
From the 1Department for Rehabilitation and Secondary Prevention, 2Laboratory for Cardiac Rehabilitation, Federal State Budgetary Institution “National Medical Research Centre for Preventive Medicine” of the Ministry of Healthcare of the Russian Federation, 3Federal State Budgetary Institution “Research Institute for Complex Issues of Cardiovascular Diseases”, 4Moscow Department of Public Health Moscow Center for Research and Practice in Rehabilitation, Restorative and Sports Medicine, Moscow, Russian Federation, 5Laboratory for Rehabilitation ,Federal State Budgetary Institution “Research Institute for Complex Issues of Cardiovascular Diseases”, Kemerovo and 6Federal State Budgetary Educational Institution of Higher Education “Altay State Medical University” of the Ministry of Health of the Russian Federation, Barnaul, Russian Federation
Objective: To measure progress towards introducing a 3-phase rehabilitation programme, based on the multidisciplinary approach, for patients with cardiovascular diseases.
Methods: Seventeen hospital and outpatient medical centres from 13 regions of the Pilot Project. Baseline questionnaires assessed the involvement of multidisciplinary teams, staffing, and the equipment in healthcare facilities. These questionnaires covered 3 rehabilitation phases: inpatient rehabilitation in the intensive care units and departments of myocardial infarction/cardiac surgery; early in-hospital rehabilitation; and outpatient rehabilitation.
Results: The pilot project was initiated in 2013. At the 5-year follow-up, phase I was established across all 17 sites, phase II at 13 sites, and phase III at 9 sites. By 2017, multidisciplinary teams were deployed to manage patients at all sites. Early rehabilitation in regional vascular centres, reduced patients’ stay from 13.7 (2.1) days in 2013 to 7.6 (1.1) days in 2017.
Conclusion: Despite successful implementation of the 3-phase rehabilitation programme based on the multidisciplinary approach, further improvement is required, with the main focus shifted to patients routing between healthcare facilities. Particular attention should be paid to the standards for providing phase III cardiac rehabilitation, in order to ensure continuity of cardiac rehabilitation. The next step should include assessment of the effectiveness of the implemented cardiac rehabilitation programme and its translation to other regions of the country.
Key words: cardiac rehabilitation; cardiovascular disease; myocardial infarction.
Accepted Apr 8, 2021; Epub ahead of print Apr 19, 2021
J Rehabil Med 2021; 53: jrm00186
Correspondence address: Svetlana Pomeshkina, Laboratory for Rehabilitation, Federal State Budgetary Institution “Research Institute for Complex Issues of Cardiovascular Diseases”, Kemerovo, Russian Federation. E-mail: swetlana.sap2@mail.ru
Doi: 10.2340/16501977-2833
Within the 5-year follow-up, we evaluated the implementation of a three-phase rehabilitation programme based on the multidisciplinary approach for patients with cardiovascular diseases in 17 healthcare institutions located in 13 cities of the Russian Federation. By the end of 2017, phases 1 and 2 cardiac rehabilitation fully corresponded to the main principles stated in the Russian clinical guidelines. All patients underwent educational sessions and physical exercise. The implementation of phase 3 cardiac rehabilitation proved to be the most difficult one to implement as it required the establishment of separate outpatient cardiac rehabilitation departments with the necessary sports gear and specialists. Thus, further improvement of rehabilitation programs is necessary. Special attention needs to be focused on the standards and principles of providing phase 3 cardiac rehabilitation followed by the introduction of the three-phase cardiac rehabilitation in other regions of the country.
Cardiac rehabilitation is the well-known standard of care in today’s cardiology. Randomized clinical trials and meta-analyses have proved the efficacy of cardiac rehabilitation, and its beneficial effects on reducing morbidity and mortality in patients with atherosclerosis. Recent evidence supports cardiac rehabilitation as a class I recommendation with level of evidence A in the guidelines (1). The Cardiac Rehabilitation Outcome Study (CROS) meta-analysis (Cardiac Rehabilitation Outcome, n = 219,702, a 40-month follow-up) showed that multi-component rehabilitation resulted in a decreased risk ratio of mortality in the early interventional period in patients with acute coronary syndrome (ACS) who were taking statins (2). A 2016 Cochrane review (63 studies, n = 14,486 participants) found benefits of exercise-based rehabilitation for patients with coronary artery disease (CAD) in reducing cardiovascular mortality (27 studies, risk ratio 0.74, 95% confidence interval (95% CI) 0.64–0.86) and hospital readmissions (15 studies, risk ratio 0.82, 95% CI 0.70–0.96) compared with the controls (3).
In the Russian Federation, over 500,000 patients have ACS annually, approximately 40,000 undergo coronary artery bypass grafting (CABG), and 200,000 undergo percutaneous coronary intervention (PCI) annually (4). Most of these patients should be referred for cardiac rehabilitation. However, introduction of the cardiac rehabilitation programme is limited by a lack of healthcare facilities, lack of financial support, and a shortage of trained personnel, since cardiac rehabilitation services have not yet been modified to address all patients’ needs.
In 2014 the Russian Society of Cardiosomatic Rehabilitation and Secondary Prevention (RSCSR), Russian Society of Cardiology (RSC), and Russian Union of Rehabilitation (RUR) presented Russian clinical guidelines for acute ST segment elevation myocardial infarction (STEMI) “Acute STEMI: rehabilitation and secondary prevention”, and in 2016 the RSCSR/Association of cardiovascular surgeons (RACVS)/RSC/RUR developed the Russian clinical guidelines “Coronary artery bypass grafting in patients with coronary artery disease: rehabilitation and secondary prevention” (5, 6). These guidelines introduced a concise framework of cardiac rehabilitation delivery and propose its main principles: multiple phase structure, consistency, continuity, and multidisciplinary care provision. Integration of the multidisciplinary team ensures a patient-centred approach to address all patient’s needs. Russian cardiac rehabilitation consists of 3 phases:
Therefore, the National Medical Research Centre for Preventive Medicine and RSCSR initiated the first nationwide pilot project on developing rehabilitation services for patients with cardiovascular diseases (CVD) in 2013.
The aim of the current study is to measure progress towards introducing the 3-phase rehabilitation programme based on the multidisciplinary approach for patients with cardiovascular diseases.
Rehabilitation Services for Patients with Cardiovascular Diseases Pilot Project
A total of 17 healthcare institutions in 13 cities of the Russian Federation (i.e. Barnaul, Voronezh, Ivanovo, Kemerovo, Krasnoyarsk, Moscow, St Petersburg, Samara, Saratov, Ufa, Cheboksary, Chelyabinsk, and Yakutsk) agreed to participate in the pilot project and were enrolled in 2013. The follow-up period was 5 years. Novel rehabilitation services were provided to patients with CAD using a single protocol, based on national and European guidelines (5–8).
All healthcare institutions participating in the pilot project were mentored by experts from the National Medical Research Centre for Preventive Medicine (NMRCPM) and Russian Society of Cardiosomatic Rehabilitation and Secondary Prevention (RSCSR) and counselled during the implementation of the 3-phased cardiac rehabilitation for patients with acute myocardial infarction (AMI) and those who underwent PCI or CABG. All health professionals in the multidisciplinary rehabilitation teams underwent additional training, with a particular focus on the main rehabilitation principles, the role of physical and psychological patient education, and counselling. All in-site changes were managed remotely, with several interactive on-site educational sessions at each participating site. Each healthcare institution was supervised by a local expert who coordinated and managed the introduction of cardiac rehabilitation with the NMRCPM.
The recommended rehabilitation phases, their duration, the number of patients referred to cardiac rehabilitation, the staffing level, the need for equipment, and the comprehensiveness of this programme were analysed.
Multidisciplinary rehabilitation team
Cardiac rehabilitation was delivered by multidisciplinary teams, consisting of cardiologists, cardiac surgeons, clinical psychologists, specialists in rehabilitation medicine (physiatrist), exercise coaches, and nurses. All specialists were certified and trained.
The cardiologist was responsible for prescribing medical therapy, arranging a rehabilitation plan and its duration, informing the patient about cardiovascular risk factors, managing their modification, and explaining the importance of a healthy lifestyle. The cardiologist coordinated the rehabilitation team. The physiatrist was responsible for restoring functional capacities and treating injuries. This specialist focused on exercise therapy as a main rehabilitation component and wrote exercise prescriptions according to stress testing and calculated intensity level. The physiatrist evaluated patients’ eligibility for cardiac rehabilitation, considered their preferences, improved their motivation, assessed the effectiveness and safety of the prescribed programme according to the clinical and instrumental data (heart rate (HR), Borg’s perceived exertion scores, electrocardiography (ECG), etc.). The exercise coach supervised exercise sessions, and conducted activity education concealment. The physiatrist supervised the exercise coach.
Cardiac rehabilitation programme
Individual counselling and medical gymnastics were started at phase I in the ICU and MI departments. Referral of patients to the next rehabilitation phase was generally determined by their rehabilitation potential: patients with MI with low and moderate rehabilitation potential were referred to phase II, and those with high rehabilitation potential were referred to the outpatient phase III.
The main elements of cardiac rehabilitation commonly include (5, 6):
By the end of phase I, all patients should have been referred to undergo CE-test screening to calculate personal power threshold and to measure the optimal exercise intensity before starting phase II rehabilitation. The intensity was calculated according to the patient’s functional capacity. Phase II rehabilitation patients participated in exercise training sessions every day under the supervision of the physiatrist in the inpatient phase. Patients in the outpatient centre-based exercise training programmes participated in 3 exercise training sessions (45–60 min) per week for 6 months. The physiatrist monitored their clinical state at the beginning of the session and during it (complaints, blood pressure measurement, heart rate, exercise resistance). Exercise training sessions were guided by the physiatrist. After the centre-based cardiac rehabilitation patients were referred to the home-based exercises (3–4 sessions per week, with a mean duration of 30–40 mins) under the remote control of the cardiologist up to one year (phone calls and, if required, hospital visits). Patients were instructed to perform a self-assessment of their physical well-being at home.
Statistical analysis
Statistical analysis was performed using the SAS software package (Statistical Analysis Systems, SAS Institute,Cary, North Carolina, USA). The Kolmogorov–Smirnov test was used to assess the normal distribution of quantitative variables. Quantitative variables are presented as the mean group value (M) and the standard deviation (SD) of the mean. A p-value of < 0.05 was considered statistically significant.
Rehabilitation Services for Patients with Cardiovascular Diseases Pilot Project
While introducing phase I rehabilitation for cardiac patients, 7 sites did not have cardiologists who were trained in rehabilitation in 2013. The cardiac rehabilitation programme in those sites was led by cardiologists who were not trained in cardiac rehabilitation. By the end of 2017, all multidisciplinary teams in 17 sites were coordinated by trained cardiologists. By 2017, all sites had employed physiatrists and exercise coaches.
In 2013, clinical psychologists and psychotherapists were not employed in the participating centres. In 2017, the rehabilitation teams comprised 30% psychotherapists and 70% clinical psychologists.
At the 5-year follow-up, phase I cardiac rehabilitation had been successfully incorporated into routine clinical practice for core patients, particularly those with MI, in the ICUs and departments of MI/cardiac surgery. For ICU patients with MI, 64% received early cardiac rehabilitation in 2013. The introduction of cardiologists enabled the enrolment of all core patients in the early rehabilitation programme. By the end of 2017, 100% of patients underwent routine early cardiac rehabilitation. At the beginning of 2013, 74% of patients with MI were transferred to the Cardiology Department and 36% to the Department of Internal Medicine. By the end of 2013, 54% of patients were transferred to the specialized Departments of MI, 36% to the Cardiology Department, and only 10% to the Department of Internal Medicine. In 2017 all patients with AMI were transferred to the core Departments of MI in the vascular centres. Importantly, no patients were transferred from the ICU to non-core therapeutic departments, which may be considered as a beneficial effect of timely routing of the patient.
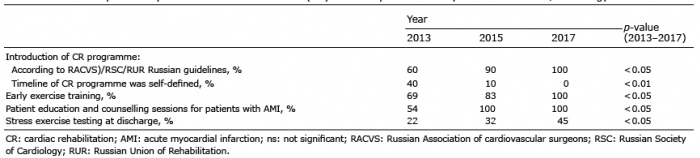
Upon transfer of patients to the Department of MI/Cardiology to continue phase I cardiac rehabilitation, the focus shifted to optimization of the cardiac rehabilitation programme and patient education (Table I). By the end of 2017, the phase I rehabilitation programme in all sites corresponded fully to that recommended by the Russian clinical guidelines. All patients participated in educational sessions and underwent exercise training. The number of stress tests increased by 23% (22% in 2013).
Early rehabilitation reduced the mean length of stay in the ICU from 4.3 (0.4) days at the start of 2013 to 1.9 (0.1) days in 2017 (p < 0.05). Early cardiac rehabilitation reduced the mean length of stay of patients with AMI in the departments of MI/cardiac surgery, from 12.7 (2.6) days at the beginning of 2013 to 6.6 (1.3) days in 2015 (p < 0.05) and to 5.7 (1.1) days in 2017 (p < 0.01). The total in-hospital stay for patients with AMI in ICU plus the departments of MI/cardiac surgery (phase I cardiac rehabilitation) mean (standard deviation (SD)) decreased from 16.8 (SD 2.4) days (length-of-stay range 10.2 to 19.6 days) at the start of 2013 to 9.1 days (SD 1.8) (length-of-stay range 6.1 to 12.1 days, p < 0.05) in 2015 and 7.6 days (SD 1.1) (length-of-stay range 5.2 to 10.5 days, p < 0.01) in 2017.
Table I. Results of phase I inpatient cardiac rehabilitation (CR) in the Department of Myocardial Infarction/Cardiology
The proportion of patients transferred from phase I to phase III cardiac rehabilitation was 27% in 2013 and 22% in 2017. The proportion of patients referred from phase I to phase II cardiac rehabilitation was 73% in 2013 and 78% in 2017.
Phase II cardiac rehabilitation programme was improved according to the Russian clinical guidelines (Table II).
In 2013, only 4 sites had separate rehabilitation departments for early rehabilitation of patients in hospitals (phase II cardiac rehabilitation). This number increased in 2015 (10 sites). In 2017, all 17 sites delivered rehabilitation services in these departments. The initiation of phase II cardiac rehabilitation for each patient required the participation of the whole multidisciplinary rehabilitation team. All of the cardiologists and physiatrists were employed in the sites to provide phase II cardiac rehabilitation. the proportion of clinical psychologists and psychotherapists in the multidisciplinary team and psychotherapists in the multidisciplinary team increased from 81% and 73% in 2015 to 89% and 80% in 2017, respectively. In 2013, there was a lack of cardiac rehabilitation equipment (treadmills, cycle ergometers) at 7 sites. By the end of 2017, all sites were equipped with the required sports equipment.
The mean length of stay for patients in the Department of Early Rehabilitation (phase II cardiac rehabilitation) was similar in 2013 and 2017 (16.6 (2.1) days and 16.7 (2.1) days, respectively).
However, a far greater challenge was the development of phase III cardiac rehabilitation, as it required separate cardiac rehabilitation departments with the necessary equipment and trained personnel in the outpatient settings. This cardiac rehabilitation phase was commonly replaced by ineffective outpatient examinations performed by general practitioners with regular referrals to cardiologists.
All sites participating in the RSCD Pilot Project faced some difficulties while establishing phase III cardiac rehabilitation. Only 9 sites provided phase III cardiac rehabilitation to patients with AMI in 2017, compared with 2 sites in 2013. All sites had all the necessary sports equipment, recruited all the specialists required, and provided cardiac rehabilitation fully consistent with Russian clinical guidelines.
Table II. Results of phase II cardiac rehabilitation (CR) in the in-hospital department of early rehabilitation
Patients with MI need to undergo cardiac rehabilitation programmes in order to address all major concerns (10). An inverse relationship between participation in at least one phase of cardiac rehabilitation and its positive effects on the outcomes has been shown in over 30,000 patients after CABG. A 4-year risk of MI and death decreased by 14% and 47% in those patients who underwent 36 exercise sessions compared with those who attended 24 exercise sessions. Patients who participated in one exercise session had a 31% increased risk of MI compared with the rest. Eighteen percent of patients were fully adherent with the cardiac rehabilitation and underwent all 36 exercise sessions (11).
Despite the importance of each specific phase of cardiac rehabilitation with a multidisciplinary approach, they are only part of the 3-phased cardiac rehabilitation, and, separately, will not be sufficiently effective in the absence of continuity between all stages of the system.
The nationwide pilot project reported the possibility of introducing exercise rehabilitation and comprehensive cardiac rehabilitation in different regions of the Russian Federation. The number of rehabilitation teams and the personnel included in these teams had increased by the end of the study. The physiatrist plays a key role in the whole multidisciplinary team. This specialist writes exercise prescriptions in the cardiac rehabilitation programme individuated to a patient according to the diagnosis and screening results. The physiatrist supervises exercise workouts and explains to patients the accepted HR for safe and effective training. During rehabilitation, the physiatrist performs serial measurements of the target physical activity according to exercise tolerance, a 6-minute walk test, and other factors that may affect physical activity level.
The best results regarding the establishment and improvement of cardiac rehabilitation for patients with AMI were obtained for phase I inpatient rehabilitation in the ICUs and departments of myocardial infarction/cardiac surgery. By 2015, participating sites stopped transferring patients with AMI to non-core therapeutic departments. Moreover, the length of stay of patients with AMI was reduced further in phase I cardiac rehabilitation. This is directly related to the opportunity to refer patients with AMI to phase II and phase III rehabilitation (for patients with high rehabilitation potential).
Finally, the significant role of multidisciplinary rehabilitation teams was demonstrated in the management of patients with AMI. At the same time, all hospitals typically developed a sensitive monitoring system for patients enrolled in phase II cardiac rehabilitation. At the 5-year follow-up, the proportion of patients who underwent phase II cardiac rehabilitation increased significantly.
There are still no uniform standards for delivering phase III cardiac rehabilitation in outpatient settings. Despite the fact that phase I and II cardiac rehabilitation has been successfully introduced in the clinical practice, phase III cardiac rehabilitation requires additional measures for its implementation. Only 9 sites recruited to the pilot project were able to establish separate outpatient cardiac rehabilitation units and provide long-term cardiac rehabilitation according to the national guidelines. This issue should be addressed by the regional government in order to help hospitals overcome all possible barriers, including financial and managerial support.
Study limitations
Long-term evaluation of cardiac rehabilitation clinical effectiveness is required. The optimal period for long-term evaluation in patients with atherosclerosis is considered to be at least 5 years. Despite the fact that the early success of the pilot project did not translate into a wider endorsement by the regional cardiology communities, we hope that a novel cardiac rehabilitation will be introduced in all regions following the long-term evaluation.
Despite successful implementation of the 3-phase rehabilitation programme based on the multidisciplinary approach, further improvement in the programme is required, with the main focus shifted to patients routing between the healthcare facilities. Particular attention should be paid to the standards for providing phase III cardiac rehabilitation, in order to ensure continuity of cardiac rehabilitation. The next step should include assessment of the effectiveness of the implemented cardiac rehabilitation programme and its translation to other regions of the country.
Funding.This work was supported by National Medical Research Centre for Preventive Medicine of the Ministry of Healthcare of the Russian Federation (115072340037).
RSCD-Pilot investigators. Barnaul: Lomteva EV, Starkova LA, Chtyreva TV; Cheboksary: Karpova AV; Chelyabinsk: Sprikut АА, Tkacheva АG, Ilyanykh DL, Karaulovskaya NN; Ivanovo: Andreev АG, Belova VV, Mishina IE, Dovgaluk YuV, Sukhanova DS; Krasnoyarsk: Lisnyak ЕА, Nikulina SYu, Ustyugov SА, Chernova AA; Moscow Region: Ivanov ЕV, Sukhinina IS; St Petersburg: Karpukhin АV, Misyura ОF, Aleksandrov PV, Gorunova AA, Zobenko IA, Perepech NB; Samara: Lebedev PА, Mischenko ОV; Saratov: Karpov ES, Kotelnikova EV; Voronezh: Belov VN, Ostroushko NI; Ufa: Karamova IМ, Abdukova ER, Gazizova NR, Petruchkin; Yakutsk: Kyblanova ЕS, Sidorov АS, Nikonorov VN.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize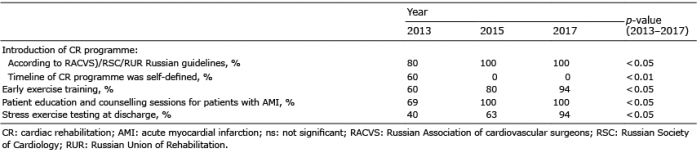 Click to show fullsize
Click to show fullsize