
From the 1Rehabilitation Medicine College, Fujian University of Traditional Chinese Medicine, Fuzhou, 2National Rehabilitation Research Center of Traditional Chinese Medicine, Fuzhou, 3Fujian University of Traditional Chinese Medicine, Fuzhou, 4Key Laboratory of Orthopedics & Traumatology of Traditional Chinese Medicine and Rehabilitation (Fujian University of Traditional Chinese Medicine), Ministry of Education, Fuzhou, China. *These authors contributed equally to this work.
Objective: The aim of this systematic review was to evaluate the effects of tai chi on metabolic control and body composition indicators in patients with type 2 diabetes mellitus.
Design: Systematic review and meta-analysis of existing literature.
Methods: Electronic resource databases were searched to collect eligible studies. Two reviewers selected studies and independently evaluated methodological quality.
Results: Twenty-three studies were included in this meta-analysis. The pooled results showed that tai chi had significant effects in improving metabolic indices, such as fasting blood glucose (mean difference (MD) = –1.04; 95% confidence interval (95% CI) –1.42 to 0.66; p < 0.01) and total cholesterol (MD = –0.50; 95% CI –0.86 to –0.13; p < 0.01) compared with conventional clinical therapy. Most indices did not support the use of tai chi over aerobic exercise, except for glycated haemoglobin (HbA1c) (MD = –0.24; 95% CI –0.49 to 0.00; p < 0.01) and high-density lipoprotein (MD = 0.07; 95% CI 0.01 to 0.12; p < 0.01).
Conclusion: Tai chi had better effects on metabolic control and body composition indicators than clinical conventional therapy, but only on HbA1c and HDL were superior than that of aerobic exercise. The best time-window for tai chi intervention may differ with different metabolic indices.
Key words: tai chi; exercise; type 2 diabetes mellitus; metabolism control; body composition; meta-analysis.
Accepted Jan 28, 2021; Epub ahead of print Feb 17, 2021
J Rehabil Med 2021; 53: jrm00165
Correspondence address: Jia Huang, Rehabilitation Medicine College, Fujian University of Traditional Chinese Medicine, Fuzhou, China. E-mail: jasmine1874@163.com; and Zhizhen Liu, Rehabilitation Medicine College, Fujian University of Traditional Chinese Medicine, Fuzhou, China. E-mail: lzz@fjtcm.edu.cn
Doi: 10.2340/16501977-2799
Exercise therapy is a possible alternative and effective strategy for blood glucose control in patients with type 2 diabetes, since drug therapy is associated with side-effects, long-term loss of efficacy, and poor adherence to lifelong treatment. A review of evidence was performed regarding the effects of tai chi on glycaemic control and other indicators in patients with type 2 diabetes mellitus. The results indicate that tai chi not only improves metabolic control, e.g. fasting blood glucose and total cholesterol, but also improves body composition indicators, e.g. body mass index. However, benefits of tai chi over aerobic exercise were seen in only a few outcome measures. The type and methodology of studies varied widely, with discrepancies in intensity, frequency, and duration of tai chi; therefore, further high-quality research is needed in order to draw specific and accurate conclusions.
The incidence of diabetes worldwide is rising, due to changing ethnic mix and ageing of the population, as well as changing lifestyles (1). According to the World Health Organization (WHO), type 2 diabetes mellitus (T2DM) accounts for 90% of all cases of diabetes (2). The International Diabetes Federation (IDF) estimates that the number of people with T2DM worldwide is projected to reach 578 million by 2030 and 700 million by 2045. As a major predictor of chronic microvascular and macrovascular complications, persistent hyperglycaemia can lead to apoptosis and damage to organs and target tissues, such as the kidneys, retina, and heart, and is associated with endothelial dysfunction, arteriosclerosis, and cardiovascular disease (CVD) (3). T2DM is also a major risk factor for end-stage renal disease (ESRD) and chronic kidney disease (CKD). The potential for abnormal blood glucose levels accelerates the renal injury caused by dyslipidaemia in patients with T2DM. In addition, dyslipidaemia and renal disease work together to worsen the clinical situation of diabetics and increase the risk of renal or cardiovascular consequences (4). Body composition indicators, such as body mass index (BMI), can predict the prognosis and complications of patients with T2DM, such as diabetic nephropathy (DKD); the predictor effect being similar to that of glycated haemoglobin (HbA1c) (5). Therefore, such indicators are of importance in monitoring disease progress and evaluating the prognosis and quality of life of patients with T2DM.
Because of the side-effects, long-term loss of efficacy and poor adherence to lifelong treatment (6) associated with drug therapy, aerobic exercise is considered an alternative and effective strategy for metabolic control in patients with T2DM (7). Tai chi is a mind-body exercise, guided by the mind and breathing. Using the waist as the pivot, the foot as the root, and the “circle” as the movement track, tai chi aims to achieve a balance of “yin” and “yang” in a combination of movement and stillness. Tai chi involves attention training, similar to meditation, and may have both physical and psychological effects, helping to control the stability of metabolic indicators. Yu et al. found that tai chi can reduce fasting blood glucose (FBG) and BMI, as well as improve quality of life (8) in patients with diabetes. However, opinions on the efficacy of tai chi vary. Lam et al. (9) found that participants who practiced tai chi showed no significant improvement in metabolic control or cardiovascular risk, while other aerobic exercises, such as brisk walking, reduced blood glucose or metabolic indicators. Therefore it is important to determine an appropriate exercise for patients with T2DM to help control metabolic indices.
The aims of this systematic review were, first, to evaluate the effects of tai chi in patients with T2DM compared with 2 kinds of control groups: routine clinical treatment; and other types of aerobic exercise; and, secondly, to explore the time taken for metabolic indices to improve with tai chi interventions.
Data sources and search strategy
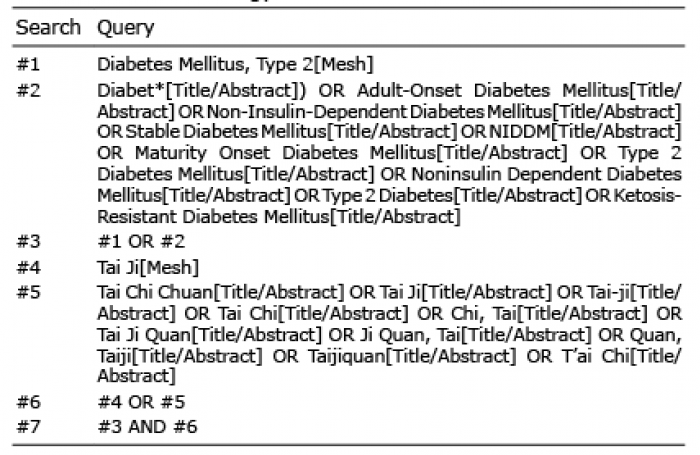
Eight electronic resource databases were searched (PubMed, Embase, MEDLINE, the Cochrane Library, Chinese Biomedical Literature Database (CBM), and China Knowledge Resource Integrated Database (CNKI)), VIP database and WanFang database. Databases were searched from inception to April 2020, using the following terms: “tai ji”, “tai chi”, “tai chi chuan”, “type 2 diabetes mellitus”, and “stable diabetes mellitus”. To achieve a complete and systematic search, synonyms were also used. Reference lists of all related studies were also consulted to identify eligible studies. The review applied Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines (10). The completed search strategy for PubMed is shown in Table I.
Table I. Search strategy for PubMed
Inclusion and exclusion criteria
The trials selected for the study met the following inclusion criteria: (i) they were published or unpublished randomized controlled studies; (ii) participants were diagnosed with T2DM; and (iii) the intervention of the experimental group was free-hand tai chi, regardless of the type; (iv) the control group received clinical conventional therapy or underwent other aerobic exercises; (v) the outcomes included measurements of glycaemic control, lipid metabolism, body composition, or insulin resistance. Studies without available data were excluded.
The studies were classified and subgroup analyses performed according to the duration of the interventions. Studies that did not explicitly define the duration of the exercise programme were excluded.
Study selection and data extraction
Two reviewers (SG and YY) independently completed data extraction, including first author, publication year, sample characteristics (sample size, mean age, sex, type of diabetes), intervention data (training time, frequency, and duration), and intervention measures of the control group. All the records were imported into the reference management software (NoteEx-press V3.2.0, Beijing Aegean software, Beijing, China) to eliminate any duplicate records. Two reviewers performed a full-text review, and, if any differences between the 2 reviewers occurred, the items were discussed with a third reviewer (ZZL) in order to reach a consensus.
Risk of bias assessment
Two investigators independently assessed the methodological quality of the included studies according to the Cochrane risk- of-bias tool (11), including the following domains: random sequence generation, allocation concealment, blinding of participants and outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias. It was difficult to blind the subjects to the interventions; therefore, the assessors were blinded. Within each domain, the risk of bias was assessed as low, unclear, or high. In the case of any disagreements, a third reviewer (ZL) was consulted to enable an agreement to be reached.
Statistical analysis
All data were recorded as mean (standard deviation; SD). If the data were reported as 95% CI or median interquartile range (IQR), the means and SDs were calculated using the appropriate statistical methods. The author was contacted to obtain the original data if the study only reported a change in outcomes. The heterogeneity of the included studies was assessed by the χ2 test and Higgins I2 value. This study defined p > 0.1, and I2 < 50% as being of no significant heterogeneity, and fixed effects models were used for the meta-analysis. If not (p ≤ 0.1 or I2 ≥ 50%), random effects models were applied. Sensitivity analyses were conducted to explore possible sources of heterogeneity and to evaluate the stability of pooled results by removing these studies one by one. A p < 0.05 was considered to indicate a significant difference between two groups. Appropriate meta-analytic approaches to determine the overall effect sizes were used when the outcomes contained at least 2 studies. If not, a descriptive analysis was performed.
To clarify the source of heterogeneity and examine whether a risk of bias may alter the synthesized results, subgroup or sensitivity analyses were performed if the heterogeneity of meta-results was high (p < 0.1 or/and I2 > 50%). All of the studies were divided into 2 groups: a short-duration group (≤ 12 weeks) and a medium-duration group (12–24 weeks); however, no studies had exercise schedules for more than 24 weeks.
A total of 613 studies were identified from the databases, and 23 studies were included in this review. The PRISMA flow diagram is shown in Fig. 1. All eligible studies were published between 2004 and 2018, and all subjects were adults with T2DM with no serious complications. Most studies were conducted in China (12–30), South Korea (31) had 1 study, while Australia, 3 studies (9, 32, 33). The characteristics of the studies are shown in Table II.
Fig.1. Flow diagram of search and selection of the studies.
Table II. Characteristic of randomized controlled trials included in the systematic review
he experimental group practiced free-hand tai chi. Tai chi sword, tai chi ball and other forms, that are practiced with equipment, were excluded. Two control groups were included in this review: a “clinical conventional therapies” (CCT) group and an “aerobic exercise” (AE) group. CCT was defined as receiving basic clinical treatment methods, including taking appropriate dose of drugs, hypoglycaemic load diets, returning to the clinic for review on time, etc. Participants in the CCT group were asked to maintain their exercise hobbies during the study, instead of adding new ones. The AE group performed exercises except tai chi; for example, brisk walking and dancing. All the studies using the AE control group reported that the intensity of exercise between groups was consistent. Two studies (14, 19) included both types of control groups.
Risk of bias of the included studies
The Cochrane Handbook for Systematic Reviews of Interventions (chapter 8.5) was used to evaluate the risk of bias. Six trials (9, 12, 14, 22, 24, 33) reported concrete methods of random sequence generation, including a centralized computer-generated allocation method (9, 12, 14, 23) or the random number table (22, 24). Only 3 studies (14, 19, 33) reported the use of allocation concealment, including sealing the opaque envelope (14, 19), or storing the random sequence in a password-protected computer (33). All studies had a high risk of “performance bias” because of the characteristics of the exercise interventions. The risk of other bias in 10 studies (9, 17–19, 23–29, 32) was judged as “high” due to the limited sample size, disproportionate dropout rates between the groups (19, 26), and other reasons (17, 18, 32, 33). The details are shown in Fig. 2.
Fig. 2. Assessment of bias risk in individual study. Green dot: low risk of bias; yellow dot: unclear risk of bias; red dot: high risk of bias. Assessment of bias risk for each study has been independently reviewed by 2 reviewers and cross checked to ensure agreement.
Effects of interventions
Glycaemic index. This review discussed the effect of tai chi on the clinical indices of blood glucose metabolism, such as FBG, HbA1c, postprandial blood glucose (PBG), and glycated serum protein (GSP). Descriptive analysis was used when meta-analysis was not available. On the basis of meta-analysis, RCTs were divided into subgroups according to the duration of intervention, and subgroup analysis was performed. Descriptive data for all the subgroup analyses of the glycaemic indices are shown in Table SI.
Compared with the CCT group, meta-results from 15 studies (13, 14, 16–21, 24–27, 29–31) showed that FBG in the tai chi group was significant (MD = –1.04; 95% CI –1.42 to –0.66; p < 0.01; Fig. 3A), but with high heterogeneity (I2 = 72%). Sensitivity analysis was conducted by removing these studies one by one, and the pooled results appeared relatively consistent. A subgroup meta-analysis showed that the tai chi group had a significant advantage over the CCT group with respect to FBG reduction in both the short-term duration group (MD = –1.54; 95% CI –2.19 to –0.88; p < 0.01) and medium-term duration group (MD = –0.57; 95% CI –0.87 to –0.28; p < 0.01).
No significant difference was found between the tai chi and AE groups in FBG reduction (MD = –0.07; 95% CI –0.38 to 0.25; p = 0.68; Fig. 3B); subgroup analysis showed similar results in the short-term duration (p = 0.08) and medium-term duration (p = 0.07) groups.
A meta-analysis of 9 (9, 13, 14, 16, 19, 20, 24, 26, 31) studies showed that the tai chi group had an advantage in the reduction of the HbA1c over the CCT group (MD = –1.28; 95% CI –2.06 to –0.51; p < 0.01; Fig. 4A), but with high heterogeneity (I2 = 98%). The pooled results of the sensitivity analysis were robust. In both the short-term duration group (MD = –0.63; 95% CI –0.43 to –0.83; p < 0.01) and medium-term duration group (MD = –2.09; 95% CI –3.03 to –1.14; p < 0.01), the tai chi group showed a significant advantage over the CCT group, and the heterogeneity of each subgroup was low (p > 0.1 or I2 <50%); therefore, the duration of exercise may be a source of heterogeneity.
Fig. 3. (A and B) Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT)/aerobic exercise (AE) group for the outcome fasting blood glucose (FBG). MD: mean difference; 95% CI: 95% confidence interval.
Fig. 4 (A and B). Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT)/aerobic exercise (AE) group for the outcome glycated haemoglobin (HbA1c). MD: mean difference; 95% CI: 95% confidence interval.
Tai chi had a strong tendency toward statistical significance in reducing HbA1c levels compared with AE (MD = –0.24; 95% CI –0.49 to 0.00; p = 0.05; Fig. 4B). Sensitivity analysis found that 4 studies (18, 22, 23, 33) can significantly affect the size of heterogeneity; removing any of the 4 studies could reduce the heterogeneity to low (p > 0.1 or I2 = 50%). The results of subgroup analysis showed that when the exercise duration was less than 12 weeks, tai chi was better than AE in HbA1c reduction (p < 0.01), but no significant difference was observed when the duration of exercise was greater than 12 weeks (p = 0.87).
Increasing evidence indicates that high PBG levels (plasma glucose concentrations 2 h after eating) plays a decisive role in the development of chronic metabolic disorders, and reducing PBG is one of main targets in the prevention and treatment of diabetes. The pooled results of 2 studies (18, 21) showed a significant advantage of tai chi on PBG reduction compared with CCT (MD = –1.58; 95% CI –1.94 to –1.22; p < 0.01; Fig. 5).
GSP is similar to HbA1c, but reflecting the usual blood glucose concentration in the past 1–3 weeks. A descriptive analysis was used to explain the results of the GSP. Zhang et al. (27) reported that the tai chi group had a potential advantage over the CCT group, but there were no statistical differences (p = 0.85) in GSP; no significant differences were found when compared with AE (28) (p = 0.06).
Fig. 5. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT) group for the outcome postprandial blood glucose (PBG). MD: mean difference; 95% CI: 95% confidence interval.
Lipid metabolism index. Lipid metabolism indices, such as total cholesterol (TC), triglyceride (TG), and high and low-density lipoprotein (HDL and LDL), were considered in this review. Descriptive data for all the subgroup analyses of lipid metabolism indices are shown in Table SI.
The meta-results of 11 studies (9, 13, 14, 16, 17, 19–21, 27, 29, 30) revealed that tai chi had a better effect on reducing TC than did CCT (MD = –0.50; 95% CI –0.86 to –0.13; p < 0.01; Fig. 6A). A sensitivity analysis was performed, and the pooled results appeared relatively consistent. Details of the subgroup analysis are provided in Table SI.
Compared with AE, tai chi did not show any advantage in reducing TC (MD = –0.08; 95% CI –0.24 to 0.09; p = 0.36; Fig. 6B), and the meta-results of each subgroup were not statistically significant.
The advantages of tai chi over CCT in reducing TG levels have been observed (MD = –0.38; 95% CI –0.65 to –0.10; p < 0.01; Fig. 7A), but with high heterogeneity (I2 = 88%). Sensitivity analysis was performed by removing the contained studies one by one, but the pooled results appeared relatively consistent. Only one study (Zhu 2017 (30)) used an intervention duration of 12–24 weeks, but with no significant differences between the tai chi and CCT groups.
Fig. 6. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT)/aerobic exercise (AE) group for the outcome total cholesterol (TC). MD: mean difference; SMD: standardized mean difference; 95% CI: 95% confidence interval.
Fig. 7. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT)/aerobic exercise (AE) group for the outcome triglycerides (TG). MD: mean difference; SMD: standardized mean difference; 95% CI: 95% confidence interval.
Four studies (14, 12, 23, 28) reported the effects of TG reduction, but there was no evidence to support an advantage of tai chi over AE (MD = 0.04; 95% CI –0.22 to 0.31; p = 0.75; Fig. 7B). A subgroup analysis was conducted to explore the possible sources of heterogeneity (I2 = 88%). When exercise duration was no more than 12 weeks, tai chi had better effects than AE (MD = –0.18; 95% CI –0.32 to –0.04; p = 0.01), but no significant difference was observed between tai chi and AE when the exercise duration was 12–24 weeks (p = 0.20). The heterogeneity of the 2 subgroups was low (I2 <50%).
In contrast to other indices of lipid metabolism, an increase in HDL within a certain range has beneficial effects on health outcomes. Compared with CCT, tai chi had a significant advantage in improving HDL levels (MD = 0.13; 95% CI 0.06–0.20; p < 0.01; Fig. 8A), but the heterogeneity was high (I2 = 58%). The pooled results of the sensitivity analysis appeared relatively consistent.
Meta-analysis showed that tai chi had better effects on HDL than AE (MD = 0.07; 95% CI 0.01–0.12; p < 0.05; Fig. 8B), and the heterogeneity was low (I2 < 50%). Subgroup analysis showed that when the exercise duration was no more than 12 weeks, tai chi maintained its advantage (p < 0.05); however, when the exercise intervention period was more than 12 weeks, the difference was not statistically significant (p = 0.59).
Tai chi had a significant effect on LDL (MD = –0.36; 95% CI –0.59 to –0.12; p < 0.01; Fig. 9A) levels compared with CCT. Subgroup analysis revealed that the advantage of tai chi was maintained only when the duration of exercise was more than 12 weeks (p = 0.02), which indicated at least 12 weeks of tai chi training was needed to produce a significant effect on LDL reduction.
The effects of tai chi and AE on LDL reduction were not significantly different (MD = 0.01; 95% CI –0.18 to 0.19; p = 0.94); and this was the conclusion from both of the subgroups (p < 0.05).
Fig. 8. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT)/aerobic exercise (AE) group for the outcome high density lipoprotein (HDL). SMD: standardized mean difference; 95% CI: 95% confidence interval.
Fig. 9. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT)/aerobic exercise (AE) group for the outcome low density lipoprotein (LDL). MD: mean difference; 95% CI: 95% confidence interval.
Body composition indices
Body composition indices were chosen that reflected the overall health status, such as BMI, waist circumference (WC), and blood pressure (BP). Indices that reflect the degree of insulin resistance, such as index of homeostasis model assessment of insulin resistance (HOMA-IR) and fasting serum insulin (FINs), were also included. Descriptive data of all subgroup analyses of body composition indices are shown in Table SI.
The effect of tai chi in reducing BMI was statistically significant compared with CCT (MD = –1.15; 95% CI –1.79 to –0.51; p < 0.01) (Fig. 10). This advantage was observed in the tai chi group, whether the exercise programme duration was ≤ 12 weeks (p = 0.03) or 12–24 weeks (p < 0.05), and the heterogeneity was low (I2 = 0%). Only one study (12) reported the advantage of tai chi over AE in lowering BMI, and no significant difference was observed (p > 0.05).
Meta-analyses of the effects of tai chi on systolic blood pressure (SBP) and diastolic blood pressure (DBP) were conducted. Compared with CCT, tai chi significantly reduced both SBP (MD = –11.86; 95% CI –14.47 to –9.25; p < 0.01, Fig. 11A) and DBP (MD = –9.58; 95% CI –11.52 to –7.63; p < 0.05, Fig. 11B). In DBP, the heterogeneity was reduced to 0% with the removal of Chan’s trial. A review of the original text of this study indicated that the specificity of participants (T2DM with 2–3 risk factors for CVD) may have contributed to heterogeneity with other studies. The results of subgroup analysis showed that tai chi had significant effects on SBP and DBP in patients with T2DM (p < 0.05), regardless of whether they were in the short-duration (≤ 12 weeks) or medium-duration (12–24 weeks) group.
Fig. 10. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT) group for the outcome body mass index (BMI). MD: mean difference; 95% CI: 95% confidence interval.
Fig. 11. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT) group for the outcome systolic blood pressure (SBP) and diastolic blood pressure (DBP). MD: mean difference; 95% CI: 95% confidence interval.
Tai chi had a significant effect on FINs compared with CCT (MD = –2.63; 95% CI –4.51 to –0.76; p < 0.05, Fig. 12). The results of the subgroup analysis explained the high heterogeneity of the meta-analysis (I2 = 90%), and significant results were observed in both exercise duration subgroups (p < 0.05). The advantage of tai chi in the CCT group was also shown on HOMA-IR (MD = –1.02; 95% CI –1.39 to –0.64; p < 0.05; Fig. 13).
Fig. 12. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT) group for the outcome fasting serum insulin (FINs) and index of homeostasis model assessment of insulin resistance (HOMA-IR). MD: mean difference; 95% CI: 95% confidence interval.
Fig. 13. Forest plot of the comparison between tai chi and the clinical conventional therapy (CCT) group for the outcome fasting serum insulin (FINs) and index of homeostasis model assessment of insulin resistance (HOMA-IR). MD: mean difference; 95% CI: 95% confidence interval.
Diabetes treatment constitutes one of the highest costs in healthcare systems and it is increasing each year (35). Most drugs inhibit glucose production and absorption by increasing insulin production and utilization (36); however, drug treatments that control disease progression are not without side-effects. Exercise, including tai chi, has been used widely as a complementary alternative supplement therapy to improve the quality of life-related outcomes (physical function, bodily pain, and social function) of patients with T2DM (37). However, there is no consistent conclusion regarding whether tai chi can affect glycaemic control, lipid metabolism, and body composition in patients with T2DM.
The results of the meta-analysis showed that when compared with CCT, Tai Chi can reduce FBG, HbA1c, PBG, TC, TG, LDL, BMI, BP, HOMA-IR, and FINs, and increase HDL. However, only in reducing HbA1c and increasing HDL, we observed the better effect of Tai Chi compared with aerobic exercise. Participants in the tai chi and AE groups practiced exercises of equal intensity and duration, hence it can be assumed that the calories consumed in both groups were similar. Articles included in the current review explored possible reasons for the differences between the groups. The key benefits of tai chi lie not in calorie consumption, but in the efficacy of enhanced metabolism, cardiopulmonary function, and anti-oxidation and anti-inflammatory activation, which can help decrease lipid and oxidative levels and prevent cardiovascular risks in patients with T2DM (12). As a typical mind-body exercise, tai chi combined moderate physical with psychological activities. Psychological activities, such as meditation, produce a specific physiological response pattern that involves various biological systems. The most frequently suggested mechanism of meditation is that it produces effects, including metabolic, autonomic, endocrine, neurological, cardiovascular, and psychological responses, on a multidimensional interactive basis. A meta-analysis of 21 studies concluded that meditation significantly reduced FBG, HbA1c, PBG, TC, and LDL levels in patients with T2DM (38). The study confirmed that exercise self-efficacy was observed in the tai chi group; hence it was easier to continue with exercise as part of daily life and cultivate this action as a daily habit (14).
Previous studies have found that tai chi can improve glucose metabolism and reduce HbA1c and insulin resistance (39). Tai chi has been introduced to health professionals as a moderate-intensity aerobic exercise that has the characteristics of comprehensive exercise of aerobic exercise and resistance exercise. In the process of exercise, it especially stimulates small muscle groups, such as fingers and peripheral tissues, which is beneficial to the promotion of blood circulation and the absorption and utilization of glucose in peripheral tissues. Most patients with T2DM also experience hyperlipidaemia. Studies have reported that, for every 1 mmol/L increase in TC level, women’s risk of CVD increases by 20% and men’s by 24% (40). Previous studies have shown that HDL levels are negatively correlated with the risk of CVD. The benefits of increased HDL include longer CVD-free time, maintenance of endothelial function, oxidative protection of LDL, and inflammatory protection. The current study found that tai chi was beneficial for the improvement of HDL levels compared with CCT or AE in this meta-analysis, which may mean that tai chi is a better method to reduce the risk of CVD than other forms of aerobic exercise or clinical routine treatment.
BMI (41) and WC have been confirmed as reliable predictors of diabetes (42) in previous systematic reviews, and proper physical exercise can reduce the risk of BMI and diabetes (7). A cross-sectional study in a healthy elderly population showed that mild to severe physical exercise is associated with lower BMI (43). Studies have shown that total energy consumption is an evolutionary, species-specific trait that is buffered in the body to prevent changes in physical activity habits; therefore, energy imbalance must be maintained for a longer period of time before detectable changes in body composition occur, usually over weeks, rather than days (44). The intervention period of RCTs included in this meta-analysis was at least 8 weeks (34), which we consider was sufficient to cause meaningful changes in body composition indicators.
The results of this review suggest that tai chi is better than CCT in reducing BP, and previous systematic reviews have suggested that tai chi may have a greater effect on BP than aerobic exercise, which can reduce SBP by 7 mmHg and DBP by 5 mmHg (45). Unfortunately, this review did not compare BP between tai chi and aerobic exercise in patients with T2DM, due to the limitations of the included studies. Therefore, it was not possible to draw a clear conclusion in this regard, i.e. whether there are differences in BP regulation between tai chi and aerobic exercise in patients with T2DM. Although not for patients with T2DM, systematic reviews in recent years have revealed that tai chi significantly reduced both SBP and DBP over a period of > 12 weeks in all studies (46); whether this result is applicable to patients with T2DM remains to be further studied. The increased risk of heart failure in patients with T2DM may be regulated by factors specific to T2DM, such as insulin resistance (47). Tai chi is more beneficial than CCT in regulating HOMA-IR and FINs. PBG and HOMA-IR were measured in only 2 or 3 studies, and the results of this measure should be viewed with caution.
A subgroup analysis was conducted according to the duration of the exercise. Exercise duration was divided into short-term (≤ 12 weeks) and medium-term (12–24 weeks). The results differed after the subgroup analysis, which may reveal the key points that should be paid attention to when tai chi is used as an intervention in clinical practice. There was no difference between tai chi and aerobic exercise on reduction in TG, but the subgroup meta-results showed that tai chi had an advantage over aerobic exercise when the exercise duration was no more than 12 weeks. Similarly, the effect of tai chi on reducing HbA1c was better than that of aerobic exercise when the exercise duration was ≤ 12 weeks, but no significant difference was observed in the 12–24-week exercise duration. These results may indicate that tai chi can improve some metabolic indices in a relatively short time.
This review included only randomized controlled trials, which implied that the included studies had a rigorous research design. However, limitations and shortcomings must be emphasized. First, in some cases, this study could not directly use the data provided from the literature due to inconsistent data formats. We had to calculate and transform data. Secondly, most of the studies were conducted in China, which may have affected the meta-analysis results. The schools and types of tai chi vary. Many studies asked subjects to modify their intensity according to their own feelings, rather than using a fixed intensity. Therefore, this review did not investigate the effects of different intensities of tai chi on metabolic indices.
Tai chi had a better effect on glycaemic control, lipid metabolism, and body composition compared with clinical conventional therapy (CCT), and was superior to aerobic exercise in improving some metabolic control. The best intervention time-window for tai chi may differ for different metabolic indices. Considering the different types of tai chi, the discrepancies in intensity, frequency, duration, the limited number of studies and small sample size, further high-quality research is needed to draw specific and accurate conclusions.
Adverse events
No adverse events were reported in the studies included in this review.
Clinical implications and recommendations for future studies
Firstly, the main purpose of this review was to observe the advantages of tai chi over CCT and AE, hence the types of tai chi were not classified. Secondly, the quality of the studies is not high, and the conclusions should be treated with caution. Future studies in this field should explore appropriate tai chi training duration (e.g. intensity, duration, frequency) for patients with T2DM. At the same time, follow-up studies are needed to assess the long-term benefits of tai chi treatment. In addition, in order to better assess the quality of the research, the author should follow the CONSORT guidelines when reporting research.
Funding support. This study is supported by: The Key Research and Development Project funded by the Ministry of Science and Technology of the People’s Republic of China (grant number 2019YFC1710301); Science and technology platform construction project of Fujian science and Technology Department (grant number 2018Y2002); and Fujian Key Laboratory of Rehabilitation Technology, Fuzhou, China.
Clinical trial information. The protocol of this study was registered with the International Prospective Register of Systematic Review, PROSPERO, under the identification number CRD42020191377, and can be integrally assessed online. (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID = 191377).
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize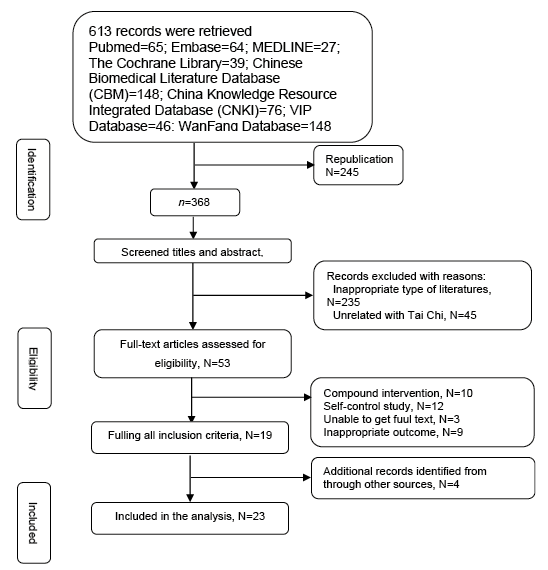 Click to show fullsize
Click to show fullsize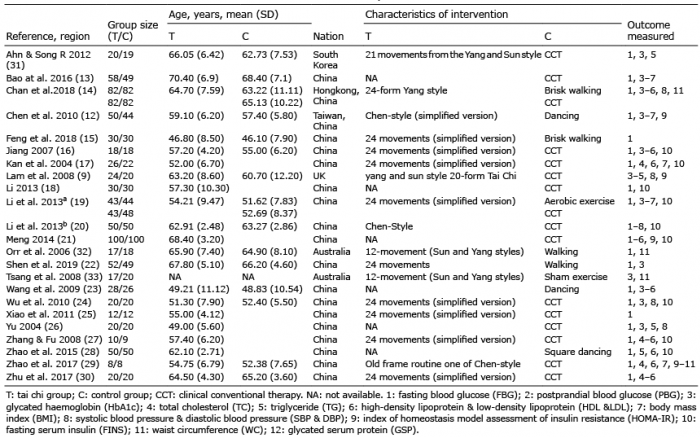 Click to show fullsize
Click to show fullsize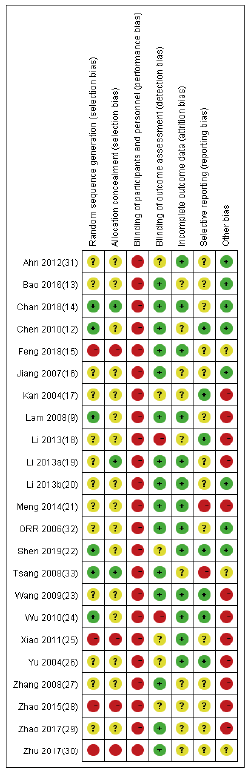 Click to show fullsize
Click to show fullsize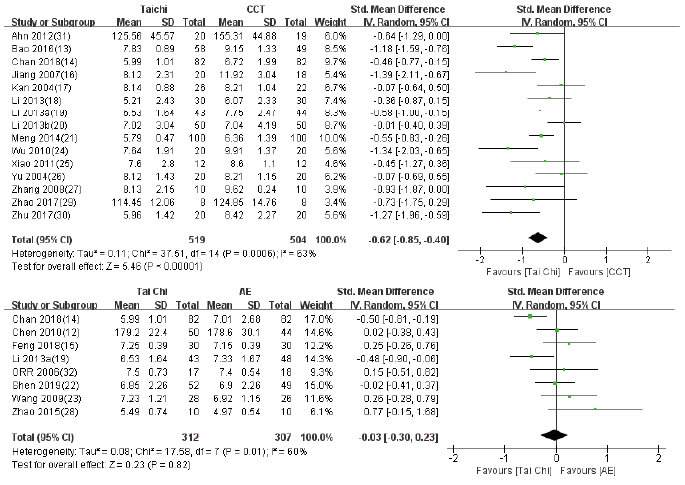 Click to show fullsize
Click to show fullsize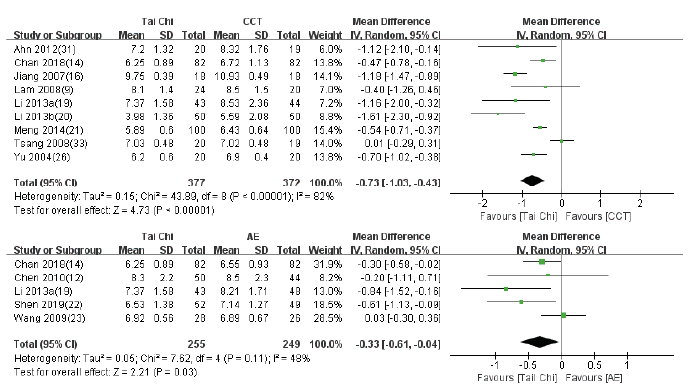 Click to show fullsize
Click to show fullsize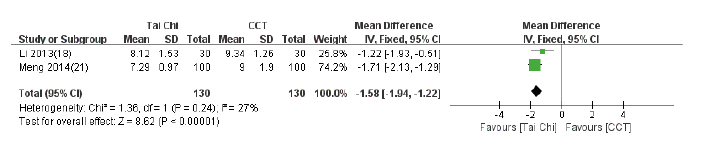 Click to show fullsize
Click to show fullsize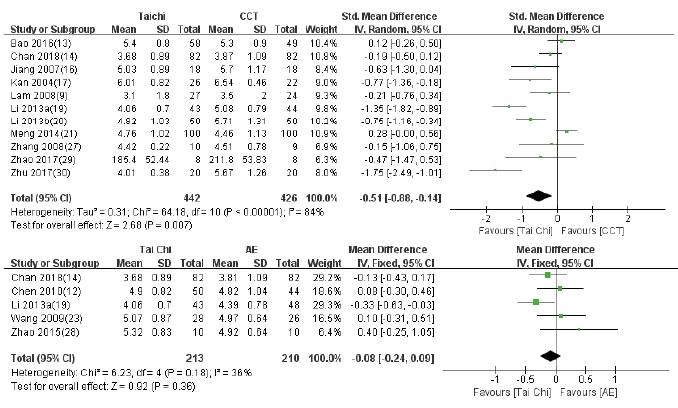 Click to show fullsize
Click to show fullsize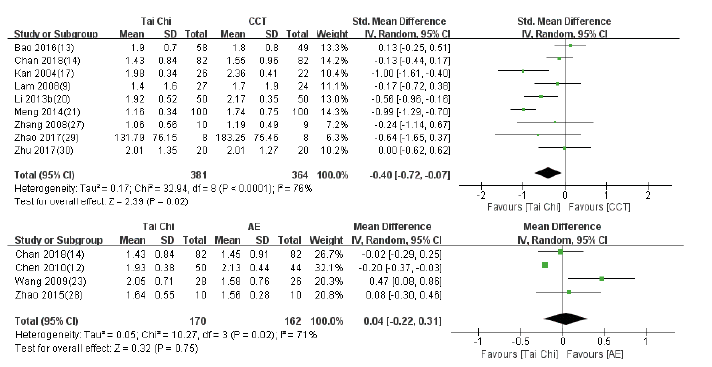 Click to show fullsize
Click to show fullsize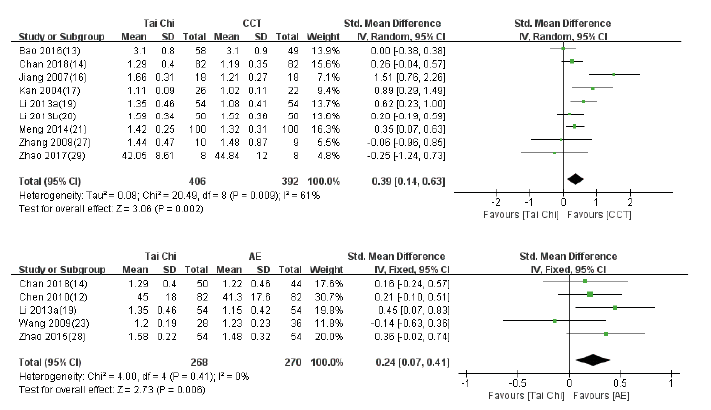 Click to show fullsize
Click to show fullsize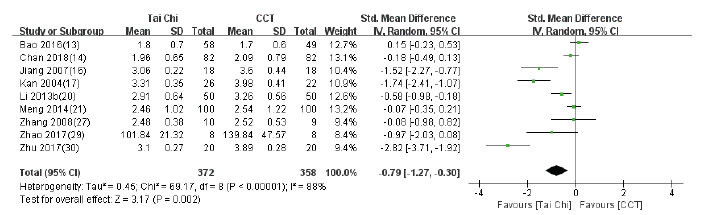 Click to show fullsize
Click to show fullsize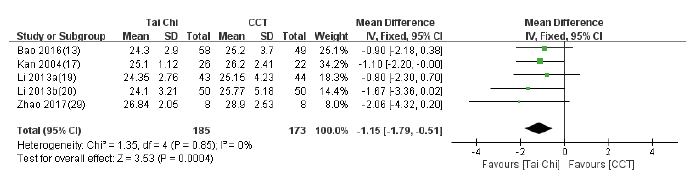 Click to show fullsize
Click to show fullsize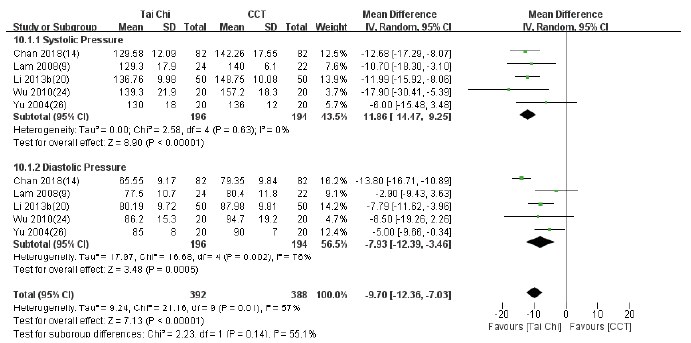 Click to show fullsize
Click to show fullsize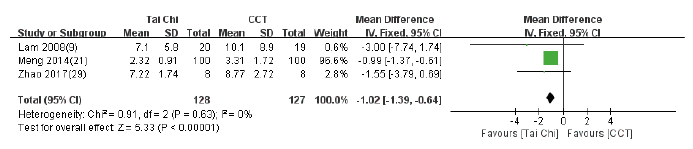 Click to show fullsize
Click to show fullsize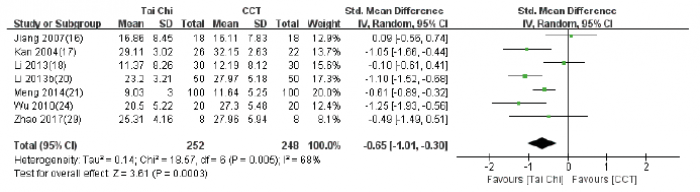 Click to show fullsize
Click to show fullsize