
From the 1Department of Rehabilitation Medicine and 2Department of Gastroenterology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China. *These authors contributed equally to this work.
Objective: To investigate the effectiveness of robot-assisted therapy on balance function in stroke survivors.
Data sources: PubMed, the Cochrane Library, Embase and China National Knowledge Infrastructure databases were searched systematically for relevant studies.
Study selection: Randomized controlled trials reporting robot-assisted therapy on balance function in patients after stroke were included.
Data extraction: Information on study characteristics, demographics, interventions strategies and outcome measures were extracted by 2 reviewers.
Data synthesis: A total of 19 randomized trials fulfilled the inclusion criteria and 13 out of 19 were included in the meta-analysis. Analysis revealed that robot-assisted therapy significantly improved balance function assessed by berg balance scale (weighted mean difference (WMD) 3.58, 95% confidence interval (95% CI) 1.89–5.28, p < 0.001) compared with conventional therapy. Secondary analysis indicated that there was a significant difference in balance recovery between the conventional therapy and robot-assisted therapy groups in the acute/subacute stages of stroke (WMD 5.40, 95% CI 3.94–6.86, p < 0.001), while it was not significant in the chronic stages. With exoskeleton devices, the balance recovery in robot-assisted therapy groups was significantly better than in the conventional therapy groups (WMD 3.73, 95% CI 1.83–5.63, p < 0.001). Analysis further revealed that a total training time of more than 10 h can significantly improve balance function (WMD 4.53, 95% CI 2.31–6.75, p < 0.001). No publication bias or small study effects were observed according to the Cochrane Collaboration tool.
Conclusion: These results suggest that robot-assisted therapy is an effective intervention for improving balance function in stroke survivors.
Key words: robot-assisted therapy; stroke; balance function; Berg Balance Scale; meta-analysis.
Accepted Feb 26, 2021; Epub ahead of print Mar 19, 2021
J Rehabil Med 2021; 53: jrm00174
Correspondence address: Xiao Lu, Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, 210029, China. E-mail: luxiao1972@163.com
Doi: 10.2340/16501977-2815
Balance is an important factor in ability to perform independent walking. Many patients with stroke gain little benefit from neural rehabilitation because their balance control is impaired. Robot-assisted therapy is a promising intervention approach, which has developed rapidly in recent years. Several previous reviews have focused on gait-related measurements, such as walking speed and endurance; however, the effectiveness of robot-assisted therapy on balance has not been clearly outlined. This systematic review and meta-analysis showed that robot-assisted therapy can significantly improve balance recovery compared with conventional therapy, especially for people in the acute/subacute phase after stroke treated with an exoskeleton and a total training time of more than 10 h.
Globally, stroke is the second cause of death and one of the most common causes of disability. Although the total incidence of stroke is decreasing in most regions worldwide, the number of disability adjusted life years is increasing, indicating that the overall burden of stroke is increasingly high (1).
Balance function is the ability of a person to maintain their centre of gravity within their base of support with minimal postural sway (2). Balance impairments are common in patients with stroke due to impaired integration of multiple sensorimotor information, postural control, and muscle strength (3). The current evidence indicates that balance is an important factor in ability to perform independent walking, and it is a significant predictive factor for gait function (4). Due to the nature of walking, the majority of the gait cycle is spent in single-limb support. During this phase, the person’s centre of gravity moves outside the base of support, making the balance inherently unstable (5). Stroke patients may have uneven weight distribution during standing and walking, and therefore are more likely to fall (6). Thus, to improve balance function is one of the main goals in a majority of stroke survivors (7).
Robot-assisted therapy (RT) is a promising intervention, which has recently expanded rapidly. RT has the potential to provide automatic and repetitive training that could enhance functional restitution and motor control for stroke patients; it can also reduce the manual burden during rehabilitation (8). Previous studies have assessed the effectiveness of RT on motor function in stroke patients. Nam et al. reported that RT could improve muscle strength of the lower limb (9). Another study noted that RT had a significant effect on improving motor control and muscle strength (10). Although balance function is essential to the readiness for walking training, to date, only a few reviews have focused on this item (11). During their recovery, treatment effects may vary according to time since stroke onset. It has been reported that acute stroke may benefit from RT, but those in the chronic phase may not (12). On the other hand, with regard to the effectiveness of RT, the device type is of major concern. Generally, robot-assisted devices can be divided into exoskeleton and end-effector. Exoskeleton devices consist of programmable drives or passive elements, which flex the hips and knees during the swing phase. Feet are placed on the foot plates in the end-effector design, and the device works to simulate the stance and swing phases (13). Training intensity may also affect the outcome of stroke.
The aims of this study were to assess the effects of RT for improving balance function after stroke, in comparison with conventional therapy, and to investigate the potential impacts of recovery stage, device type and training intensity on stroke prognosis.
A systematic review and meta-analysis were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (14). The protocol was previously registered at PROSPERO (registration number CRD42018115589).
Search strategy and selection criteria
An electronic search of the published literature was conducted in PubMed, the Cochrane Library, Embase and China National Knowledge Infrastructure databases. Studies were collected from inception up to 17 January 2020. Indexing terms and free-text words of the following key terms and synonyms were used: (Participants) “stroke”; (Intervention) “robot-assisted therapy; (Outcome) “gait” or “balance”; (Study design) “RCT”. A detailed search strategy used in PubMed is shown in Appendix SI. In addition, manual searching was performed to identify the relevant references in these articles.
Studies were selected based on the following inclusion criteria: (i) patients had been diagnosed with cerebral vascular accident; (ii) robot-assisted training was aimed to the recovery of balance function; (iii) control group received conventional therapy (e.g. regular physical therapy, manually-assisted body-weight supported treadmill training, etc.); (iv) RCTs were dose-matched trials in which the experimental and control groups spent an equal amount of time on exercise therapy. Studies were excluded if: (i) they compared the effects of 2 different types of robot; (ii) they were trials in which RT was combined with other treatments (e.g. functional electrostimulation); (iii) they were case reports and pre-post design studies.
Data extraction
Two researchers (LW and XTZ) independently extracted the following information from individual studies: authors; publication year; country of origin; participant characteristics; method of randomization; blinding; intervention information; outcome measures; and adverse events. Data on intervention regimens, including device type, training time, frequency and duration, were extracted. Outcome measures were extracted, including one of the following tests: Berg Balance Scale (BBS), Timed Up-and-Go (TUG), Tinetti balance scale, Trunk Impairment Scale (TIS), postural sway tests and specific balance parameters using equipment sensors, such as force plates, accelerometers, and gyroscopes. If the trials had more than 2 groups and permitted multiple comparisons, only the data of interest were extracted.
Risk of bias assessment
Risk of bias for the included trials was assessed independently by 2 reviewers (LW and XTZ) according to the Cochrane Collaboration tools (15). These tools evaluate the selection, performance, detection, attrition, and reporting bias with 7 items. There are 3 evaluation options for each item: low, unclear, and high risk, based on the original research. Disputes and disagreements were solved by discussion or referral to a third reviewer (YZ).
Data analysis
As the selected RCTs used different robotic devices, methodology, and subscales of outcome measures, the treatment effect of the intervention was estimated by pooling the weighted mean difference (WMD) with 95% confidence interval (95% CI). In assessing heterogeneity among studies, the Cochran’s Q and I2 statistics were used. I2 values represent the amount of total variation explained by variation among studies, with a value of greater than 50% indicating severe heterogeneity (16).
The primary analysis was performed to explore the efficacy of RT on balance function reflected with BBS immediately after the intervention. Secondary analysis was conducted in a subset of patients according to: (i) recovery stage (acute/subacute < 6 months or chronic > 6 months); (ii) device type (end-effector or exoskeleton); and (iii) training intensity (total time < 10 or ≥ 10 h). The training intensity was presented using total time (number of sessions × time per session, in h) (17). This cut-off because was arbitrarily applied it was the most frequently used point in the included studies.
Publication bias was assessed by using funnel plots and the Egger linear regression test, with p-values less than 0.1 indicating potential publication bias. All statistical analyses were performed using RevMan 5.2 (The Cochrane Collaboration/The Nordic Cochrane Centre, Copenhagen, Denmark) and Stata12.0 (StataCorp, College Station, TX, USA).
Literature search and study characteristics
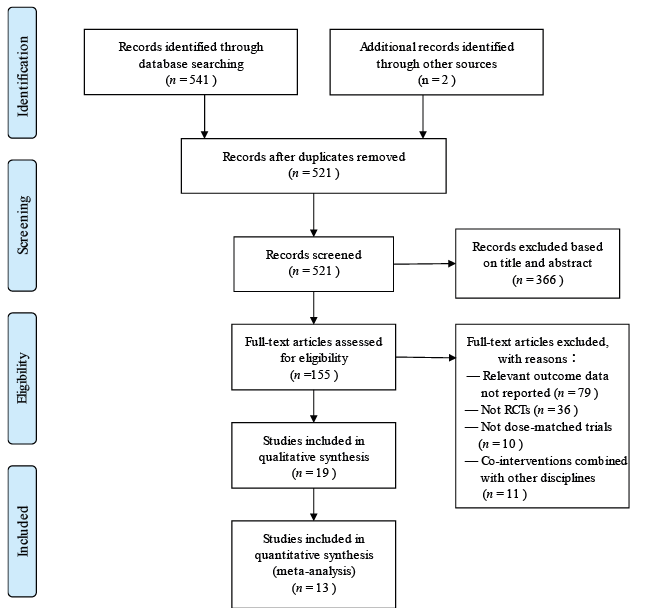
Fig. 1 summarizes the trial selection procedure. After searching the electronic databases, 521 unique records were screened, of which 155 titles and abstracts were considered to be relevant for further screening. After checking the full-text according to the inclusion and exclusion criteria, 19 RCTs were included in qualitative synthesis and 13 RCTs were included in quantitative synthesis. Out of 19 studies 17 were published in English and 2 in Chinese (17, 23). Table I shows the characteristics of included trials. The duration of the intervention ranged from 2 weeks to 5 months, with the training frequency varied from 1 to 6 days. The time spent per session of intervention ranged from 20 min to 1 h and the total time of intervention ranged from 6 to 20 h. In the included studies, Lokomat (Hocoma AG, Zurich, Switzerland), Exowalk (HMH Co. Ltd., South Korea), Walkbot ((P&S Mechanics, Seoul, South Korea)) and Flexbot-B (Jinghe robot Co. Ltd., Shanghai, China) were documented as exoskeleton and G-EO system (Reha Technology, Olten, Switzerland), Morning Walk (Hyundai Heavy Industries and Taeha Mechatronics, South Korea) and Gait Trainer (Reha-Stim, Berlin, Germany) were end-effector robots.Quality assessment
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for trial inclusion and exclusion. RCT: randomized controlled trial.
Table I. Characteristics of selected randomized controlled trials
Quality assessment
Figs 2 and 3 demonstrate the overview of risk of bias for included trials according to the Cochrane Collaboration tools. Bias regarding randomization procedure was unclear in 3 studies, and allocation concealment was unclear in 7 studies. Bias of performance was high, because therapists who supervised training and subjects can hardly be masked to the group allocation. In addition, all studies showed low risk of attribution bias and reporting bias, but were unclear for other bias. Overall quality assessment indicated that all included studies had low or moderate risk of bias.
Fig. 2. Risk of bias graph for all included studies.
Fig. 3. Risk of bias summary: review authors’ judgements about each risk of bias item for each included study
Effects of robot-assisted training on balance
As shown in Fig. 4, 517 participants from 13 studies were included, RT significantly improved balance function compared with conventional therapy (WMD 3.58, 95% CI 1.89–5.28, p < 0.001) with no significant heterogeneity (I2 = 41%, p = 0.06). The other 6 studies were analysed qualitatively. Three reported that no significant difference in balance recovery was detected between RT and CT, although longitudinal significant improvement in balance function was observed (33–35).
In comparing the effectiveness of RT vs CT, 3 factors may affect the outcome of interest, including recovery stage (acute, subacute or chronic), device type (end-effector or exoskeleton), and training intensity (total time ≥ 10 or < 10 h). Fig. 5 shows that RT achieved significantly greater improvement in BBS than CT during the acute/subacute stage of stroke recovery (WMD 5.40, 95% CI 3.94–6.86, p < 0.001). In contrast, no significant results supported that RT was more effective than CT in chronic patients (WMD 1.61, 95% CI –0.02–3.25, p = 0.05). In addition, there were 128 participants in 3 end-effector robot trials, and 389 participants in 10 exoskeleton robot trials (Fig. 6). With the exoskeleton the balance recovery in the RT groups was significantly better than in the CT groups (p < 0.001). However, in the end-effector subset, the improvement in the RT group was not statistically significant compared with that in the CT group (p = 0.18). In addition, Fig. 7 demonstrated that there was a statistically significant difference between RT and CT in the subset with total time ≥ 10 h (WMD 4.53, 95% CI 2.31–6.75, p = 0.12); however, when the total time was less than 10 h no significant differences were detected.
Fig. 4. Comparison of RT vs CT on BBS. 95% CI: 95% confidence interval; SD: standard deviation; IV: inverse variance; RT: robot-assisted therapy.
Fig. 5. Secondary meta-analysis of RT vs CT on BBS by recovery stage. 95% CI: 95% confidence interval; SD: standard deviation; IV: inverse variance; RT: robot-assisted therapy.
Fig. 6. Secondary meta-analysis of RT vs CT on BBS by device type. 95% CI: 95% confidence interval; SD: standard deviation; IV: inverse variance; RT: robot-assisted therapy.
Fig. 7. Secondary meta-analysis of RT vs CT on BBS by training intensity. 95% CI: 95% confidence interval; SD: standard deviation; IV: inverse variance; RT: robot-assisted therapy.
Safety of robot-assisted training
With the exception of 2 studies, all trials reported that there were no adverse events observed during and/or after the interventions. Hornby et al. reported that 2 patients discontinued due to leg pain, 1 patient experienced pitting oedema in the RT group, 4 patients discontinued due to leg pain, 1 patient presented with significant hypertension, and 2 patients withdrew due to subjective exercise intolerance in the control group (22). Maple et al. reported that 1 patient admitted to an acute-care hospital, and another patient experienced a deteriorating medical condition in the control group, no adverse events observed in the RT group (26).
Publication bias
There was no significant funnel plot asymmetry detected, and the Egger test also indicated no evidence of publication bias (p = 0.57). Funnel plots of meta-analysis are demonstrated in Fig. 8.
Fig. 8. Funnel plot of meta-analysis. SE: standard error; MD: mean difference.
This systematic review and meta-analysis included 19 studies comparing the efficacy of RT on balance function after stroke, in comparison with CT. Despite the heterogeneity of the included studies, RT showed superior effects to CT on balance recovery.
BBS is a static-dynamic integrated test used as a representative method for evaluating the balance ability of stroke patients. BBS evaluates a total of 14 functional tasks, yielding a maximum score of 56. A higher score represents a better balance performance (2). RT provides not only simple and repetitive movement, but also generates more complex, controlled multisensory stimulation, which is regarded as essential to balance recovery (36). In addition, RT could make stroke patients experience early verticality, and by gradually increasing weight-bearing, the patients could start standing and standing balance training as soon as possible. Another advantage of RT is that it reduces energy consumption and cardiorespiratory load, and stroke patients can tolerate longer training time and greater training intensity (37). The current results are consistent with several other reviews, showing that RT can significantly increase BBS score after a period of training. Heterogeneity of the current results cannot be ruled out, due the diversity of target population, device type or training protocol.
Brain plasticity is defined as the intrinsic ability of the brain to reorganize its function and structure in response to stimuli and injuries. It is widely recognized that neural plasticity is more likely to happen during the early stage of stroke (38). The plasticity process is initiated in an attempt to compensate for the lesion itself and its remote effects. Changed neural activity and connectivity, in terms of function and structure, could be detected in the perilesional and remote regions (39). The current study found that stroke patients treated with RT showed better outcomes of balance function in acute/subacute phase (< 6 months). The mechanisms above may benefit patients from RT at the early stage, while the correlation and interaction between the central network and the functional recovery need to be further investigated.
Subgroup analysis showed that RT presented better balance function in the exoskeleton subset. According to the device design, the structure of the exoskeleton resembles a human limb, as robot joint axis matches the joint axis of the lower limb. These devices are designed to operate side by side with the human lower limb, and are therefore attached to the lower limb at multiple locations. These systems are suitable for the early-stage patients, as they do not require significant motor ability. On the other hand, the end-effector device facilitates the gait by propulsion of footplates, which may aid movement of the feet and legs in a symmetrical manner. The joints of the end effector are not designed to match the human body. Therefore, these devices cannot perform segmental control of the lower limbs (40). For this reason, it is assumed that end-effector systems may be more suitable for patients with residual motor skills sufficient to control their movement (41). In the current study, only 3 RCTs investigated the effectiveness of an end-effector device, while 10 RCTs focused on exoskeletons. The limited sample size may conceal the real efficacy of interventions.
It was also not clear whether the observed differences between experimental and control groups may be impacted by the training intensity. The pooled results indicated that a total time of ≥ 10 h could improve balance function in the RT group. Time devoted to therapy is a rough estimation of training intensity and provided no clue for the actual amount and type of intervention (42). For instance, a 30-min training session could be either low- or high-intensity. Larger controlled trials are required to investigate the optimal frequency, intensity and duration of RT.
Study limitations
The current study has several limitations. Firstly, due to the limited sample size in individual trials, the pooled results of the current meta-analysis are different from previous ones. Therefore, multi-centre RCTs with larger sample size are warranted to clarify the effectiveness of RT. Secondly, timing of assessment may play a role in the data synthesis and it varied across individual studies. In the current study, 5 trials reported longitudinal results. Three trials performed follow-up at 1-month and other 2 at 6 months. Interestingly, 4-week follow-up demonstrated significant improvement in 2 out of 3 trials (24, 29) while another trial followed up at 4 weeks and those at 6 months did not (20, 22, 26). It is assumed that the efficacy of RT may wane with time.
It is suggested that future studies adopt longitudinal design to explore the role of timing of assessment, which may provide significant insight to training protocol modification. Last, but not least, relevant studies might be missed due to language barriers, which may have led to an incomplete synthesis of data, in particular, advanced robotics were developed in non-English countries, such as Japan and Germany.
Conclusion
This meta-analysis showed that the use of RT has positive effects on balance function compared with CT, especially for subjects in the acute/subacute phase after stroke, treated with exoskeleton and a total training time of more than 10 h. Robotics may compensate part of therapists’ workload and carry out accurate and objective monitoring of motion parameters, providing real-time feedback. RT may therefore be considered a promising intervention for improving balance function in stroke survivors. When combining these results into clinical practice, it should be cautious because of the limited sample included in the current meta-analysis. Future studies that are well-designed and large scale are required to further verify the effectiveness of RT for balance and to determine the optimal RT protocol.
Funding. This work was funded by the National Key R&D Program of China (grant number 2017YFB1303200) and the Nanjing Municipal Science and Technology Bureau (grant number 2019060002). The funding bodies had no role in the study design, data collection, analysis, or the interpretation of data.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize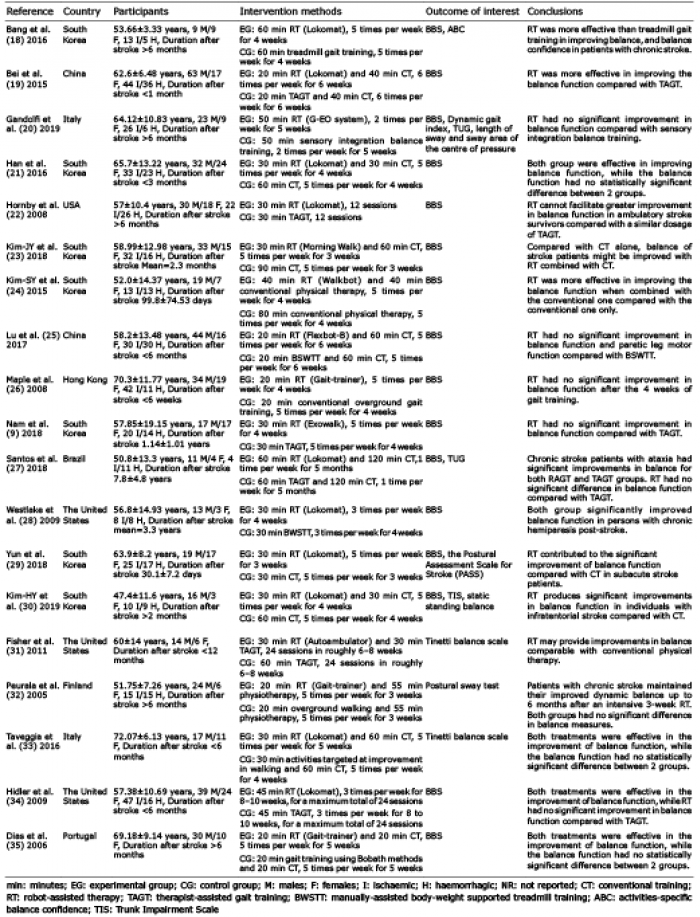 Click to show fullsize
Click to show fullsize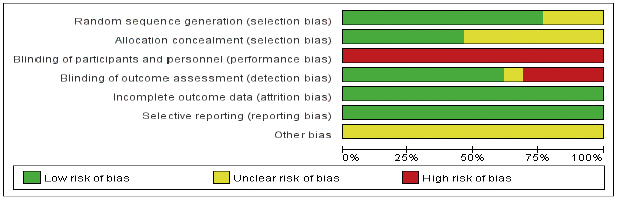 Click to show fullsize
Click to show fullsize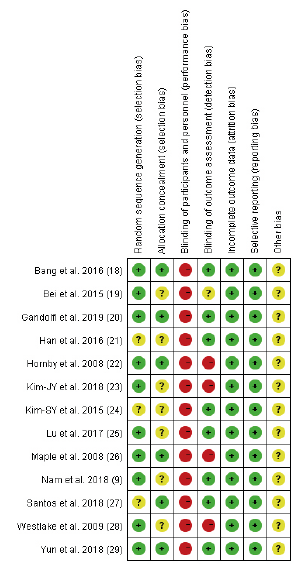 Click to show fullsize
Click to show fullsize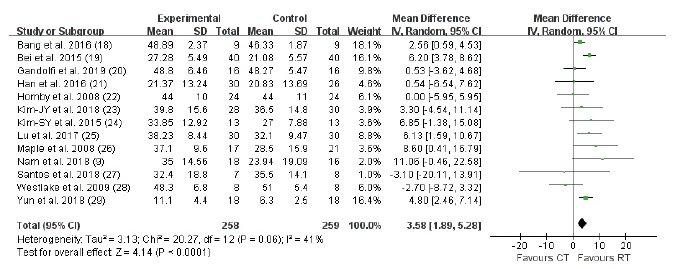 Click to show fullsize
Click to show fullsize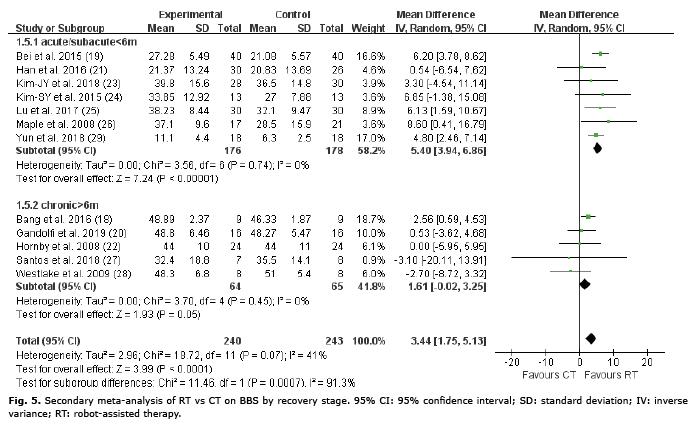 Click to show fullsize
Click to show fullsize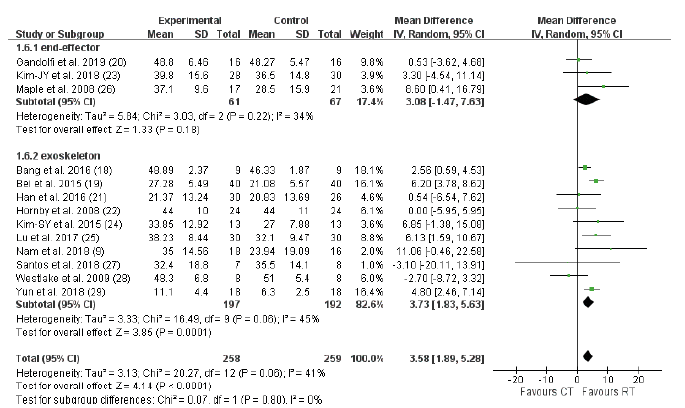 Click to show fullsize
Click to show fullsize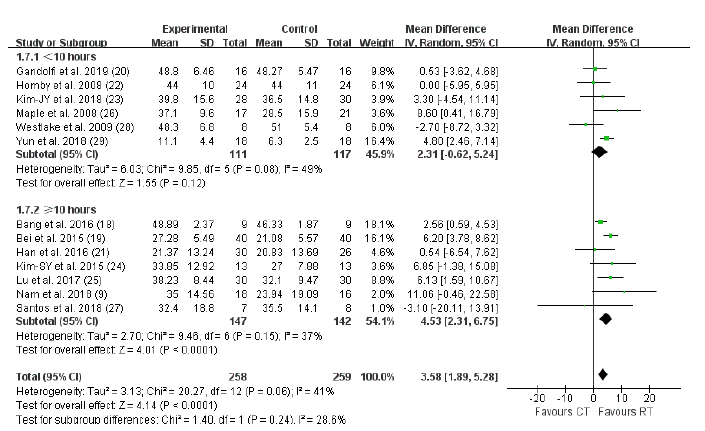 Click to show fullsize
Click to show fullsize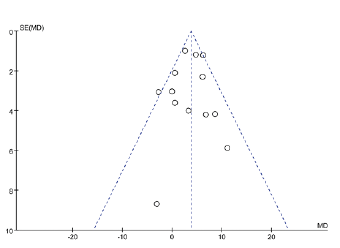 Click to show fullsize
Click to show fullsize