A total of 701 persons with CWP, who had participated in a pain management programme during the period 2010–16 at 5 primary healthcare rehabilitation centres in 5 cities or towns in the western part of Sweden, were invited to join the study between March 2018 and April 2019 via letter providing written information about the study. The letter was followed by a phone call 1–2 weeks later to screen for inclusion and exclusion criteria and interest in participating. Subject who could not be reached by phone were sent a second letter in which they were asked to contact the study coordinator if they were interested in participating.
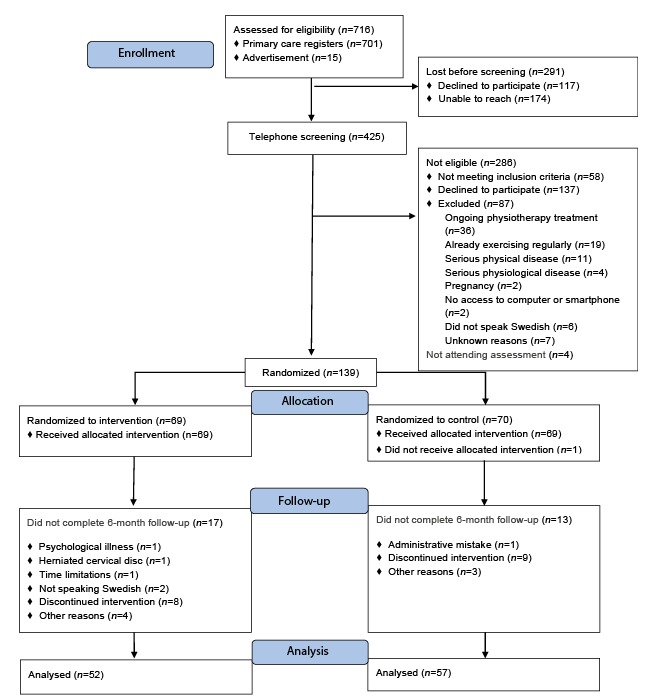
Of the total of 701 persons, 117 declined to participate in the study and 174 people could not be reached by phone or letter. After an advertisement in a local newspaper in 1 of the 5 cities, an additional 15 people contacted the study coordinator and were screened by phone. In total, 425 people were screened by phone by physiotherapists at the healthcare rehabilitation centres. During the phone screening, 137 people declined to participate when informed about the study, 58 were omitted as they did not fulfil the inclusion criteria, and 87 were excluded based on the exclusion criteria. Four people did not attend for baseline examination, for unknown reasons. A final total of 139 persons with CWP were included in the study and randomized (Fig. 1).
Fig. 1. Consolidated Standards of Reporting Trials (CONSORT) flow diagram of progress of the 2 groups in the randomized controlled study.
Baseline and follow-up examinations
Examinations were conducted at baseline and after 6 months by blinded examiners at the primary healthcare centres. The examinations included a battery of questionnaires and a test of physical function. Outcome assessment measures were the same in both groups of randomization.
Randomization
Randomization was performed after baseline examination, using block randomization, in blocks of 6, separately for each site, with sealed, opaque, sequentially numbered envelopes prepared by a statistician. Randomization was performed by a person who was not involved in the examination or intervention. A total of 69 participants were randomized to the intervention group and 70 to the active control group.
Measures
Demographic data. Data on age, pain duration, pain localization, pharmacological treatment, tobacco use, country of birth, level of education, family status, economic status, work status, sick-leave, and disability pension were collected via a questionnaire.
Primary outcome measurement. Pain intensity during the previous week was assessed with a 0–100 subscale from the Fibromyalgia Impact Questionnaire (FIQ) (20); FIQ-pain. A lower score indicates less pain. FIQ-pain is sensitive to change in pain intensity in persons with CWP (8), and the minimal clinical important difference (MCID) for FIQ-pain has been suggested to be 15% in clinical trials (21).
Secondary outcome measurements. FIQ-total (0–100) assesses overall health status with 10 subscales. A lower score indicates better health. FIQ-total and the subscale FIQ-fatigue, assesses global fatigue, were used as secondary outcomes in the present study (22). FIQ-total has shown satisfactory test-retest reliability and validity among persons with FM (20).
The Multidimensional Fatigue Inventory (MFI-20) (4–20), includes 20 statements rated 1–5 on a Likert scale. The questionnaire has 5 subscales: general fatigue, physical fatigue, mental fatigue, reduced motivation, and reduced activity. A higher score indicates a higher degree of fatigue. MFI-20 has shown satisfactory construct validity and test-retest reliability in FM (23).
The Stress and Crisis Inventory (SCI-93) (0–140), assessing clinical manifestations of stress, comprises 35 items rated 0–4 on a Likert scale. A higher score indicates a higher level of stress. SCI-93 has shown satisfactory validity and test-retest reliability in persons with FM and CWP (24).
The General Self-Efficacy Scale (GSES) (10–40) comprises 10 items, rated 1–4 on a Likert scale. A higher score indicates higher self-efficacy. The Swedish version of GSES has been validated in different cohorts (25).
The Short Form 36 (SF-36) (0–100), assessing health-related quality of life, gives 2 composite scores: the Physical Component Summary (PCS) and the Mental Component Summary (MCS). The PCS was included as outcome in the present study. A higher score indicates better quality of life (26).
The Leisure Time Physical Activity Instrument (LTPAI) assesses leisure-time physical activity during a typical week The LTPAI has shown satisfactory test-retest reliability and validity among persons with FM (27).
Physical function was assessed with the 1-min chair-stand test. The participant was instructed to stand up and sit down on the chair as rapidly as possible, and as many times as possible during 1 min. The test has acceptable inter-rater reliability in FM (28).
Intervention
The intervention was created by physiotherapists, scientists, together with a patient research partner with chronic pain from the Swedish Rheumatoid Association. The theoretical framework was based on the theories of person-centred care (PCC) and self-efficacy. PCC is an ethical approach, the basis of which is to understand the person behind the patient and to include their knowledge, resources, and barriers in planning the rehabilitation (29). Actively involving the patient in treatment is thought to enhance the patient’s ability to manage health problems and to strengthen their confidence and resources (29). Using person-centred principles is suggested to enhance self-efficacy (30). Self-efficacy refers to one’s belief in one’s ability to succeed in accomplishing a task (30) and is promoted by mastering tasks, role models, feed-back and one’s earlier emotional and physical experiences of the intended task (30).
The two groups underwent the same first individual meeting with a physiotherapist to create a health plan with physical activities. The difference between the groups was the type of support, where the intervention group had one follow-up meeting and thereafter were supported through a digital e-health platform for 6 months, and the active control group had no follow-up meeting and were supported only by one follow-up phone call.
The physiotherapists who performed the interventions had clinical experience of person-centred physiotherapy for patients with CWP. The minimum requirement of experience for the physiotherapist was 2 years of working with patients with CWP. Due to the nature of the intervention it was not possible to blind the participants or the physiotherapist to group allocation.
Intervention group
The intervention comprised 2 individual meetings with a physiotherapist at a primary healthcare centre.
At the first meeting the physiotherapist and participant created a health plan with physical activities, and if needed, stress management, based on each participant’s individual preferences, obstacles, goals, and resources, according to a person-centred model used in earlier studies (29, 31). The physical activity had individual health promotional goals aiming towards the World Health Organization’s (WHO’s) recommended level of physical activity; to be physically active at a moderate intensity for 150 min per week or, at a high intensity, for 75 min per week (32).
One week after the first meeting, a second individual meeting was held. At this meeting the physiotherapist initiated a discussion about the health plan and asked to what extent it had been followed by the participant. The health plan was adjusted if the participant felt the need for it. The digital platform was uploaded on the participant’s smartphone or computer and they were instructed in its use.
During the 6-month study period, communication between the physiotherapist and participant was managed through the digital platform pursuant to each participant’s individual needs. Participants could contact the physiotherapist if needed, and were encouraged to access the platform once a week to answer questions regarding their health, and the extent to which they had been able to manage their health plan during the previous week. Participant’s use of the digital platform was estimated by the number of times they accessed the platform to answer the questions, based on 3 categories (“1–3 times”, “3–10 times” and “more than 10 times”) and by the number of times they accessed the platform to contact the physiotherapist. Seven participants in the intervention group had telephone contact a few times during the 6 month study period, after they expressed a need for this through the digital platform.
The generic digital platform (33) was developed according to a participatory design (34), which involved researchers from the Centre for Person-Centred Care at the University of Gothenburg (GPCC) and potential end-users, such as patient representatives and healthcare professionals. On the platform, the participant could both send and receive messages from the healthcare professionals in order to promote interaction. The co-created health plan was uploaded to the digital platform.
Active control group
Participants in the active control group had one individual meeting with a physiotherapist at a primary healthcare centre. During the meeting the physiotherapist and the participant created a health plan with physical activities adjusted to the person’s symptom severity, and if needed, stress management, based on each participant’s individual preferences, obstacles, goals and resources, according to person-centred principles (29, 31). The goal for physical activity was individual, aiming for WHO’s recommended level of physical activity, as described above (32). The meeting was followed-up by a phone call from the same physiotherapist one month after the initial meeting. During this phone call the health plan was followed-up briefly and adjusted if the participant felt the need for it. After the phone call the participants in the active control group had no further contact with the physiotherapist.
Ethics
The study was reviewed and approved by the Regional Ethical Review Board in Gothenburg, University of Gothenburg (number 1025-17). All participants received written and oral information about the study and provided written consent to participate.
Statistical analyses
Sample size determination was made prospectively, based on previous research (8). The baseline value of the FIQ-Pain scale was 68.8 units. A total of 60 participants was needed in each group in order to detect a clinically meaningful difference (being 15% (21) and corresponding to a 10 units difference between the groups, with an estimated standard deviation (SD) of 19, 80% power, and 5% significance level) using a 2-sided Mann-Whitney U test. To allow for dropouts, the study aimed to recruit 70 participants per group.
The analyses in the present study were made according to intention-to-treat, implying that participants were analysed according to allocation group, regardless of how well they had followed the intervention. However, only measured values were included in analyses of changes over time between the 2 groups, implying that missing cases were not included in the analysis.
Descriptive statistics are shown as means and SD for continuous data and as numbers (n) and percentages (%) for categorical and dichotomous data (Table I). Primary and secondary outcomes at baseline and follow-up are shown as means and SD, and the differences from baseline to the 6-month follow-up are shown as means, SD, and 95% confidence intervals (95% CI) (Table II).
Between-group differences for changes in outcomes from baseline to 6-month follow-up were calculated using Mann–Whitney U test for continuous data, and Pearson’s χ2 or Fisher’s exact test for categorical data. Significance level was set at 5% with no adjustment for multiple comparisons.
Descriptive statistics
Descriptive baseline data for the intervention group and the active control group are shown in Table I. A total of 109 subjects (79%) participated in the 6-month follow-up; 52 (75%) subjects in the intervention group and 57 (83%) in the control group (Fig. 1). For more details see the “Loss to follow-up” section, below.
Six health plans were found to be missing. The content of the 133 available health plans developed at baseline revealed that 74 participants (56%) of 133 had developed goals for physical activity that were in line with, or higher than, the WHO’s recommended level of physical activity. Ninety-one (68%) of 133 participants included strength training in their health plans.
Table I. Baseline data for the intervention and active control groups. Mean and standard deviation (SD) for continuous variables, and number and percentage (%) for categorical variables
Activity on the digital platform
In the intervention group, activity on the digital platform varied between participants. Of the 69 participants in the intervention group, 60 (87%) used the platform. Participants answered the questions regarding their health and to what extent they had followed the health plan, to various degrees: 36% (n = 25) answered the questions “1–3 times”, 20% (n = 14) answered “3–10 times” and 30% (n = 21) answered “more than 10 times”. The remaining 9 participants (13%) never used the digital platform after the introduction.
Of the 60 participants who used the platform, 21 (35%) contacted the physiotherapist a total of 126 times, mean 6.0 (range 1–20) times. Ninety-four contacts (75%) concerned seeking advice for health problems, increased pain, adjustment of the health plan, or practical matters regarding the study. Thirty-two (25%) of the contacts concerned problems with the digital platform. Twenty participants (33%) were contacted by the physiotherapist a total of 69 times, mean 3.5 (range 1–10) times. In 66 (96%) of these contacts the patient answered questions from the physiotherapist regarding the health plan and physical activity. In 3 contacts (4%) the physiotherapist contacted the participants concerning the platform. Nineteen participants (32%) never had any contact with the physiotherapist through the platform, nor did they answer questions asked by the physiotherapist via the platform. There was a significant difference from baseline to 6-month follow-up between the participants who used the platform (n = 50) compared with those who did not use the platform (n = 7) with regard to change in FIQ-pain (p = 0.025, mean change 3.8 mm (SD 19.66) vs –20.5 mm (SD 6.36)). There was no significant difference regarding change in LTPAI between users and non-users of the platform.
Primary outcome
Between-group comparisons. There were no significant differences between the intervention and active control groups regarding change in pain intensity assessed with FIQ-pain from baseline to 6-month follow-up (Table II).
Table II. Mean and standard deviation (SD) for baseline values and differences (∆) with 95% confidence intervals (95% CI) from baseline to the 6-month follow-up, and p-values for between-group differences
Secondary outcomes
Between-group comparisons. There was a significant difference between the groups in change from baseline to 6-month follow-up regarding global fatigue assessed with FIQ-fatigue; the active control group improved significantly compared with the intervention group (p = 0.004). No significant differences were found between groups for change in any other outcomes (Table II).
Loss to follow-up
A total of 29 participants were lost to follow-up; 17 in the intervention group and 12 in the active control group. There were no significant differences between the participants in the 2 groups who were lost to follow-up regarding baseline data for pain localization, pain duration, work status, education level, economic status, FIQ-pain, FIQ-total, FIQ-fatigue, SCI-93, SF-36, GSES, FABQ, PDI, or the 1-min chair-stand test.
Significant differences were found in age (p = 0.010), LTPAI (p = 0.048) and MFI-20 mental fatigue (p = 0.021); those who were lost to follow-up in the intervention group were older, performed fewer hours of physical activity, and had lower mental fatigue at baseline, compared with those who were lost to follow-up in the active control group (age: baseline mean 54 years (SD 7) vs 44 years (SD 11), LTPAI: baseline mean 3.7 hours (SD 2.0) vs 8.5 hours (SD 6.5), MFI-20 mental fatigue: baseline mean 13.6 score (SD 4.4) vs 17.8 score (SD 2.4)).
This RCT investigated the effect of a person-centred intervention, comprising eHealth, to support individuals with CWP to remain physically active, in order to achieve lasting health improvements. The results showed no significant difference between the intervention group, supported by the digital platform and the active control group, supported by a follow-up phone call, regarding change in the primary outcome, pain intensity or most of the secondary outcomes. These results imply that digital support does not contribute to improvements in the outcomes measured. This is in line with a previous RCT of persons with chronic pain (35) showing that adding an internet-based programme to a multimodal rehabilitation (MMR) programme did not contribute to any improvements in health-related aspects (35).
The active control group showed a significant improvement in the secondary outcome, global fatigue, when compared with the intervention group. This is an intriguing finding; it may indicate that the health plan together with follow-up by phone resulted in this improvement. However, further studies are needed to investigate the best way to provide adequate support for persons with chronic pain to enable them to be physically active and maintain physical activity habits.
In the current study, the digital platform was applied both as a tool for interaction between the participant and the physiotherapist, and as a tool for the participants to monitor their health, which are suggested to be 2 main functions of eHealth (36). The participants in the current study were randomized to receive support via the digital platform, regardless of whether they expressed a need for the platform. Thirty-five percent of participants used the platform to contact the physiotherapist for advice when encountering obstacles, such as increased pain or other health problems, and 30% answered the weekly questions regularly. These proportions are in line with a previous study of a web-based programme, in which 36% of subjects used all modules provided in the programme (35). Activity on the digital platform seemed to be dependent on the participants’ individual needs, which is in line with recommendations that eHealth interventions should be individualized (14, 35). Participants who did not use the platform improved significantly more in pain intensity than those who used the platform; however this result should be interpreted with caution, since 1 of the comparison groups was small (n = 7). When implemented in clinical practice, the digital platform should be offered to patients who prefer this type of digital support, as this might affect both the amount of use and the effect of the digital platform.
The participants in both the intervention group and the active control group in this study created a health plan together with a physiotherapist. The first individual person-centred meeting was initiated with a question from the physiotherapist regarding the participant’s previous experiences of physical activity, followed by questions regarding the participant’s goals in creating a health plan including physical activity. The participant’s preferences, resources, fears, and barriers were discussed and the health plan was created in mutual understanding and partnership with the physiotherapist, who contributed professional knowledge. At present there is a lack of valid instruments to assess how well participants’ preferences are met; hence this was not measured. As person-centred interventions are complex there is no consensus about the components that lead to change (37).
In the current study, participants received a health plan based on their preferences. However, follow-up and progression of the health plan were limited, and the digital support was based on the participants’ own decisions to contact the physiotherapist. Further studies are therefore needed to determine whether frequent scheduled follow-ups might be desired by the participants to discuss possible progression of the health plan, and whether this would lead to other outcomes.
The study sample was similar to other populations with CWP in earlier exercise studies regarding age, symptom severity and work status (11, 38). The study hypothesis was that increased physical activity would contribute to improvement in pain intensity. A total of 74 participants had baseline goals in their health plan that were in line with, or higher than, WHO’s recommended level for physical activity. The self-reported total amount of physical activity appeared to increase in the intervention group, but not in the active control group. The mean increase in physical activity in the intervention group was 2 h per week, which might not be enough to have an impact on pain intensity. In addition, at baseline the intervention group had a lower level of physical activity than the active control group, which could have affected the ability of each group to increase the amount of physical activity during the study period.
Study strengths and limitations
A limitation of the current study is the lack of an objective measure of physical activity, since we do not know how many of the participants that reached their physical activity goals.
Another limitation concerns the digital support used in the intervention. Since there is a continuous development of digital tools, the results of this study are only applicable for the mode of digital support used in this study.
There have been few previous studies evaluating digital support for physical activity in persons with CWP. A strength of the current study is that it compares 2 clinically relevant methods for following a health plan of physical activities developed with person-centred guidance for persons with CWP, both of which are expected to have a low cost.
Clinical implications
The results of the current study show that the digital intervention programme promoting physical activity for persons with CWP was as effective as the control procedure with a follow-up telephone call, regarding pain intensity but less effective for global fatigue. We consider that individual preference should guide the type of support offered to persons with CWP, which is in line with person-centred principles.
A previous review indicates that eHealth has the potential to improve clinical practice and act as a complement to face-to-face care (14). It is possible that the type of digital platform used plays a role in the impact of the intervention (39); therefore, the results of the current study cannot be generalized to other digital platforms. Nevertheless, this study contributes valuable information on which to base further development of eHealth to support physical activity in persons with CWP.
Conclusion
When comparing the intervention group, supported by a digital platform, and the active control group, supported by a follow-up phone call, no significant difference was found regarding pain intensity. The active control group showed significant improvements in global fatigue when compared to the intervention group. Mechanisms of this improvement can, however, not be analysed in this study.
It is important to develop interventions or methods that support individuals to maintain physical activity over time, in order to achieve lasting improvements in health and physical function. Further development of interventions to support persons with CWP to maintain regular physical activity is needed.
This study was financed by grants from the Swedish state under an agreement between the Swedish government and the county councils, the ALF agreement (ALFGBG-722411). It was also financed by grants from The Healthcare Committee, Region Västra Götaland, and The Swedish Rheumatoid Association.
Charlotte Alfredsson, Elisabeth Enhörning, Ninni Eliasson, Eva-Lena Forssén, Urban Ryssnäs, Maria Ellsén, Anneli Lund, Marie-Louise Andersson, Eva Johansson, Sofia Johansson and Malin Johansson conducted examinations or interventions. The patient research partner from the Swedish Rheumatoid Association was Gert Persson.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize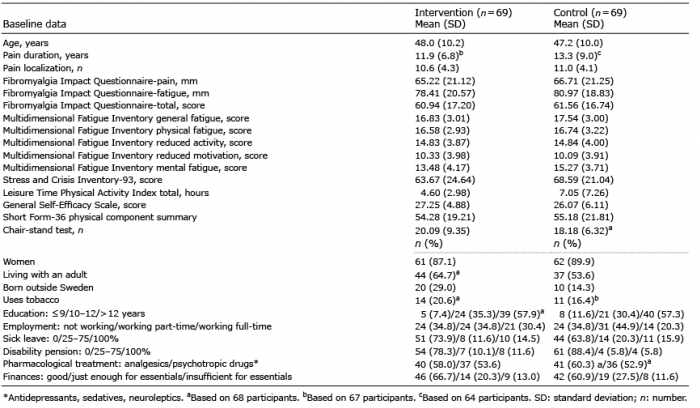 Click to show fullsize
Click to show fullsize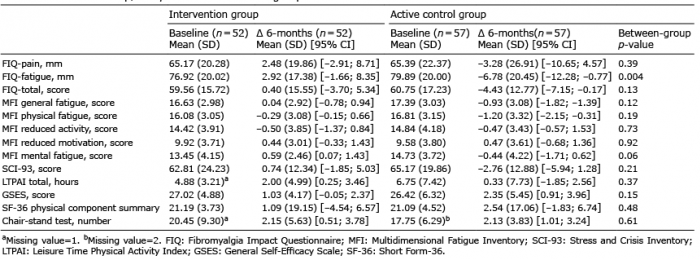 Click to show fullsize
Click to show fullsize