
From the 1Department of Gynecology and Obstetrics, The Third Affiliated Hospital of Southern Medical University, Guangzhou and 2Department of Rehabilitation, General Practice Center, Nanhai Hospital, Southern Medical University, Foshan, China
Objective: To evaluate the effects of a rehabilitation programme for lumbopelvic pain after childbirth.
Methods: Women with lumbopelvic pain 3 months postpartum were included in a randomized controlled trial. Patients in the intervention group (n = 48) received pelvic floor muscle training combined with neuromuscular electrical stimulation of the paraspinal muscles for 12 weeks, while patients in the control group (n = 48) received neuromuscular electrical stimulation for 12 weeks. Outcomes were measured with the Triple Numerical Pain Rating Scale (NPRS), Modified Oswestry Disability Questionnaire (MODQ) and Short-Form Health Survey-36 (SF-36).
Results: The NPRS score was significantly better in the intervention group at 12 weeks compared with the control group (p = 0.000). The MODQ score was significantly better at 6 and 12 weeks compared with the control group (p = 0.009 and p = 0.015, respectively). The mean value of the Physical Components Summary of the SF-36, was significantly better in the intervention group at 6 weeks (p = 0.000) and 12 weeks (p = 0.000) compared with the control group, but there was no significant improvement in Mental Components Summary of the SF-36.
Conclusion: A postpartum programme for women with lumbopelvic pain is feasible and improves the physical domain of quality of life.
Key words: lumbopelvic pain; biofeedback; myoelectric stimulation; pelvic floor; postpartum women.
Accepted Feb 19, 2021; Epub ahead of print Mar 16, 2021
J Rehabil Med 2021; 53: jrm00180
Correspondence address: Ribo Xiong, 28# Liguan Road, Lishui County, Foshan, China. Email: xiongribo@outlook.com; Yan Liu, 183# West Zhongshan Avenue, Guangzhou, Guangdong Province, China. E-mail: 19714343@qq.com
Doi: doi: 10.2340/16501977-2812
Postpartum lumbopelvic pain is common, and there are a range of treatments available. The aim of this study was to establish a programme for use in clinical practice, comprising pelvic floor muscle training combined with other traditional treatments. The programme was shown to reduce pain and improve patients’ quality of life. No adverse events occurred.
Lumbopelvic pain refers to self-reported pain in the lower back, sacroiliac joints, or a combination of these locations, among pregnant and postnatal women (1). The pain may radiate into the posterior thigh and is also experienced in conjunction with, or separately from, symphysis pubis pain. Approximately 50% of pregnant women report lumbopelvic pain to some degree (1). Although the majority of women recover within 3 months of delivery, in a substantial number of women the pain persists, with prevalence ranging from 26.5% to 91.0% 2–3 years after delivery (2). Risk factors for such pain include maternal age, parity, body mass index, education, and uncomfortable working conditions (3). Recent studies indicate the importance of hip extensors, pelvic floor muscle (PFM) and transverse abdominal muscle (TrAM) in the development of lumbopelvic pain (4). Moreover, pelvic instability, asymmetry and insufficient compression of the sacroiliac joints contribute to continuous lumbopelvic pain after delivery (5). Studies have demonstrated the importance of choosing an optimal treatment strategy in clinical practice, and 5 subgroups of self-rated pain locations have been identified in the pelvic area (6). This study focused on pelvic girdle pain (PGP), or PGP in combination with lumbar pain, since these groups have been shown to have the highest impact on activity levels and health-related quality of life (6).
Stabilization exercises that include dynamically controlling the lumbar segments and pelvic joints have been shown to result in functional improvement in patients with lumbopelvic pain (7). Different treatments have been used, including drugs, specific exercises, short-wave therapy, ultrasound, neuromuscular electrical stimulation, corsets, acupuncture and massage (2). The most frequently used interventions are strengthening exercises for the TrAM, PFM training, and a technique involving manipulation of the lumbar multifidus. Although several studies have shown that correct PFM contractions cause co-contractions of the abdominal muscles (8, 9), to date, studies of exercise programmes for treatment of lumbopelvic pain have shown mixed findings and there is insufficient evidence to guide clinical practice in this area. There was also variability across existing randomized controlled trials (RCTs) in the components of programmes, modes of delivery, follow-up times and outcome measures (3, 4, 7). It is therefore not known whether PFM training works well alone, or in combination with other therapies. There is a strong need for the development of a validated postpartum programme.
A common concept in PFM training is the use of standardized exercises or electromyographic activity of the PFM (10). Physical therapists are frequently needed to give instructions on how to contract the PFM correctly at hospital or at home. A new validated myoelectric activation method, using biofeedback registration, was used in the current study (11). This technique can be regarded as an adjuvant electromyography, allowing both patients and physical therapists to observe PFM functioning and assess muscle integrity. This technique has been shown to improve self-reported subjective success and satisfaction in patients with pelvic floor dysfunction (11).
The aim of the current study was to investigate whether a rehabilitation programme focusing on biofeedback-assisted PFM training is sufficient as treatment for women with PGP or combined pain postnatally.
This was a randomized controlled trial with an equal number of participants in each of 2 groups. The study protocol was approved by an ethics committee of Southern Medical University (number RCT02561094). All participants signed a consent form prior to enrollment.
This study was conducted in Lishui County, Foshan, China, situated in the middle of Pearl River Delta, which is one of the most affluent regions in south China. At the end of 2108, the total registered population of Lishui county was approximately 600,000. Patients were recruited from the postpartum rehabilitation unit of Naihai Hospital, Southern Medical University, a 1,000-bed tertiary hospital in Foshan, between January 2018 and June 2019. In 2019, annual delivery in the department of obstetrics was approximately 1,800.
Women were included if they fulfilled the following criteria: (i) diagnosis of PGP or PGP in combination with lumbar pain (combined pain) as defined by the Mechanical Diagnosis and Therapy protocol (MDT) (12); (ii) age between 20 and 35 years; (iii) body mass index (BMI) < 28 kg/m2; (iv) given birth by unmedicated vaginal delivery to a singleton infant after more than 32 weeks of gestation; (v) parity < 4; (vi) 3 months after delivery; (vii) not planning to move away from Lishui County within 3 months of study enrollment.
Exclusion criteria were: (i) previous caesarean section; (ii) epidural analgesia during labour; (iii) systemic locomotor system disease; (iv) verified spinal problems in the previous 2 months; (v) a history of spinal, pelvic, or femur surgery or previous fracture, neoplasm; (vi) psychiatric disorders or other unstable/serious conditions requiring active treatment; (vii) treatment with deep core muscles exercises or PFM training during the previous 3 months; (viii) inability to cooperate with treatment procedures or declined to participate.
The diagnosis of PGP was based on the history of present illness, starting with pain onset during a pregnancy or within 3 weeks after delivery, and ongoing since then. The pain is located distal and/or lateral to the L5–S1 area in the buttocks. It was followed by clinical examination according to the Mechanical Diagnosis and Therapy protocol (MDT) (12) (i.e. active straight-leg raising test, posterior pelvic pain provocation test, compression test, Gaenslen’s test, distraction test, and sacral thrust). A positive score is needed on 2 or more tests for a diagnosis of PGP (12). Lumbar pain was defined based on reproducible pain and/or a change in range of motion from repeated movements or different positions of the lumbar spine or experience of centralization and peripheralization phenomena during examination and fewer than 2 positive pain pelvic pain provocation tests according to the classification of MDT (12). In addition to PGP, some women also had lumbar pain, and were considered to have PGP in combination with lumbar pain (combined pain) (12) and were also included.
All participants underwent a stabilization strengthening programme, which is a routine treatment offered by physical therapists. The programme, including abdominal bracing exercises, side-support exercises, and quadrupled exercises, has been described in detail previously (13). During the first 4 weeks, women were instructed to perform the exercises once a day. After the 4-week period, they were instructed to perform exercises 4 times a week lasting 4 weeks, then 2 times a week until the end of the study (12 weeks’ follow-up). Patients were encouraged to continue training by themselves at home. To ensure compliance with the training programme, phone calls were made at a minimum of 2 times a week and a daily training diary was kept by the therapists during the study period. Subjects also received exercise guidebooks and instruction videos.
The scheduled treatment for the intervention group was 12 weeks, which combined neuromuscular electrical stimulation (NMES) with biofeedback-assisted pelvic floor muscle training (BAPFMT). The combined therapy started on the day following enrollment and performed by a female physical therapist with 5 years of experience. Each subject was scheduled for 4 treatment sessions per week over the first 4-week period, followed by twice and once a week over the second and third 4-week periods, respectively. The sessions lasted 40 min. The BAPFMT consisted of biofeedback and electrical stimulation therapy, lasting 20 min. Before treatment, subjects were required to empty the bladder and lie in a supine position. A disposable probe was inserted into the vagina to record PFM activity and contraction, using a neuromuscular therapy instrument. Using computer graphics, the parameters of the device were determined by ensuring the passive and active contraction of PFM and patient tolerance (14). The parameters of electrical stimulation were set as pulse width of 20–120 μs and low voltage of 20–80 Hz. The therapy was applied according to the protocols described by Miller et al (15).
The NMES was applied bilaterally to the lumbar paraspinal muscles after patients completed BAPFMT. Four rectangular electrodes were used, as described previously (16). The parameters were set a frequency of 80 pulses/min, pulse width of 0.1–0.5 ms and on:off ratio of 4 s:10 s. The intensity was increased until the patients could feel it, but it was not painful. Each patient was scheduled for 4 treatment sessions per week over the first 4-week period, followed by twice and once a week over the second and third 4-week periods, respectively. The session lasted 20 min. For the subjects in the control group, the NMES was administered following the same protocol as applied in the intervention group, but no BAPFMT was administered.
This study involves a 12-week intervention, and all participants were followed up at 6 and 12 weeks. Outcomes were measured by a physiotherapist who was blind to participant enrollment and allocation. The indicators selected focused on the following factors: (i) pain intensity, measured on the triple Numerical Pain Rating Scale (NPRS), an 11-point scale ranging from 0 (no pain) to 10 (maximum pain). Patients were asked to answer 3 questions regarding the intensity of current pain, the best and the worst pain intensity in the past 24 h. The score is based on the mean of the 3 sub-scores (17). (ii) Functional performance, assessed with the Modified Oswestry Disability Questionnaire (MODQ), which includes 10 domains related to back pain. The maximum score within each domain is 5, with a high aggregated score indicating greater levels of disability (18). (iii) Quality of life, determined with the Short Form Health Survey-36 (SF-36). The SF-36 consists of 36 items, which assess the extent of the health-related limitations, both in physical and mental functioning. Previous studies on the Chinese version of the SF-36 have proved its reliability and validity (19).
The sample size was calculated based on SF-36, the primary outcome variable of this study, and repeated measures analysis of variance design, referring to the study of Gutke et al. (4). To achieve 80% power with an effect size of 0.5, a total of 62 participants was required. Estimating a loss-to-follow-up of 15%, 10 more patients would be needed; hence the number of subjects selected for this study was 72.
A total of 96 eligible women were randomly assigned to the intervention group or control group by computerized block randomization, which was concealed from the researcher and participants. The block size was 2, with equal numbers in each group, and opaque sealed envelopes were used to produce a randomization sequence by an administrative person not involved in subject recruitment. The envelope could only be opened by a postgraduate student investigator whenever a potential subject was eligible for random assignment.
Data were analysed using SPSS22.0. Kolmogorov–Smirnov test to examine normality for all outcome variables. Baseline information was analysed by Mann–Whitney U test. Two-way repeated measures analysis of variance was used to examine the differences between the intervention and control groups. A p-value < 0.05 was considered statistically significant.
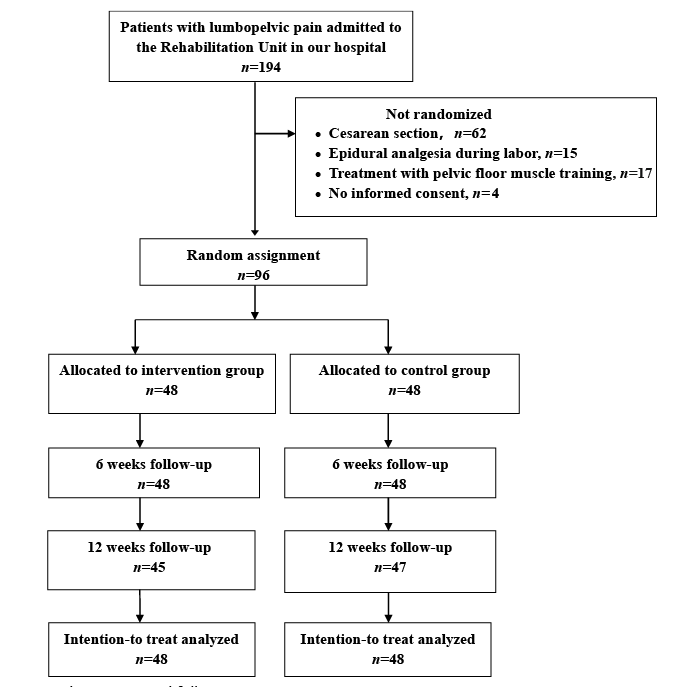
Over the recruitment period from January 2018 and June 2019, 194 women with lumbopelvic pain underwent screening, with 96 meeting the selection criteria (Fig. 1). The main reasons for exclusion were caesarean section (31.9%), followed by epidural analgesia during labour (7.7%) and experience of PFM training during the previous 3 months (8.6%), whereas only 4 women declined to participate. A final total of 96 subjects was included in the study. Subjects were randomly assigned to intervention and control groups in equal numbers (n = 48 in each group). Information was obtained for all subjects at 6 weeks after treatment (0% missing). For outcome measures, 12-week results were obtained for 47 subjects in the control group (2.1% missing) and 45 (6.2% missing) in the intervention group. One individual in the control group was not followed because she had moved out of Lishui County. Data on 3 women in the intervention group were missing due to their reluctance to undergo treatment. All analyses followed the intention-to-treat principle. There were no study-related adverse events.
Fig. 1. Flowchart of patient randomization and follow-up.
Baseline characteristics are shown in Table I. The mean age of participants was 30.8 years. Most were married (91.7%), educated at high school or lower (53.1%), and rarely or never performed heavy lifting at work (94.8%). Mean BMI of participants was 25.9 kg/m2. Most subjects had 2 parities (63.5%). The majority of women (78.1%) did not report lumbopelvic pain during pregnancy. Most did not receive treatment for lumbopelvic pain during pregnancy (93.7%). There were no significant differences between the groups for sociodemographic features, clinical indicators for BMI, parity, onset of pain during pregnancy, or treatment of lumbopelvic pain during pregnancy.
Table I. Baseline demographic profiles and clinical data of patients allocated to the intervention and control groups
The primary outcomes after 6 and 12 weeks are shown in Table II. Triple Numerical Pain Rating Scale (NPRS) score at 12 weeks was significantly better in the intervention group (F = 6.40, p = 0.000) compared with the control group, but with no difference at 6 weeks. There was significant between-groups difference (F = 5.36, p = 0.000). The Modified Oswestry Disability Questionnaire demonstrated significantly better results in the intervention group than in the control group at 6 (F = 8.74, p = 0.009) and 12 (F = 10.81, p = 0.015) weeks. Significant difference was also noted between groups (F = 6.47, p = 0.012). The mean values of Physical Components Summary, an integral part of SF-36, were significantly better in the intervention group at 6 (F = 18.70, p = 0.000) and 12 (F = 15.03, p = 0.000) weeks compared with the control group. Between-group improvement was also significant (F = 6.08, p = 0.000). However, the same trend was not observed in the Mental Components Summary score of the SF-36.
Table II. Comparison of triple NPRS, MODQ and SF-36 by groups over 3 time-points (baseline, 6 weeks and 12 weeks)
To our knowledge, this is one of few RCTs investigating the effect of a rehabilitation programme applying biofeedback-assisted PFM training and specific stability exercises in women with postpartum PGP or combined pain. The main findings of this study suggest that outcomes with regard to pain intensity, functional performance and quality of life were more favourable in the intervention group than in the control group.
The positive outcomes of BAPFMT as an add-on to traditional treatment support the use of PFM training to increase compressive forces in the sacroiliac joints. No adverse events were noted during the treatment sessions. This comprehensive programme with BAPFMT offers a safe, effective conservative management option. Biomechanical and anatomical studies have shown that contraction of the PFM can cause the synergistic co-contraction of the transversely-oriented muscles of the abdominal wall, especially the TrAM (8, 9). The TrAM is the deepest of the lateral abdominal muscles, and is the most suitable muscle to achieve compression of both innominate bones against the sacrum (8). Hence, it has been postulated that efficient contraction of those muscles could reduce movement in the sacroiliac joints and reduce strain on the engaged ligaments in the pelvic ring, resulting in a greater chance of recovery. However, it has been reported in healthy volunteers that the activity of TrAM varies in difference anatomical locations (20). Contraction of the middle part of the TrAM may have an adverse effect on the pelvic girdle due to increased intra-abdominal pressure (20). Some researchers have therefore proposed that, rather than being a single entity, PGP disorders include a number of sub-groups with different underlying pain mechanisms. These authors suggest that only those women with lumbopelvic pain who have a positive active straight-leg raise test would benefit from the exercises that target deep abdominal musculature (4, 7). Nevertheless, in clinical practice for lumbopelvic pain, contraction of the TrAM is emphasized. Although there are many PFM training protocols, no accepted standard exists. The protocol developed for the current study was based on the tenets of exercise physiology. By adding biofeedback to PFM training, neuroplasticity or functional neural regeneration mechanisms of central nervous system is induced (11). This mechanism can help patients control and monitor their future muscle activities and movements, thus improving participant adherence and perceptions of treatment. The literature lacks a clear opinion on the optimum type of biofeedback (i.e. verbal, pressure, electromyography or palpation), to be combined with PFM training. In addition, different kinds of electrodes have been used in BAPFMT studies. In order to develop more uniformity in the treatment of lumbopelvic pain, more RCTs, with the use of uniform equipment, are warranted, in order to make valid comparisons.
The benefits of the postpartum programme in favour of the intervention group in this study can also be attributed to the application of NMES. This is consistent with previous studies on patients with chronic low back pain (21). It seems that NMES can activate the superficial and deep paraspinal muscles, and is therefore effective in decreasing pain and disability. However, a study by Alrwaily et al. contradicts these results (13); an RCT by these authors found that NMES does not add any benefit for patients with chronic back pain when combined with stabilization exercises. This lack of significant difference may be explained by the variation in NMES dosage, the number of sessions per subject, study population and design. In the current study, the higher number of treatment sessions, and supervision by a physical therapist, may be associated with improved clinical outcomes.
Stabilization exercises are the first-line treatment option for lumbopelvic pain after childbirth. The results of the current study support the hypothesis that women with postpartum lumbopelvic pain have load transfer dysfunction in this area (4). In the current study, stabilization training focussed mainly on local muscles, including the TrAM, the lumbar multifidus and the PFM. The training consisted of local segmental control, closed chain segmental control and open chain segmental control, with an emphasis on activities of daily living. Previous studies also suggest the inclusion of exercises for global muscles, as well as local muscles in the treatment strategies for lumbopelvic pain (22). Taking into account the lack of knowledge regarding specific stabilizing exercises, there is a need for further research into the function of stabilizing components.
The current study also found that this rehabilitation programme cannot significantly improve MCS in postpartum lumbopelvic pain. It is possible that the programme does not provide sufficient psychological support for subjects to reach optimal outcomes. The lack of positive change in mental health may be attributed to, but not limited to, factors such as postpartum anxiety and depression, low self-efficacy, high pain intensity, and long duration of symptoms. This study indicates that postpartum lumbopelvic pain is a complex phenomenon, and that a more specific treatment regimen for better management of physical symptoms, as well as psychological support, is needed.
Study limitations
This study has several limitations. First, only women who had had vaginal deliveries were included, which may which may limit the generalization of the results to the general population. Secondly, although all subjects were contacted to encourage them to perform exercises at home after the initial 4-week period, the quality of their training was not assessed (i.e. how many times and how assiduously each woman performed the exercises). Thirdly, the programme lasts 3 months and is time-consuming.
Conclusion
This study found that a postpartum programme, focusing on biofeedback-assisted PFM training, for women with lumbopelvic pain was feasible and resulted in an improved physical domain of quality of life.
The authors would like to thank all the patients who took part in this research, and the staff at the centre, who facilitated this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize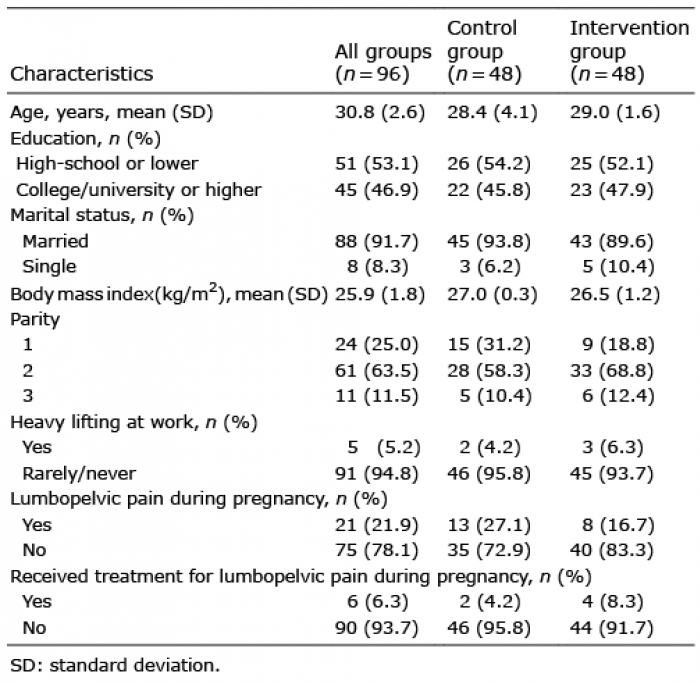 Click to show fullsize
Click to show fullsize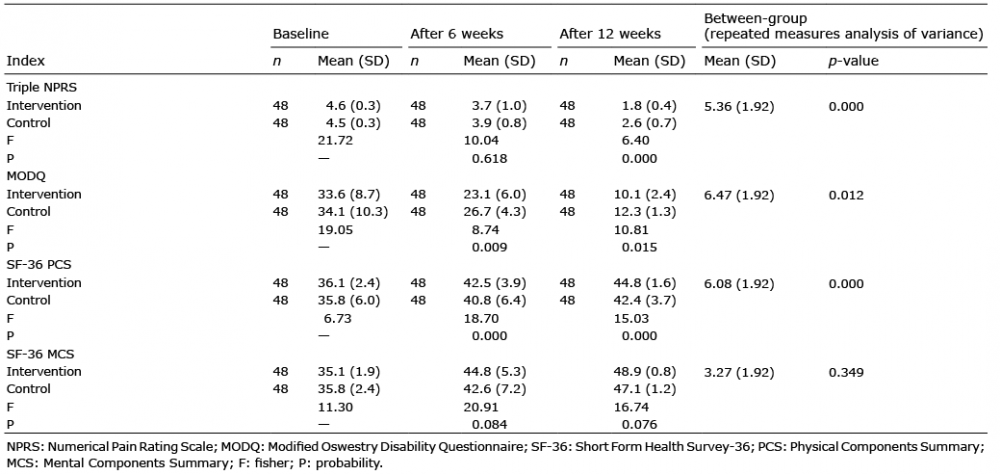 Click to show fullsize
Click to show fullsize