
From the 1Department of Rehabilitation Medicine, Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, Guangdong, China and 2Department of Rehabilitation Medicine, Maoming People’s Hospital, Maoming, Guangdong, China
*These authors contributed equally to this work.
Objective: To explore the effects of transcranial direct current stimulation combined with cognitive training on executive function and activities of daily living performance among stroke patients.
Methods: A total of 50 subjects were enrolled and randomly allocated into 2 groups of 25 each. The real-transcranial direct current stimulation group was simultaneously subjected to transcranial direct current stimulation and cognitive training, while the sham-transcranial direct current stimulation group was simultaneously subjected to sham transcranial direct current stimulation and cognitive training. At baseline, and after treatment, each subject was assessed with the Wisconsin Card Sorting Test (WCST), Stroop Color-Word Test (SCWT), Digital Symbol Test (DST), Mini-mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA) and Activities of Daily Living Scale (ADLs).
Results: After treatment, the gains in most indices of WCST, SCWT, DST, MMSE, MoCA and ADLs in the real-transcranial direct current stimulation group were significantly higher than those in the sham- transcranial direct current stimulation group (p < 0.05). Nonetheless, no significant differences were noted in the gains in SCWT (including only Part A time and error, and Part B time) and activities of daily living (including only basic activities of daily living) between the 2 groups (p > 0.05).
Conclusion: Transcranial direct current stimulation combined with cognitive training was found to significantly enhance executive function and instrumental activities of daily living performance among stroke patients.
Key words: transcranial direct current stimulation; executive function; cognitive training; activities of daily living; stroke.
Accepted Feb 11, 2021; Epub ahead of print Feb 26, 2021
J Rehabil Med 2021; 53; jrm00162
Correspondence address: Xi-Quan Hu, Department of Rehabilitation Medicine, Third Affiliated Hospital of Sun Yat-Sen University, 600 Tianhe Road, Guangzhou 510630, Guangdong Province, China. E-mail: xiquhu@hotmail.com. Zhen-Hong Liang, Department of Rehabilitation Medicine, Maoming People’s Hospital, Maoming, Guangdong Province, China. E-mail: 1454825714@qq.com
Doi: 10.2340/16501977-2807
Executive function is the ability of an organization to plan and solve problems. The efficacy of use of a combination of transcranial direct current stimulation and cognitive training in the treatment of executive dysfunction among stroke patients remains undetermined. This is the first randomized controlled study of the effects of such treatment. The results indicate that a combination of transcranial direct current stimulation and cognitive training significantly enhances executive function and instrumental activities of daily living performance among stroke patients.
Stroke presents a serious threat to human health and safety, causing cognitive impairment, motor impairment and aphasia (1). Executive function, as an advanced cognitive function, reflects a comprehensive ability to solve problems. Post-stroke executive impairment (PSEI) is a prevalent sequelae of stroke that inhibits complete recovery, social participation, return to work, and activities of daily living (ADL) (2, 3). Epidemiologically, an estimated 75% of acute stage and 66% of recovery stage stroke patients exhibit various levels of executive dysfunction (4). Although conventional table-top cognitive training, task-oriented training, and medications improve PSEI to some degree, they are uninteresting, slow-acting, time-consuming, and poorly adhered to by patients (5). The efficacies of available therapies for PSEI are unsatisfactory; as such, there is an urgent need for the development of novel alternative treatments.
Transcranial direct current stimulation (tDCS) is a safe non-invasive and painless electrophysiological technology, currently applied in neurological and mental rehabilitation (6–8). Studies suggest that tDCS enhances post-stroke cognitive impairment (PSCI) (9), and executive dysfunction among healthy adults, patients diagnosed with Parkinson’s disease, and schizophrenia, among other diseases (10–12). The efficacy of tDCS in improving executive function in these populations depends on underlying internal mechanisms, including increasing cerebral blood flow perfusion, enhancing cerebral blood flow velocity, decreasing synaptic activity of γ-aminobutyric acid (GABA), improving N-methyl-D-aspartate (NMDA) receptor function, and modulation of synaptic plasticity (13, 14).
Computer-assisted cognitive training is entertaining and interesting because of the vivid images, multi-sensory feedback and rich materials, which easily improves the active cooperation of patients. A randomized controlled trial (RCT) found that computer-assisted cognitive training effectively promotes recovery from PSCI, potentially because it improves cerebral blood flow and brain metabolism in the damaged areas (15).
Nevertheless, there is a paucity of scientific evidence supporting the combinational use of tDCS and cognitive training as a therapeutic option for PSEI. Moreover, its associated efficacy is unestablished. It was hypothesized that the combination of tDCS and cognitive training effectively treats PSEI and ADL dysfunction. Therefore, this study evaluated the therapeutic efficacy of combinational use of 2.0 mA tDCS and cognitive training on PSEI and ADL, geared towards exploring and optimizing its therapeutic options for clinical treatment.
Study site and participants
This study was performed at the Department of Rehabilitation Medicine, Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China. In total, 50 patients diagnosed with stroke executive impairment admitted to the hospital between June 2018 and July 2020 were randomly assigned into 2 treatment groups 25 patients; the Real-tDCS treatment group and the Sham-tDCS treatment group.
Inclusion and exclusion criteria
Inclusion criteria were; (i) diagnosed with stroke; (ii) screened for cognitive dysfunction by MMSE (total score less than 24) and MoCA (total score less than 26); (iii) screened for executive dysfunction by the visual space and executive function subtest of MoCA (less than 4 out of 5 points); (iv) in stable condition and can complete the test with a pen; (v) first onset and course of disease (6–18 months); (vi) aged between 18 and 75 years; and (vii) capable of giving informed consent for the study.
Exclusion criteria were: (i) intracranial metal implants or skin lesions on target sites for stimulation; (ii) neurological or psychiatric disorders; (iii) severe cardiopulmonary, renal, and hepatic diseases; (iv) visual and hearing disorders; and (v) pregnancy.
Study design
Notably, this randomized controlled study was single-blind i.e. a computer-generated 1: 1 randomization table, created by a statistician not involved in the study, was used to randomly allocate subjects into the Real-tDCS and Sham-tDCS groups. Group assignments were confidentially placed in sealed opaque envelopes kept in a central locked cupboard by independent researchers not involved in the study.
After the initial assessment, the allocation scheme was disclosed to an occupational therapist, who performed rehabilitation with all subjects. The subjects were assessed by a blinded physician at baseline and the end of treatment (after 4 weeks). All the involved researchers, therapists, and physicians were trained on the use of the assessment tools before the start of the study.
Participants in the Real-tDCS group received both real tDCS stimulation and cognitive function training, whereas those in the Sham-tDCS group received both sham tDCS stimulation and cognitive function training. At baseline and after treatment, every participant was assessed by WCST, SCWT, DST, MMSE, MoCA, and ADLs.
Transcranial direct current stimulation
The tDCS was performed using a battery-driven, constant-current stimulator Model 8060 (Yimai Medical Technology Co., Ltd, Wuhan, China). This stimulator uses a 25 cm2 (5 × 5) isotonic saline sponge electrode as the stimulant. Studies show that the left dorsolateral prefrontal cortex (DLPFC) is closely associated with executive function performance (16–18). Therefore the left DLPFC was chosen as the stimulus target. The anode was placed at the left DLPFC, and the cathode was placed at the right DLPFC. The positioning of the electrodes was based on the international 10–20 electroencephalography (EEG) system. Stimulation, starting and ending simultaneously with cognitive function training, was applied continuously at an intensity of 2.0 mA. The treatments were scheduled for 5 sessions per week (Monday to Friday) over a span of 4 weeks for each study subject. In the sham stimulation, the current was delivered for 30 s and discontinued (19); however, the tDCS apparatus was left in place for 20 min, to mimic the real tDCS treatment (20 min). The stimulation sites were similar for both treatment groups.
Cognitive function training
Based on Withiel et al. (20), these procedures were performed using a computer. Study participants were simultaneously subjected to structural ability training (spatial understanding, spatial integration, and spatial structure training), reasoning ability training (sequence reasoning, spatial reasoning, and similarity training), and simulated daily task-oriented training (diary writing and shopping). During training, the therapist administered corresponding oral guidance based on the severity of the executive dysfunction of the participants. The difficulty and intensity of the training were varied gradually from easy to difficult. The treatments were scheduled for 20 min per session, 5 sessions a week (Monday to Friday), over a span of 4 weeks for each study participant.
Assessment methods
The selection of assessment methods was based on the International Classification of Functioning, Disability and Health (ICF), which provides a comprehensive evaluation of PSEI patients at the level of functional structure and activity participation.
Primary outcome measurements
The Wisconsin Card Sorting Test (WCST) was used to detect the abilities of study participants in abstract generalization, concept formation, and stereotype transformation. This test comprises 48 response cards and 4 stimulus cards. Based on colour, shape, and number, the study participants were asked to match a series of cards upon a command from the therapist. During the test, the participants were uninformed on the rules, but were informed on whether the right choices had been made each time. An accuracy rate of less than 60% for each indicator showed varying degrees of executive dysfunction (21).
The Stroop Color-Word Test (SCWT) was applied to evaluate the abilities of participants in perception conversion, selective attention, and inhibition of habitual response. This test comprised 3 cards. Card A was painted with red, green, yellow, and blue circles. The study participants were asked to tell the colours of the circles as quickly and as accurately as possible. The Chinese characters “go, up, sun, pass” and “red, green, yellow, blue” were written on cards B and card C in yellow, red, blue, and green, respectively. The participants were required to read the colours of the characters, where a score below 39 indicated executive dysfunction (22).
The Digit Symbol Test (DST) was used to measure the flexibility, learning, and conversion ability of participants. It is an efficient tool for evaluating executive function. The reference section of the DST comprises 9 numbers and 9 symbols corresponding to the numbers. The participants were asked to fill in the space below the number based on the reference section. The test time limit was 90 s, where a total score of 65 points, less than 21 points indicated executive dysfunction (23).
Secondary outcome measurements
The Mini-mental State Examination (MMSE) was performed in the overall cognitive function examination of each study participant. A total score of 24 or less indicated the presence of cognitive impairment, a score of 21–24 implied the presence of mild cognitive impairment, a score of 10–20 implied moderate cognitive impairment, while a score of 0–9 implied severe cognitive impairment (24).
The Montreal Cognitive Assessment (MoCA) was used for screening cognitive and executive functions. A total score of less than 26 suggested the presence of cognitive function impairment. On the other hand, the visual space and executive function subtest of MoCA, with a score of less than 4 out of 5 points, indicated the existence of executive dysfunction (25).
The Activities of Daily Living Scale (ADLs) test was performed to evaluate the ADL ability of the study participants. This test comprised 2 sub-scales of basic activities of daily living (BADL) and instrumental activities of daily living (IADL). The BADL scale included basic daily activities including dressing, washing, and transferring with a total score of 32, while the IADL scale included complex daily activities including shopping, financial management, and telephone use, with a total score of 48 (26).
Ethics approval
Ethics approval was obtained from the ethics committee of the Third Affiliated Hospital of Sun Yat-Sen University (reference number [2016] 2-151). The research was registered at Chictr.org (Chinese Clinical Trial Registry Unique Identifier: ChiCTR1900025467) on August 27, 2019, and was performed in compliance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for human experiments.
Statistical analysis
Categorical variables were presented as frequencies and percentages. Normally distributed continuous variables were presented as the mean and standard deviation (SD), while non-normally distributed continuous variables were expressed as medians with the first and third quartiles. Baseline characteristics were compared between the Real-tDCS group and the Sham-tDCS group using the independent sample t-test for continuous variables and the χ2 tests for categorical variables. Independent samples t-test (normal distribution variables) and Mann–Whitney U test (non-normal distribution variables) were used to test for significant difference in gains between the 2 groups. The IBM SPSS 25.0 statistical program (IBM Corp, Armonk, NY, USA) was used for statistical analysis. Statistical significance was set at p < 0.05.
Demographic and clinical characteristics
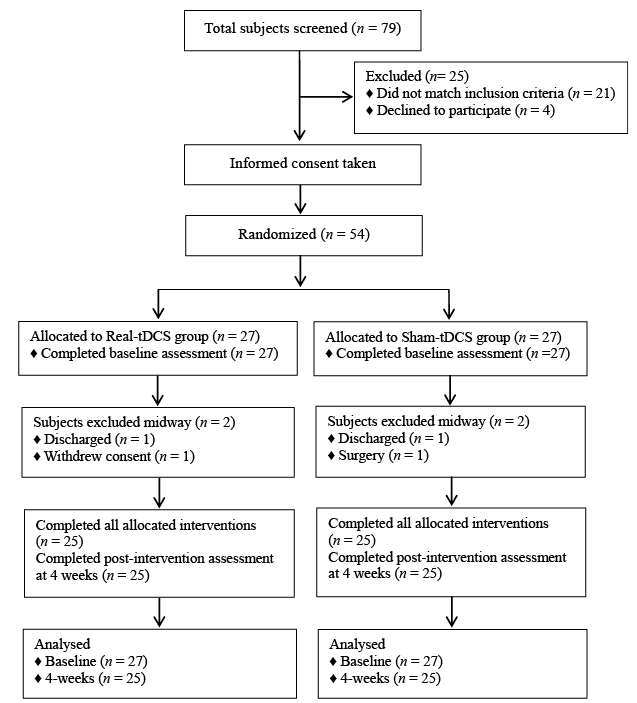
The study flow diagram is shown in Fig. 1. Table I presents a summary of the demographic and clinical features of all study participants. A total of 25 participants, median age 65 years, 15 males and 10 females, were enrolled in the Real-tDCS group. A total of 25 participants, median age 64 years, 12 males and 13 females, were enrolled in the Sham-tDCS group. No significant differences in baseline characteristics were noted between the 2 treatment groups. MMSE was used to examine the cognitive function of participants with mild, moderate, and severe cognitive impairments. No significant difference in the number of participants with mild, moderate, or severe cognitive impairment was noted at baseline.
Fig. 1. Consolidated Standards of Reporting Trials (CONSORT) study flow diagram. tDCS: transcranial direct current stimulation.
Table I. Demographics and clinical characteristics of all study participants at baseline
Changes in primary outcome measures
The primary outcome measurement scores are shown in Table II. After treatment, the gains observed in WSCT, SCWT (including the errors in part B, the time and the errors in Part C) and DST in the Real-tDCS group were significantly greater than those observed in the Sham-tDCS group (p < 0.05). No significant differences were found in gains of SCWT (including the time and the errors in part A, the time in part B) between the 2 groups. The overall improvement in DST did not exceed its minimal clinically important difference (MCID) value, which was 17.1% of the total score, or 11 points.
Table II. Changes in primary outcome measures for all study participants
Changes in secondary outcome measures
The secondary outcome measurement scores are shown in Table III. After treatment, improvements in MMSE, MoCA, and ADLs (including IADL) scores were significantly better in the Real-tDCS group than in the Sham-tDCS group (p < 0.05). Nevertheless, no significant difference in the BADL scores was found between the 2 groups. The overall improvement of MoCA did not exceed the MCID value of 13.3% of the total score, or 4 points.
Side-effects
During stimulation, 4 participants in the Real-tDCS group and 2 participants in the Sham-tDCS group experienced mild side-effects, including headaches or skin redness under the stimulation site.
Table III. Changes in secondary outcome measures for all study participants
The results reveal that executive function and IADL ability scores in the Real-tDCS group were significantly better than those in the Sham-tDCS group. Therefore, a combination of tDCS and cognitive function training improves executive dysfunction and IADL function among stroke patients. Moreover, its efficacy was superior to cognitive function training alone. These outcomes validate the study hypothesis and will be useful for optimizing the clinical treatment plan for PSEI.
Despite being shown to enhance executive function in healthy adults and patients with schizophrenia and Parkinson’s disease, studies on tDCS treatment of PSEI are lacking. Gorlick et al. (27) performed tDCS stimulation of the dorsal prefrontal cortex on 20 healthy adults, and found that tDCS significantly enhanced their executive function within a month. However, their results would be more convincing if they had used more assessment tools rather than the Hayling task alone. Doruk et al. (28) investigated the immediate and long-term effects of 10 consecutive anodal tDCS sessions on the right DLPFC (5 cases), and the left DLPFC (6 cases). Also, a sham stimulation was conducted on 7 cases, and eventually, tDCS enhanced executive function in patients with Parkinson’s disease. Nevertheless, their conclusions were limited by the small sample size. Orlov et al. (29) recruited 28 patients with schizophrenia and treated them with sham or tDCS stimulation. They reported a significant improvement in the executive function and working memory abilities of patients with schizophrenia. Unlike the above-described studies, the participants in the current study were all in the chronic stages of stroke, the sample size was larger, and the assessment tools were more comprehensive.
This study indicates that tDCS sham stimulation and cognitive function training might help improve executive function in stroke patients, consistent with the results of Shaker et al. (9). Stimulation by sham tDCS might improve executive function through non-specific effects, including induced muscle movements, tactile and temperature sensory inputs. These peripheral movements and somatosensory sensations produced a placebo effect and reduced the promotion effect in the cortex, with an impact on the psychological and physiological levels of patients (30). In addition, cognitive training based on computer games enhanced the active cooperation of participants because of the vivid and rich game pictures. Improvement in executive function was attributed to the entertaining nature of the computer games, which engaged the attention of participants. This effect relieved negative emotions, increased cerebral blood flow and cerebral metabolism in the damaged areas (31). Moreover, communication with family and medical staff improved the self-worth of patients, maintaining their enthusiasm and interest in rehabilitation therapy (32).
Furthermore, a similar degree of enhancement was not noted in the outcomes of SCWT in patients within the Sham-tDCS group and the Real-tDCS group. This was attributed to the relatively low difficulty of parts A and B in the SCWT, reflecting reaction speed and low levels of selective attention. This was completed by participants with a basic level of cognition, for improvement in the scores of parts A and B of SCWT to some extent, but did not reflect a significant difference. On the other hand, the gains in DST and MoCA were significantly different; however, the overall improvement did not exceed their respective MCID values. Several factors were associated with the estimation of MCID values, including age, stroke type, baseline severity, and intensity of rehabilitation intervention. Future studies should focus on exploring the factors that might be associated with MCID estimation.
These findings suggest that the IADL performance of the Real-tDCS group was significantly superior to that of the Sham-tDCS group. This significance was not observed in BADL scores, since IADL is an advanced daily activity requiring a satisfactory executive function. This phenomenon could be attributed to the better executive function of patients in the Real-tDCS treatment group than in the Sham-tDCS treatment group. Moreover, BADL is a basic daily activity, requiring only basic cognitive functions and not advanced executive functions.
Based on the ICF, the evaluation methods in the current study were used to evaluate the PSEI patients for aspects of functional structure and participation. The assessment tools covered multiple aspects of executive function and ADL performance. These included WCST, which better reflected the abilities of participants to change posture, working memory, abstraction generalization, and inhibitory control. Unlike the Sham-tDCS group, the sub-scores of WCST in the Real-tDCS group were significant. This indicated that participants answered questions based on different classification rules, flexibly switched between tasks with different classification rules, and no longer repeated old behavioural patterns. Nevertheless, this scale was time-consuming and relatively difficult to administer, and hence it was difficult to obtain the cooperation of participants. The SCWT score reflected the anti-disturbance ability of participants, requiring them to have good selective attention, potential switching, and inhibition of habitual response patterns. Each sub-item score in SCWT of the Real-tDCS group was enhanced compared with the baseline. This indicated an improved speed of task performance, resistance to interference, and problem-solving. The DST test assessed fine motor, operating speed, vision-motor coordination, and persistence of the participants. The DST scores in the Real-tDCS group were significantly enhanced compared with the Sham-tDCS group. This demonstrated that tDCS could improve learning and conversion ability in PSEI patients. The ADLs scores comprised BADL and IADL components. The IADL scores improved significantly in the Real-tDCS group compared with the Sham-tDCS group, suggesting that tDCS improved IADL performance in PSEI patients.
In the course of tDCS treatment, only 6 subjects experienced mild headaches and discomfort at a low discomfort rate. These side-effects were relieved by relaxation. Moreover, no participants experienced adverse symptoms including epilepsy or syncope, nor did they experience any worsening of their condition. This indicated that tDCS was relatively safe under the specific conditions of this study.
Study limitations
The study was limited by a small sample size, short intervention period, and lack of follow-up evaluation. This prevented the determination of the long-term efficacy of tDCS on PSEI. In addition, the lack of incorporation of electroencephalogram (EEG) and functional magnetic resonance imaging (fMRI) to further explore the recovery mechanism of PSEI patients was a drawback.
Conclusion
A combination of tDCS and cognitive function training was effective in enhancing executive dysfunction and IADL performance among stroke patients. The treatment parameters of tDCS were safe and did not induce brain tissue damage. Studies with large sample sizes, multi-centre, increased follow-up sessions, and randomized controlled trials combining neurophysiological and imaging tools are needed to further investigate the long-term effects and recovery mechanisms of a combination of tDCS and cognitive function training on PSEI.
This study was supported by the National Natural Science Foundation of China (grant numbers 81871847, 81972151, 81672261, and 81702232), the Natural Science Foundation of Guangdong Province (grant number 2019A1515011106) and Science and Technology Plan Foundation of Guangzhou (grant number 201803010119).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize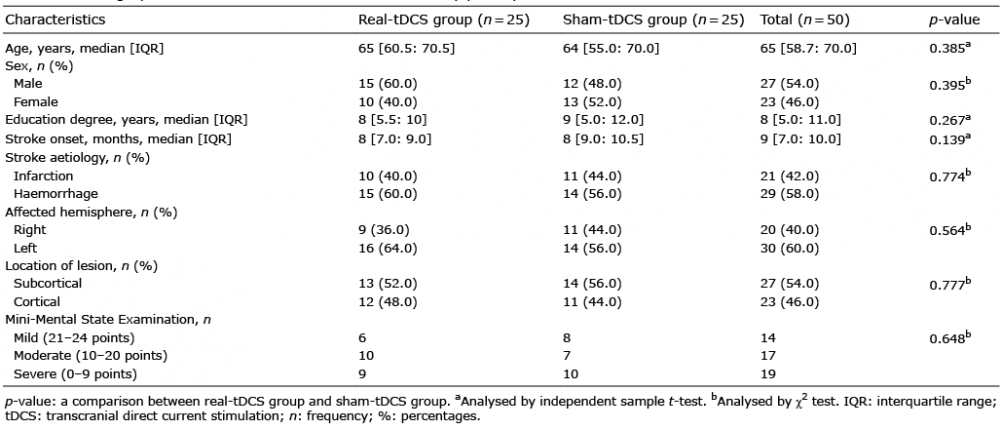 Click to show fullsize
Click to show fullsize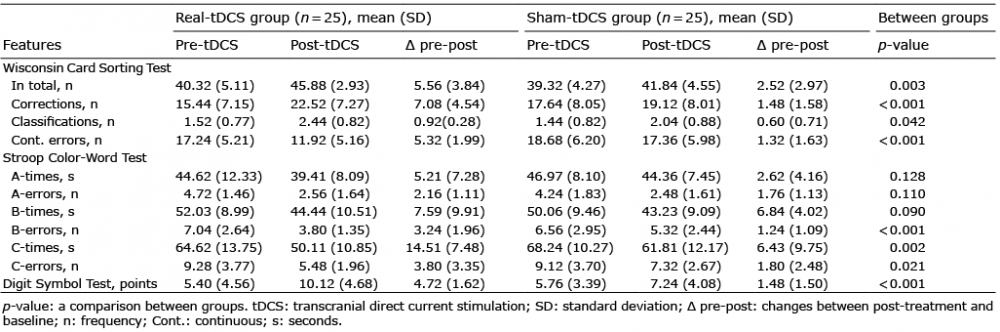 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize