
From the 1Sensation and Perception Research Group, GIGA Consciousness, University of Liège, GIGA CHU- B34 Quartier Hôpital Avenue de l’Hôpital, 11, 2Cognitive Ergonomy and Work Intervention Department, University of Liège, Quartier Agora – Place des Orateurs, 2 B32, 3Interdisciplinary Algology Department, Hospital University of Liège, Domaine Universitaire du Sart Tilman; B35, and 4Public Health Department, Biostatistics, University of Liège, CHU (B35), Quartier Hôpital – Avenue de l’Hôpital, 11 and 5Musicothérapie and Counselling, Liège, www.music-therapy.be, Liège, Belgium
Objective: To identify profiles of patients who are at risk of dropping out from biopsychosocial approaches to chronic pain management.
Patients: A total of 575 patients were included in the study. Of these, 203 were randomized into 4 treatment groups: self-hypnosis/self-care; music/self- care; self-care; and psychoeducation/cognitive behavioural therapy. The remaining 372 patients were not randomized, as they presented with the demand to learn self-hypnosis/self-care, and therefore were termed a “self-hypnosis/self-care demanders” group.
Methods: Socio-demographics and behavioural data were included in the analyses. Univariates analyses, comparing early drop-outs (never attended treatment), late drop-outs (6/9 sessions’ treatment) and continuers were conducted in order to select variables to include in a multivariate logistic regression.
Results: Univariate analyses yielded 8 variables, out of 18 potential predictors for drop-out, which were eligible for inclusion in the multivariate logistic regression. The model showed that having an intermediate or high educational level protects against dropping out early or late in the pain management process. Having to wait for more than 4 months before starting the treatment increases the risk of never starting it. Being randomized increases the risk of never starting the treatment.
Conclusion: In a context in which randomization is considered a “gold standard” in evidence-based practice, these results indicate that this very principle could be deleterious to pain management in patients with chronic pain.
Key words: chronic pain; non-pharmacological treatment; randomization; drop-out; loss to follow-up; attrition.
Accepted Mar 16, 2021; Epub ahead of print Apr 8, 2021
J Rehabil Med 2021; 53: jrm00185
Correspondence address: Aminata Bicego, Sensation and Perception Research Group, GIGA, Consciousness, University of Liège, GIGA CHU- B34 Quartier Hôpital Avenue de l’Hôpital, 11, 4000 Liège, Belgium. E-mail: abicego@uliege.be; and Audrey Vanhaudenhuyse, Interdisciplinary Algology Department, University Hospital of Liege, Domaine Universitaire du Sart Tilman; B35, 4000 Liège, Belgium and Sensation and Perception Research Group, GIGA Consciousness, University of Liège, GIGA CHU- B34 Quartier Hôpital Avenue de l’Hôpital, 11, 4000 Liège, Belgium. E-mail: avanhaudenhuyse@chuliege.be
Doi: 10.2340/16501977-2824
The aim of this study was to identify profiles of patients who are at risk of dropping out from biopsychosocial approaches to chronic pain management. A total of 575 patients were included in the study. Of these, 203 patients were randomized into 4 treatment groups: self-hypnosis/self-care; music/self-care; self-care; psychoeducation/cognitive behavioural therapy. The remaining 372 patients were not randomized, as they presented with the demand to learn self-hypnosis/self-care, and hence formed a “self-hypnosis/self-care demanders” group. Analyses of socio-demographics and behavioural data were conducted, comparing early drop-outs (never attended treatment), late drop-outs (6/9 sessions’ treatment) and continuers. Results showed that having an intermediate or high educational level protects against dropping out early or late in the management process. Having to wait for more than 4 months before starting the treatment, and being randomized, increases the risk of never starting it. Thus, in a context in which randomization is considered as a “gold standard” in evidence-based practice, these results indicate that this very principle could be deleterious to pain management in patients with chronic pain.
Chronic pain is a complex disorder in which pain appears persistent and prolonged (> 3 months) and includes biological, psychological and socio-professional factors that undermine patients’ everyday life. Patients and healthcare providers are increasingly turning to non-pharmacological treatments, such as hypnosis and music therapy, combined with cognitive behavioural therapy (CBT) (1). The efficacy of these treatment in managing chronic pain has been demonstrated (2–4).
A major problem in clinical research is drop-out, which ranges from 5% to 46%, in chronic pain management, depending on the study (5). The first issue concerns the definition of drop-out, since this varies between authors: some regard drop-out as patients ending therapy before the agreed-end-of-treatment (6), others consider it as not attending therapy sessions even though patients have agreed to attend (7). The second issue is that few clinical studies in the field of chronic pain take drop-out into account, thus generating a bias in the overall results of clinical trials investigating the efficacy of such treatments (8). The lack of studies and the disagreement regarding definitions lead to a range of results in the study of drop-out predictors in chronic pain. Some authors have highlighted that a low educational level increases the risk of dropping out from therapy (cohort study (9)), while others have shown the contrary (randomized trial (10)). The same controversy can be seen when considering age, sex and personality (systematic review (5); randomized trial (10); retrospective study (11); non-randomized trial (12)). Predictors outside of patient-related factors have mostly been studied in the mental health literature. As the management of chronic pain and mental health is relatively similar, consideration of these factors seems relevant. A meta-analysis showed that, in psychotherapy settings, the therapist expertise had an influence on drop-out. The results demonstrated that when trainees (pre-degree attainment) lead the group therapy, patients tended to be more likely to drop-out (13). Another meta-analysis showed that patients’ motivational level predicted drop-out from psychotherapy (14). A further barrier to completing treatments is the waiting period between initial contact and the effective start of the treatment (retrospective study (15)). Another retrospective study highlighted that the longer the patients in a substance abuse treatment programme had to wait until the onset of treatment (≥8 days), the more likely they were not to attend the first session of the programme (16).
Given the lack of consensus, a better understanding of the profile of drop-outs and contextual risk factors, is essential in order to prevent this phenomenon, enhance treatment adherence and, consequently, ameliorate the study of treatment efficacy in chronic pain.
The aim of this study was to retrospectively identify patient- and context-related factors to explain drop-out from randomized biopsychosocial-based treatment programmes.
Population
A total of 607 patients with chronic pain who spontaneously attended the Interdisciplinary Algology Department of the University Hospital of Liège, Belgium, from March 2015 until December 2017, were recruited to the study. A final total of 575 patients were included in the study (7 patients were not interested in the study, 23 did not complete the T1 questionnaires, one had other health issues, and one could not attend therapy due to organizational issues). Inclusion criteria were: patients at least 18 years old; fluent in French; and a diagnosis of chronic pain. Exclusion criteria were: psychiatric disorders (schizophrenia, psychosis, borderline with prolonged dissociation episode); drug addiction; and alcoholism. A proportion of patients were randomized into 4 treatment groups: psychoeducation/cognitive behavioural therapy (CBT), self-care, self-hypnosis combined with self-care; and specifically composed music combined with self-care. Other patients presented with the specific demand to learn self-hypnosis/self-care, and thus were not randomized; they were included in a “self-hypnosis/self-care demanders group”. Drop-out was divided into 2 categories: “early drop-outs”: patients who agreed to participate, but never attended the treatment groups; and “late drop-outs”: patients who attended fewer than 6 sessions out of 9. Continuers were patients who completed the treatment programme.
The study was approved by the ethics committee of the Medical School of the University of Liège. All participants provided written informed consent to participate in the study.
Design
This study is part of a randomized clinical trial, registered retrospectively on ClinicalTrials.gov (NCT04218227) on the 1 March 2020.
Treatment groups
The treatments have been described previously by Vanhaudenhuyse et al. (2). Each of the 4 treatment groups included 8 patients, and each treatment comprised 7 sessions (1 per month) of 2 h and 2 follow-up sessions.
Psychoeducation/CBT group. This treatment group was run by 2 psychologists (NM and IS), and comprised group discussions, aimed at enhancing the patients’ autonomy, informing them and empowering them to become more active in their treatment. The psychologists gave a presentation on problems underlying chronic pain, on the biopsychosocial approach and the benefit of patients’ empowerment. Sessions included discussions on themes such as: specificities of chronic pain, psychological factors linked to it, attitudes and beliefs, and suggestions for coping with chronic pain.
Self-care group. This treatment group was run by 3 psychologists (NM, IS and AV) and an algologist (M-EF), and was based on CBT. The principle was to teach patients to take care of themselves in their everyday life through concrete tasks. The objectives were to empower the patients and to reactivate and amplify their awareness of the positive experiences they encountered every day. All of the proposed tasks focused on the patient’s general well-being rather than on pain. Patients were asked to keep a daily journal in which they had to write down the tasks performed and their observations from each task. Each session began with a discussion of the tasks prescribed and completed.
Self-hypnosis/self-care group. This treatment group was run by psychologists (NM, IS, AV) and an algologist (M-EF), all of whom were specialized in clinical hypnosis. Self-care learning was the same as described above. At the end of each session, a 20-min hypnosis exercise was conducted. All patients were given compact discs (CDs) containing the hypnosis exercise from the session, and were invited to perform the exercise on a daily basis. Six different exercises were proposed to patients, plus 2 more during the follow-up period. The first session was an introduction to hypnosis, and no exercise was realized. The first exercise included suggestions about relaxation, positive body sensations and invitation to observe a sunrise and a beautiful landscape, while relaxing in a white cloud chair. The second exercise was a safe place suggestions-based hypnotic script. The third exercise was centred on healing sleep suggestions. The 2 subsequent exercises were centred on analgesia suggestions. The final exercise was centred on hand analgesia suggestions. The 2 follow-up exercises were centred on lightness sensations and the metaphorical creation of a problem encountered in the patient’s life. All exercises were created by one of the co-authors (M-EF). The goal of listening to the CDs was to help the patients to self-induce hypnosis.
Specially composed music/self-care group. This treatment group was run by psychologists (NM, IS, and AV) and an algologist (M-EF). The aim and the procedure were the same as in the “self-hypnosis/self-care” group above, except no hypnosis exercise was given. Instead, at the end of each session, patients were invited to listen to a specially composed melody for 20 min. Six CDs were given to each patient and they were asked to listen to them on a daily basis, 2 more CDs were given during follow-up sessions. The music was composed and recorded by one co-author, who is specialized in music therapy (AC).
Self-hypnosis/self-care demanders group. Finally, the “self-hypnosis/self-care demanders” group received the same intervention as the self-hypnosis/self-care group.
Data collection
Baseline data collection was performed based on the Initiative in Methods, Measurements and Pain Assessment in Clinical Trials (IMMPACT) recommendations (17):
There is no total score, but a specific score for each subscale; the higher the score, the more the patient endorses the belief.
French validation was used for all questionnaires except the SOPA-35.
Statistical analyses
Qualitative variables are represented as count and percentage. Quantitative variables with a normal distribution are represented as mean and standard deviation (SD), and as median and interquartile range (Q1–Q3) when symmetrical distribution is not fulfilled. The normality of the quantitative variable was investigated graphically and numerically. Univariate analyses were performed to compare variables between continuers and drop-out groups: χ2 test for categorical variables and one-way analysis of variance (ANOVA) or its non-parametric equivalent Kruskal–Wallis test for quantitative variables. Significant variables in univariate case were included in a multivariate logistic regression to produce a profile of patients at risk of dropping out. The dependent variable was the drop-out factor and the continuers were taken as the referential category. Two-tailed p-values < 0.05 were considered to be statistically significant. The acquired data were processed using statistical data processing software R 3.6.0 (26).
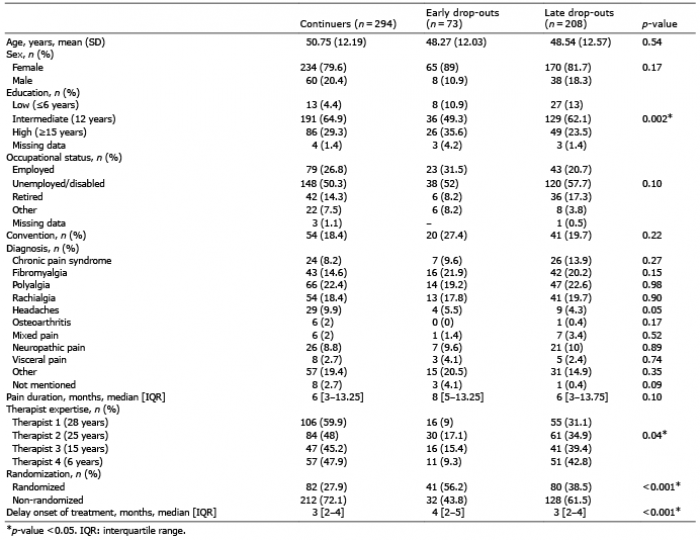
A total of 575 patients were included in this study. Of these, 281 (48.8%) were classified as drop-outs and 294 (51.2%) as continuers. In the drop-out group (n=281), 73 (26%) patients were considered “early drop-outs” as they had agreed to start treatments, but never attended to the sessions; and 208 (74%) were considered “late drop-outs” as they attended fewer than 6 sessions out of 9. There were no statistical differences in age, sex, occupational status, convention and aetiologies (Table I). Significant differences were found in educational levels: 4.5% of the continuers had a low educational level vs 10.9% for the early drop-outs and 13% for the late drop-outs (p = 0.002). The therapist’s expertise was significantly different: patients tended to continue according to the therapist’s expertise (therapist one was considered to have the most expertise, while therapists 2, 3 and 4 had less expertise): therapist one (28 years of group expertise) had 59.9% of continuers, 9% of early drop-outs and 31.1% of late drop-outs; therapist 2 (25 years of group expertise) had 45.2% of continuers, 15.4% of early drop-outs and 39.4% of late drop-outs. Therapist 3 (15 years of expertise) had 48% of continuers, 17.1% of early drop-outs and 34.9% of late drop-outs; therapist 4 (6 years of expertise) had 47.9% of continuers, 9.3% of early drop-outs and 42.8% of late drop-outs (p = 0.04). Randomization had an effect on the proportion of drop-outs: in the non-randomized group 72.1% were continuers vs 19.7% continuers in the randomized group (p < 0.001). The delay in onset of treatment was significantly different across groups: 2.94 (1.76) months for continuers, 4.08 (2.15) for early drop-outs and 3.14 (2) for late drop-outs (p < 0.001).
Table I. Characteristics of continuers and drop-outs in a chronic pain treatment programme. Early drop-outs: patients who never started the treatments; late drop-outs: patients who attended to < 6 sessions out of 9; continuers: patients who completed the treatments
Univariate analyses for behavioural variables
No statistical differences between continuers and all types of drop-outs were found for pain intensity, the subscale depression of the HADS, ISI, PDI, CHLC, IHLC and PHLC subscales of the MHLC, PCS subscale of the SF-36 and the disability, harm, emotion, solicitude, medical cure and medication subscales of the SOPA-35 (p > 0.05) (Table II). Significant differences were found for fatigue intensity (p = 0.02), showing less fatigue intensity for continuers 6.48 (2.15) than for early 6.87 (2.4) and late 6.93 (2.14) drop-outs. The anxiety subscale of the HADS was also significant (p = 0.04): continuers showing less anxiety 11.37 (4.19) compared with early 12.5 (4.22) and late 12.12 (1.14) drop-outs. A significant effect was found for the MSC subscale of the SF-36 (p = 0.001), demonstrating that continuers had a better mental quality of life 29.60 (12.66) than early 25.7 (13.23) and late 26.19 (12.18) drop-outs. Only the “perceived control” subscale of the SOPA-35 differed statistically across groups (p = 0.03), showing that early 5.9 (4.93) and late 6.59 (4.11) drop-outs had less perceived control than continuers 7.23 (4.06).
Table II. Mean and standard deviation (SD) or median and 1st and 3rd interquartile ranges (IQR) for non-normal distribution of the 18 variables measured at baseline. Early drop-outs: patients who never started the treatments; late drop-outs: patients who attended to < 6 sessions out of 9; continuers: patients who completed the treatments
Multiple logistic regression analyses
An 8-predictor logistic model was fitted to the data to test the research hypothesis regarding the likelihood of dropping out of a pain management programme (Table III). Concerning late drop-outs, only the educational level was statistically significant: intermediate educational level (p = 0.002) and high educational level (p = 0.005) protected against dropping out during treatment. Regarding early drop-outs, educational level was a significant protector, but only for the intermediate level (p = 0.04). Delay in onset of treatment was significant (p = 0.001), meaning that a delay of more than 4 months increased the risk of not starting treatment. Randomization was also statistically significant (p = 0.009), being randomized increased the risk of not starting treatment.
Table III. Results of multiple logistic regression analysis of potential predictors for drop-out (educational level, therapist expertise, randomization, delay onset of treatment, subscale anxiety of the Hospital Anxiety and Depression Scale (HADS), Mental quality of life (MCS) of the Short Form-36 (SF-36) and subscale control of the Survey of Pain Attitude-35 (SOPA-35)). Early drop-outs: patients who never started the treatments; late drop-outs: patients who attended < 6 sessions out of 9
The aim of this study was to identify the profile of patients committed to a biopsychosocial approach to pain management by considering type of drop-out. The objective was not to understand if the treatment’s efficacy would influence drop-out rates, but if a priori characteristics would have an impact. Univariate analyses yielded 8 potential predictors of drop-out, out of 18 variables eligible for inclusion in multivariate logistic regression analyses. These analyses revealed an association between patients’ educational level and all types of drop-outs, showing that an intermediate or a high educational level protects against drop-out by 0.6 (67%) and 0.6 (68%), for early and late drop-outs, respectively. Furthermore, an association was found between delay in onset of treatment and randomization for early drop-outs only. This means that a delay longer than or equal to 4 months increases the risk of never attending the first session of treatment by 0.02 (25%). The fact of being randomized in any of the treatment groups increases the risk of never attending the first session of treatment by approximately 134%.
Given the scarcity of studies focusing on drop-out from chronic pain treatments and the similarities between treatments for chronic pain and psychological disorder (e.g. anxiety and addiction), this discussion will sometimes rely on the literature regarding patients with psychological disorders.
A recent meta-analysis highlighted that scientific literature about drop-out in chronic pain is controversial (5). Depending on the studies, associations between drop-out rates and various socio-demographics, such as age, sex, occupational status, convention and aetiologies, are conflicting, and do not allow us to consider them as real predictors (5). In the current study, none of these variables were significantly associated with drop-out, potentially because they display rather inconsistent associations with drop-out throughout the literature and are, consequently, not acknowledged as predictors of drop-out. Furthermore, to our knowledge, the SF-36 subscales, SOPA-35 subscales and MHLC subscales, and PDI and ISI scores have not been investigated as potential predictors in other studies, making it difficult to compare the current results with other studies. Even though no statistical significance was found, drop-outs vs continuers had higher scores in anxiety (12.22 (4.15) vs 11.37 (4.19), respectively) and depression (10.2 (4.22) vs 9.55 (4.43), respectively), in the Insomine Severity Index (18.52 (8.56) vs 17.06 (6.81), respectively) and in the Pain Disability Index (40.27 (14.29) vs 38.12 (13.14), respectively). Subscales of the SOPA-35 also differed slightly, but did not attain significance: drop-outs had higher scores in the harm subscale (10.09 (3.91)) vs continuers (9.8 (3.95)), in the emotion subscale (12.37 (5.49)) vs continuers (11.78 (5.01)) and in the medical cure subscale (11.23 (3.42)) vs continuers (10.94 (3.22)). Drop-outs had lower scores for perceived control (6.41 (3.98)) vs continuers (7.23 (4.06)) and solicitude (8.51 (5.16)) vs continuers (9.19 (4.96)). From a clinical point of view, it is of interest to note that distressed patients may also be more likely not to complete the treatment.
Concerning socio-demographic factors, the results showed a significant association only for educational level and drop-out: drop-outs (early and late) with a low educational level tended either to never attend the first session, or to drop-out during treatment. However, other studies of drop-out predictors in chronic pain have shown that patients with a high educational level tend to be more likely to drop-out (10), or even that no link exists between education and drop-out (27). The results of a study by Oosterhaven et al. (9) were similar to the current results. Various studies have repeatedly demonstrated an association between poorer health outcomes and lower levels of education (28). One explanatory linkage is considered to be health literacy, i.e. “the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health” (29). It has been shown that low education is correlated with low health literacy skills (28). Considering this definition, it seems logical to assume that low health literacy skills are a barrier to health information, healthcare access and lower health in general (28). Low health literacy was also associated with low self-reported mental health, low self-reported physical health and low self-reported general health in healthy subjects (28). In addition, patients with low health literacy had higher scores of pain intensity and pain perception (30). Others have reported that 54% of chronic pain patients (n = 131) had low health literacy, which was associated with low educational levels and less perceived controle over pain (31). Finally, and in agreement with the current results, Hardman et al. (32) showed that low health literacy, and thus low education, was associated with higher rates of drop-out (32). As all treatments had self-management components, it would be of interest to explore how educational level is related to self-efficacy. This was not done in the current study, and therefore constitutes a limitation that should be addressed in future studies.
In the current study, the delay in onset of treatments, also termed “waiting time” by other authors (15), increased the risk of never starting treatment by 25%. One study, focusing on psychotherapy in substance abuse, showed that a prolonged delay in onset of treatment was associated with increased drop-out rates before the beginning of treatment (33) and after admission (34). A longer delay may generate second thoughts in entering the programme, alter treatment expectations, and reduce motivation to enter a treatment programme (15, 35). Unfortunately, delay in onset is often due to organizational factors, such as randomization, as was the case in this study. In a similar way to that of centralized intake units for substance abuse, an alternative for chronic pain management could be to propose “treatment before the treatment”, to patients. This “pre-treatment” could be dedicated to explaining the mechanisms related to chronic pain, the biopsychosocial model of chronic pain, and highlighting the active role that the patient needs to endorse in the management of pain.
The most notable result of this study is that being randomized in any of the treatment groups was associated with a greater likelihood of never starting treatment compared with non-randomized patients. Randomized control trials (RCT) are considered to be the “gold-standard” in evidence-based practice (36). Nevertheless, different limitations have been mentioned concerning the application of RCTs in psychological therapy (not specific to chronic pain management), one of which seems accurate within this framework: often, the patients have been referred due to information about the reputation of the lead therapist, hence they are unlikely to be blind to the treatment options (36). It is reasonable to think that one might feel less involved if one is not in the treatment programme desired initially. Furthermore, patients who are included in the decision-making process regarding treatment seem to increase their personal involvement, which maximizes the treatment effect (37–39). In other words, allowing patients to choose their treatment might alter their subjective appraisal of the treatment, and, hence, the treatment outcome, in a more positive way. We propose that personalized medicine, pragmatic trials, and qualitative studies should be promoted in clinical research. The fact that patients do not complete the proposed treatment probably impacts the multidisciplinary team, possibly diminishing their motivation in providing state-of-the-art care. To our knowledge no study has investigated this issue, and future research on this topic would be of great interest.
Clinicians should enhance health literacy especially for those patients with low educational levels. By doing so, patients would eventually be able to understand their active role in the management of their pain, which would empower them and increase treatment adherence independently of the proposed treatment. Various communication skills aim at increasing patients’ motivation and decision-making (40). For example, motivational interviewing aims at allowing patients to address ambivalence about positive behavioural changes, making it especially interesting in the management of chronic pain, as the majority of treatments aim to change maladaptive behaviours into adaptive ones (40). Prospective studies assessing drop-out should also be conducted. This study was retrospective, and therefore could not take into account all potential predictors of drop-out.
In conclusion, this study emphasizes that drop-out might not be associated with patients’ characteristics (except for education), but rather with external factors inherent to the application of evidence-based practice. The results show that randomization increases the risk of never attending the treatment sessions. In order to overcome this deleterious effect, researchers should rely on pragmatic, quasi-experimental, and observational trials, as well as qualitative studies to complement more classical RCTs.
The study was supported by the University and University Hospital of Liège, “Plan National Cancer” of Belgium (grant numbers 138 and 139), Cancer Foundation of Belgium, and Benoit Foundation (Bruxelles). Observational, case-control Clinical trial number: NCT04218227.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize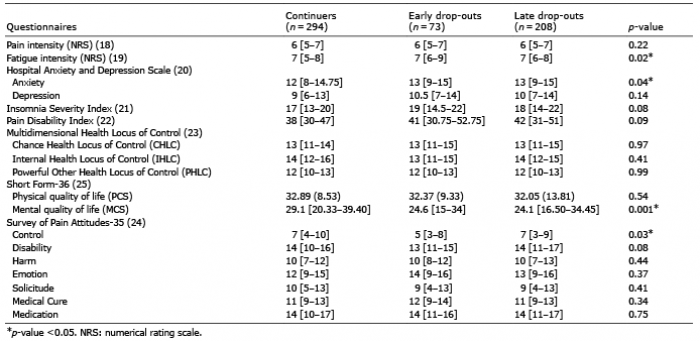 Click to show fullsize
Click to show fullsize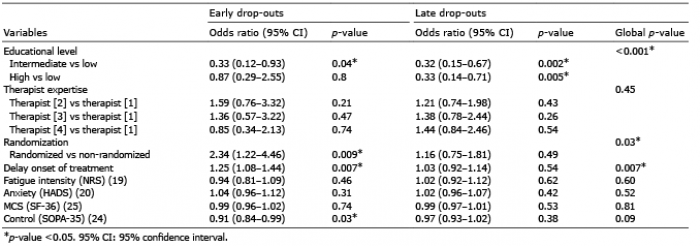 Click to show fullsize
Click to show fullsize